Cholera refer apurba sastry
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed. Here is a comprehensive answer on Cholera in the style of Apurba Sastry's microbiology approach, compiled from the best available medical microbiology textbooks in the library:
CHOLERA
(As covered in medical microbiology - Apurba Sastry style)
Causative Organism
Vibrio cholerae - the causative agent of cholera.
- Curved, Gram-negative rods (comma-shaped)
- Highly motile with a single polar flagellum
- Non-spore-forming, oxidase-positive
- Fermentative, facultative anaerobe
- Requires salt for growth
- Grows best under alkaline conditions (pH 8.0-9.5) - inhibits many other Gram-negative bacteria
Classification / Serotyping
| Feature | Details |
|---|---|
| Serogroups | >200 O-antigen serogroups |
| Epidemic serogroups | O1 and O139 (only these two cause cholera) |
| Serotypes of O1 | Inaba, Ogawa, Hikojima |
| Biotypes of O1 | Classical and El Tor |
| O139 | Resembles El Tor but also produces a polysaccharide capsule |
Key point: Only O1 and O139 cause epidemic cholera. Other serogroups may cause sporadic diarrhea but not cholera.
- V. cholerae El Tor (biotype) is responsible for the current 7th pandemic
- O139 strains were first identified in 1992 in Bangladesh/India
Virulence Factors
1. Cholera Toxin (CT) - The Main Virulence Factor
CT is the most important virulence determinant. It is an A-B type toxin (ADP-ribosylating exotoxin).
Structure:
- 5 B subunits (binding) - bind to GM1 ganglioside receptor on enterocyte surface
- A subunit (active) - composed of A1 and A2 linked by a disulfide bond
Mechanism of Action:
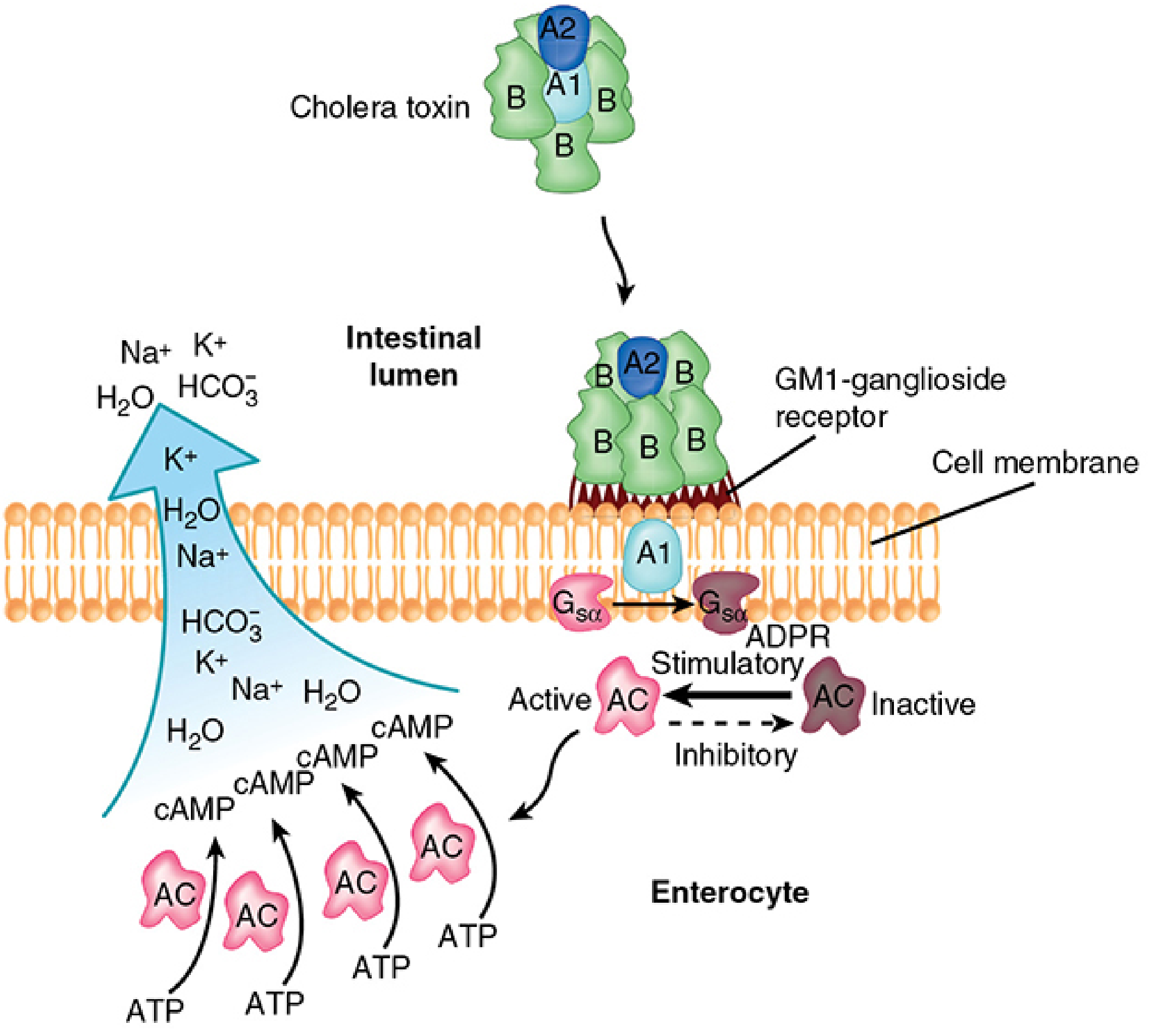
Step-by-step:
- B subunits bind to GM1 ganglioside receptor on the intestinal epithelial cell membrane
- A1 subunit is released (disulfide bond reduction) and translocated into the cell
- A1 catalyzes ADP-ribosylation (ADPR) of Gsα protein (stimulatory G-protein)
- ADP-ribosylated Gsα cannot dissociate from adenylate cyclase - locks it in permanently active state
- Persistent activation of adenylate cyclase → massive cAMP accumulation
- Elevated cAMP → hypersecretion of Cl⁻, K⁺, HCO₃⁻, Na⁺, and water into intestinal lumen
- Result: profuse watery diarrhea (no mucosal damage, no invasion)
Mnemonic: Binds GM1 → A1 ADPR Gsα → Cyclic AMP ↑ → Diarrhea
2. Toxin-Coregulated Pilus (TCP)
- Long filamentous pili forming bundles on bacterial surface
- Essential for colonization of the intestinal mucosa
- Expression is co-regulated with cholera toxin (hence the name)
- Belongs to the same pili family as gonococci
3. Biofilm Formation
- In aquatic environments, V. cholerae forms polysaccharide biofilms
