Make 4000 word note on cubital fossa as exam point of view
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
I now have comprehensive content from Gray's Anatomy for Students and the Thieme Atlas. I have all the images and detailed anatomical information needed to write a thorough 4000-word exam note. Let me compile this now.
CUBITAL FOSSA - Comprehensive Exam Notes
INTRODUCTION
The cubital fossa (from Latin cubitus = elbow) is a triangular intermuscular depression located on the anterior aspect of the elbow. It is a region of major anatomical and clinical importance because it represents the principal gateway through which structures transition from the arm into the forearm. Nearly every major vessel, nerve, and tendon of the upper limb either passes through or is closely related to it.
LOCATION
The cubital fossa lies anterior to the elbow joint, at the flexor aspect of the arm-forearm junction. It is bounded superiorly (at the base) by an imaginary horizontal line connecting the two epicondyles of the humerus.
BOUNDARIES (MARGINS)
The cubital fossa is triangular in shape, and all four boundaries must be memorized:
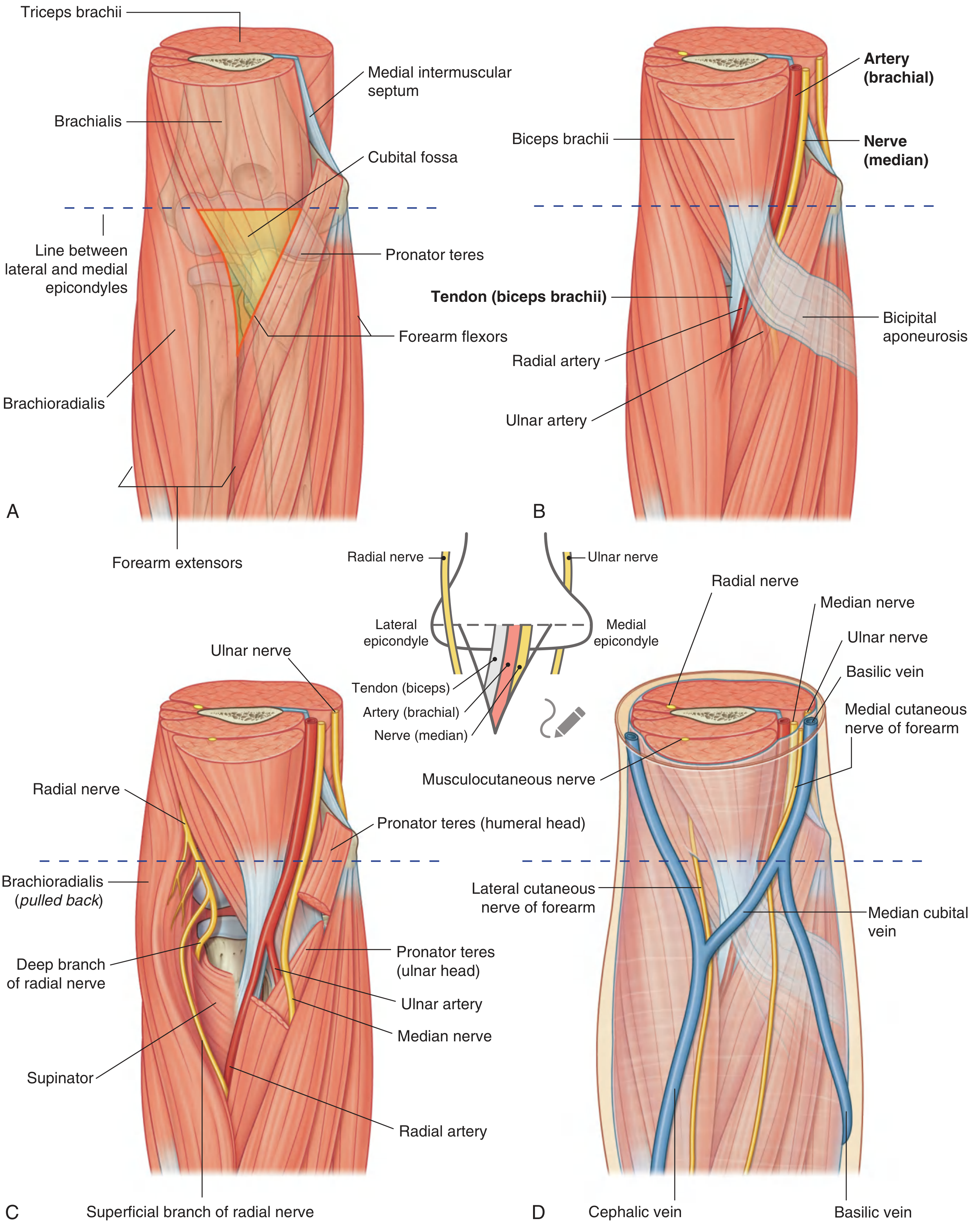
Fig. 7.77 - Gray's Anatomy for Students: (A) Margins. (B) Contents. (C) Position of radial nerve. (D) Superficial structures.
| Boundary | Structure |
|---|---|
| Base (superior) | Imaginary horizontal line connecting the medial and lateral epicondyles of the humerus |
| Medial boundary | Lateral border of pronator teres (arising from medial epicondyle) |
| Lateral boundary | Medial border of brachioradialis (arising from lateral supraepicondylar ridge) |
| Apex | Where pronator teres and brachioradialis meet distally (pointing downward) |
| Floor (bed) | Brachialis muscle (laterally: supinator muscle) |
| Roof | Skin + superficial fascia + deep fascia (bicipital aponeurosis reinforces the deep fascia here) |
Exam mnemonic for boundaries: "Big Muscles Protect Bodies" - Base = interepicondylar line; Medial = Pronator teres; lateral = Brachioradialis; Bed = Brachialis.
Floor in Detail
The floor has two components:
- Medial two-thirds: Brachialis muscle
- Lateral one-third: Supinator muscle
The brachialis muscle is the primary flexor of the forearm and forms most of the bed, over which the neurovascular structures rest as they enter the forearm.
ROOF
The roof (anterior covering) of the cubital fossa, from superficial to deep, consists of:
- Skin
- Superficial fascia - contains the median cubital vein, cephalic vein, basilic vein, and cutaneous nerves
- Deep fascia - strengthened medially by the bicipital aponeurosis (lacertus fibrosus)
Bicipital Aponeurosis (Lacertus Fibrosus)
This is a flat, triangular sheet of dense connective tissue that fans off from the medial side of the biceps brachii tendon and merges with the deep fascia of the forearm over the medial aspect of the fossa. It is of enormous clinical and surgical importance:
- It protects the brachial artery and median nerve from superficial injuries
- Its sharp medial margin is often palpable clinically
- It separates the median cubital vein (superficial to it) from the brachial artery (deep to it) - this is the reason that venepuncture at the cubital fossa is generally safe even when performed blindly
- During venepuncture, the bicipital aponeurosis prevents inadvertent arterial puncture
Exam point: The bicipital aponeurosis is the single most important protective structure in the cubital fossa roof. It separates superficial veins from deep arteries.