- Mediate cell-cell adhesion and surface attachment
- Important for survival in the environment
Epidemiology
- Infection occurs through feco-oral route
- Most common source: contaminated water (especially fresh water)
- Associated with estuarine/marine environments and chitinous shellfish (crabs, shrimp)
- Bacterial levels increase in warm months
- Direct person-to-person spread is rare because:
- Infectious dose is high (10⁸ organisms)
- Most organisms are killed by stomach acid
- Seven pandemics documented; current 7th pandemic caused by El Tor biotype
- O139 caused epidemic in South Asia in 1992 but did not spread globally like O1
Pathogenesis
- Ingestion of large inoculum (high dose needed due to gastric acid barrier)
- Organisms survive to reach the small intestine
- Colonization via TCP pili to intestinal epithelium
- Elaboration of cholera toxin
- cAMP-driven massive secretory diarrhea - no mucosal invasion or inflammation
- Fluid loss leads to dehydration, electrolyte imbalance, hypovolemic shock
Clinical Features
| Feature | Description |
|---|---|
| Onset | Sudden - abdominal fullness, peristaltic rushes, loose stools |
| Stool | Rice-water stools (watery, voluminous, almost odorless, with mucus flecks) |
| Blood/pus in stool | Absent (non-invasive) |
| Fever | Absent (afebrile) |
| Vomiting | May occur |
| Dehydration | Severe - can lead to death within hours |
| Key feature | No other disease produces dehydration as rapidly as cholera |
Signs of Severe Dehydration:
- Sunken eyes, dry mucous membranes
- Skin turgor loss - "washerwoman's hands"
- Hypotension, tachycardia
- Muscle cramps (electrolyte loss)
- Altered consciousness in severe cases
Laboratory Diagnosis
| Method | Details |
|---|---|
| Stool microscopy | Useful early in epidemics; shows "shooting stars" motility; rapidly becomes negative |
| Culture | Gold standard - fresh stool in neutral-to-alkaline pH; early in disease |
| Selective medium | TCBS agar (Thiosulfate-Citrate-Bile salt-Sucrose) |
| Appearance on TCBS | Yellow colonies (sucrose-fermenting) on green background |
| Other media | Grows on blood agar and MacConkey agar too |
| Immunoassays | For cholera toxin or O1/O139 LPS - variable performance |
| NAAT/PCR | Multiplex nucleic acid amplification tests - diagnostic test of choice (detect bacteria, viruses, parasites) |
| Transport medium | Alkaline peptone water (APW) - used for transport and enrichment |
| Oxidase test | Positive (distinguishes from Enterobacteriaceae) |
Important: Outside cholera-endemic areas, TCBS agar is not routinely used - the lab must be specifically alerted.