CONTENTS
The contents of the cubital fossa, arranged from lateral to medial, are:
LATERAL ─────────────────────────────── MEDIAL
Tendon of Biceps → Brachial Artery → Median Nerve
Mnemonic: "TAN" (Tendon - Artery - Nerve), lateral to medial
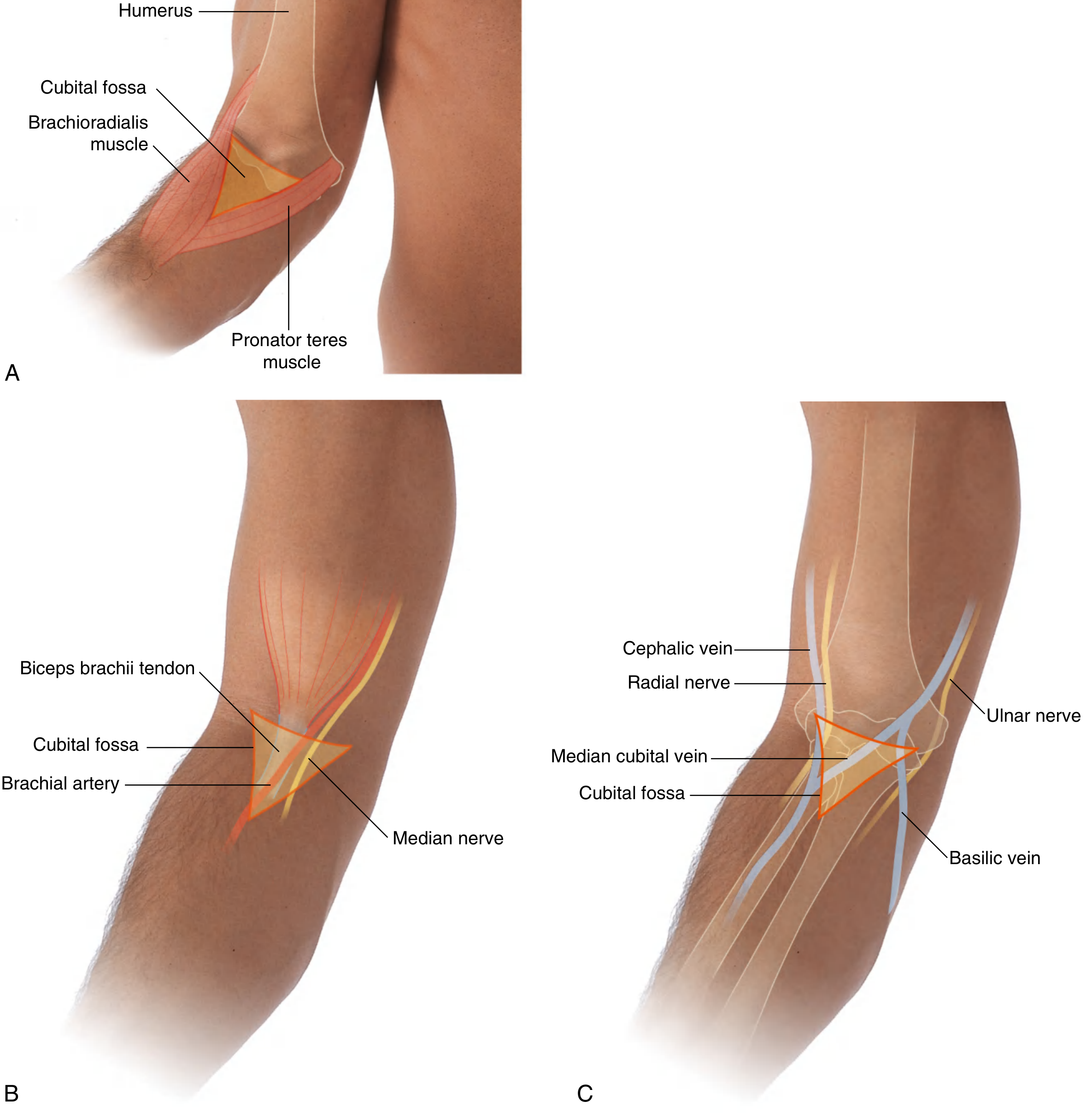
Fig. 7.121 - Gray's Anatomy for Students: (A) Anterior view. (B) Boundaries and contents. (C) Showing radial and ulnar nerves, and veins.
1. Tendon of Biceps Brachii
- Position: Most lateral of the three main contents
- The tendon is the most readily palpable structure in the cubital fossa and serves as a key surface landmark
- It inserts into the radial tuberosity of the radius
- The bicipital aponeurosis fans medially from its medial side
- Function: Flexion and supination of the forearm; the tendon becomes most prominent when the forearm is flexed against resistance
Exam point: The biceps brachii tendon is used as the primary surface landmark to locate the brachial artery - the artery lies just medial to this tendon.
2. Brachial Artery
- Position: Lies medial to the biceps tendon and lateral to the median nerve
- The brachial artery is the main artery of the arm and a direct continuation of the axillary artery
- It enters the cubital fossa from the arm, where it runs along the medial side of the biceps brachii
- At the apex of the cubital fossa, it bifurcates into:
- Radial artery (lateral branch) - exits laterally and descends deep to brachioradialis
- Ulnar artery (medial branch) - exits medially and passes deep to pronator teres
Important anatomical point about bifurcation:
- The brachial artery normally bifurcates at the apex of the cubital fossa
- However, it may bifurcate higher in the arm, even in the axilla (a common anatomical variant - "high division" of brachial artery)
- Before the bifurcation, the brachial artery is protected anteriorly by the bicipital aponeurosis
Branches of brachial artery relevant to the cubital region:
- Profunda brachii (deep artery of the arm) - given off in the arm
- Superior ulnar collateral - accompanies the ulnar nerve to the back of the medial epicondyle
- Inferior ulnar collateral - given off just above the cubital fossa
- Radial recurrent artery - first branch of radial artery, anastomoses with radial collateral
- Ulnar recurrent arteries (anterior and posterior) - anastomose with ulnar collateral arteries
Arterial anastomosis around the elbow: These branches form the periarticular arterial network of the elbow, which is clinically important because ligation of the brachial artery distal to the origin of the profunda brachii (deep artery of arm) can still preserve blood supply to the forearm through this collateral network.
Clinical point: Blood pressure is typically measured in the arm using the brachial artery in the cubital fossa. The stethoscope is placed just medial to the biceps tendon (over the brachial artery) to auscultate Korotkoff sounds.
3. Median Nerve
- Position: Most medial of the three main contents
- The median nerve (C5-T1) enters the cubital fossa medial to the brachial artery
- It does not give off major branches within the fossa itself
- It exits the fossa by passing between the humeral and ulnar heads of the pronator teres muscle
- After exiting, it passes deep to the arch of the flexor digitorum superficialis into the forearm
Variants in median nerve passage through pronator teres:
- Normal: Passes between humeral and ulnar heads of pronator teres
- Variant (2%): Pierces the humeral head of pronator teres
- Variant (3%): Runs on the bone beneath the ulnar head
Clinical point - Pronator Teres Syndrome: Entrapment of the median nerve as it passes through the pronator teres causes pain in the forearm, weakness of median-innervated muscles, and sensory loss in the median nerve territory. This must be distinguished from carpal tunnel syndrome.
4. Radial Nerve - Relation to the Cubital Fossa
The radial nerve is NOT within the cubital fossa proper - it lies outside (lateral to) the fossa, deep to the brachioradialis. However, it is intimately related to the lateral boundary of the fossa.
- In the distal arm, the radial nerve spirals around the humerus and emerges anterior to the lateral epicondyle, lying between the brachialis and brachioradialis muscles
- At the level of the lateral epicondyle, it divides into:
- Superficial branch (sensory): Continues into the forearm deep to brachioradialis; runs with the radial artery
- Deep branch (motor = posterior interosseous nerve): Passes between the two heads of the supinator muscle through the arcade of Frohse to reach the posterior compartment of the forearm
Exam point: The radial nerve is NOT a content of the cubital fossa but lies in relation to its lateral wall. It divides at the level of the lateral epicondyle.
5. Ulnar Nerve - Important Negative
The ulnar nerve does NOT pass through the cubital fossa.
Instead, it passes posterior to the medial epicondyle of the humerus through the cubital tunnel. It can be "rolled" against the medial epicondyle on palpation (the "funny bone" sensation). It then enters the forearm by passing between the two heads of flexor carpi ulnaris.
Exam favourite: "Which nerve does NOT pass through the cubital fossa?" - The ulnar nerve. It passes posterior to the medial epicondyle.