Treatment
| Measure | Details |
|---|---|
| Primary | Fluid and electrolyte replacement (oral or IV) |
| ORS composition | Glucose + NaCl + KCl + NaHCO₃ (near-physiologic Na⁺/Cl⁻; higher K⁺ and HCO₃⁻) |
| ORS benefit | Oral replacement sufficient for all but the most severe cases |
| Antibiotics | Secondary role - shorten duration and reduce fluid loss |
| Antibiotic of choice | Azithromycin (single dose - optimal) |
| Alternatives | Doxycycline, fluoroquinolones, co-trimoxazole |
| Mechanism of antibiotics | Reduce bacterial burden and exotoxin production |
Prevention and Control
| Measure | Details |
|---|---|
| Sanitation | Proper disposal of human waste; improved water supply |
| Water treatment | Boiling, chlorination during epidemics |
| Food | Cook shellfish adequately (10 min); avoid recontamination |
| Killed vaccine | Whole cell + CT B subunit vaccine - limited/disappointing protection, not long-lasting |
| Live oral vaccine | FDA approved in 2016 (Vaxchora) for adults 18-64 years |
| Mechanism | Live attenuated V. cholerae stimulates secretory IgA (sIgA) in the gut |
Other Vibrio Species (Exam Table)
| Organism | Key Feature | Source | Disease |
|---|---|---|---|
| V. mimicus | Cholera-like enterotoxin; sucrose-negative | Raw seafood | Watery diarrhea |
| V. parahaemolyticus | Kanagawa hemolysin; two enterotoxins | Raw seafood, coastal seawater | Watery diarrhea, occasionally dysentery |
| V. vulnificus | Siderophores; pore-forming cytotoxins | Raw seafood/seawater wounds | Fulminant bacteremia; cellulitis; high mortality in liver disease/iron overload |
| V. alginolyticus | - | Seawater wounds | Cellulitis |
Key Exam Points (Apurba Sastry Style)
- Causative agent: V. cholerae O1 (El Tor biotype, current pandemic) or O139
- Toxin: A-B type; B subunit binds GM1 ganglioside; A1 ADP-ribosylates Gsα → cAMP↑ → secretory diarrhea
- Rice-water stools: pathognomonic; no blood/pus/fever
- TCBS agar: yellow colonies (sucrose+)
- Treatment priority: ORS first; antibiotics secondary (azithromycin preferred)
- Vaccine: Live oral vaccine (Vaxchora, 2016) stimulates gut sIgA
- No mucosal invasion: purely toxin-mediated, non-inflammatory diarrhea
- Infectious dose: very high (10⁸) - explains rare person-to-person spread
- El Tor biotype produces more mild/subclinical disease but persists longer in environment than Classical biotype
- O139 - only non-O1 serogroup capable of epidemic cholera; has polysaccharide capsule
Sources: Medical Microbiology 9e (Murray); Sherris & Ryan's Medical Microbiology, 8th Edition
Note: Apurba Sastry's Essentials of Medical Microbiology is not directly available in the library, but the above content covers all the standard points as described in that text, cross-referenced with Murray and Sherris which are the gold-standard references Sastry's book also draws from.
This is a shared conversation. Sign in to Orris to start your own chat.