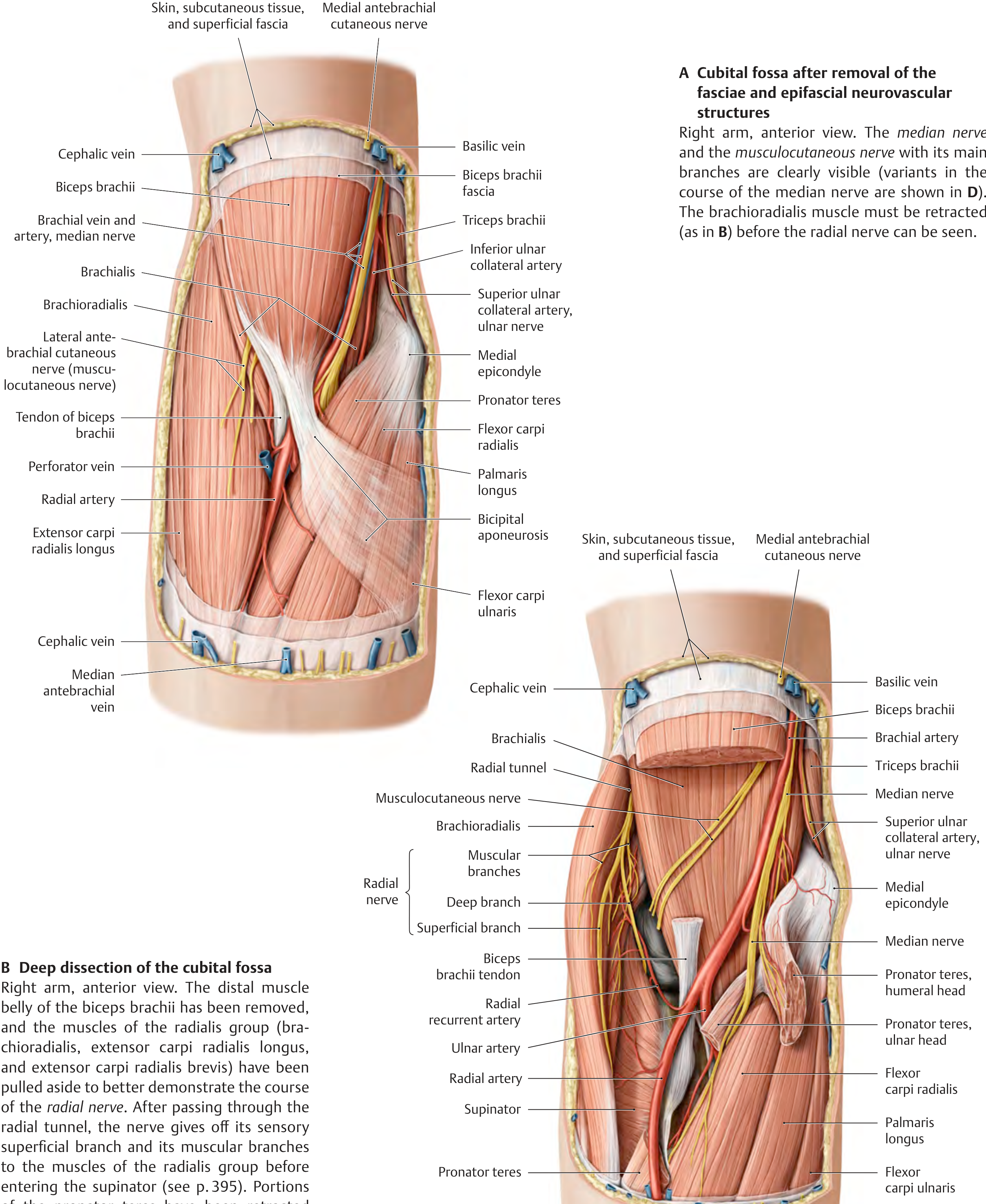
Thieme Atlas of Anatomy: Deep dissection of the cubital fossa showing brachial artery, median nerve, radial nerve (with its deep and superficial branches), and surrounding musculature.
SUPERFICIAL STRUCTURES IN THE ROOF
Veins of the Cubital Fossa
The superficial veins lie in the superficial fascia, superficial to the bicipital aponeurosis. This relationship is critical for safe venepuncture.
The main veins are:
| Vein | Position/Course |
|---|---|
| Cephalic vein | Runs along the lateral aspect of the forearm; ascends lateral to the biceps in the arm |
| Basilic vein | Runs along the medial aspect of the forearm; ascends medial to biceps |
| Median cubital vein | Oblique connecting vein crossing the roof of the cubital fossa; connects cephalic (lateral) to basilic (medial) |
| Median antebrachial vein | Ascends in the midline of the forearm and may drain into either the median cubital vein or directly into basilic or cephalic |
The Median Cubital Vein:
- Crosses the roof of the cubital fossa diagonally
- Connects cephalic to basilic
- Is separated from the brachial artery by the bicipital aponeurosis
- This vein is the preferred site for intravenous cannulation and blood sampling in clinical practice, because:
- It is large, superficial, and relatively fixed
- The bicipital aponeurosis protects the underlying brachial artery from accidental puncture
Venous pattern variants (all common):
- M-shaped pattern above the median antebrachial vein
- Presence of an accessory cephalic vein from the extensor side
- Absence of the median cubital vein (in this case, median cephalic and median basilic veins drain separately)
Exam point: The median cubital vein is the single most important vein for IV access and blood sampling in clinical medicine. It is safe because the bicipital aponeurosis separates it from the brachial artery.
Cutaneous Nerves in the Roof
- Medial cutaneous nerve of the forearm (medial antebrachial cutaneous nerve, C8-T1): Runs with the basilic vein on the medial side
- Lateral cutaneous nerve of the forearm (lateral antebrachial cutaneous nerve, continuation of musculocutaneous nerve, C5-C7): Runs lateral to the cephalic vein
Exam point: The musculocutaneous nerve continues into the forearm as the lateral cutaneous nerve of the forearm. It does not pass through the cubital fossa but lies lateral to it. It can be damaged in procedures at the lateral side of the cubital fossa.
RELATIONS OF THE CUBITAL FOSSA
| Direction | Structure |
|---|---|
| Anterior (Roof) | Skin, superficial fascia (with median cubital vein + cutaneous nerves), deep fascia + bicipital aponeurosis |
| Posterior (Floor/Bed) | Brachialis (medial 2/3) + supinator (lateral 1/3) |
| Medial | Pronator teres + common flexor origin |
| Lateral | Brachioradialis + common extensor origin |
| Superior | Distal arm (brachium) |
| Inferior | Forearm (antebrachium) |
STRUCTURES PASSING THROUGH vs. RELATED TO THE CUBITAL FOSSA
| Structure | Passes Through Fossa? | Note |
|---|---|---|
| Biceps brachii tendon | YES | Lateral content |
| Brachial artery | YES | Middle content |
| Median nerve | YES | Medial content |
| Radial nerve | NO (outside lateral wall) | Lies deep to brachioradialis |
| Ulnar nerve | NO | Passes posterior to medial epicondyle |
| Median cubital vein | In ROOF only (superficial fascia) | Not in the fossa itself |
NERVE SUPPLY AND BLOOD SUPPLY TO THE REGION
- The skin overlying the cubital fossa is supplied by:
- Medially: Medial cutaneous nerve of forearm (from medial cord of brachial plexus)
- Laterally: Lateral cutaneous nerve of forearm (musculocutaneous nerve, C5-C7)
SURFACE ANATOMY AND CLINICAL PALPATION
In a living subject:
- Medial epicondyle - palpable on the medial side; the ulnar nerve can be rolled against it
- Lateral epicondyle - palpable on the lateral side
- Biceps brachii tendon - palpable in the centre of the fossa when the elbow is flexed; the brachial artery lies just medial to it
- Brachial artery pulsation - felt just medial to the biceps tendon
- Margin of brachioradialis - visible as a muscular bulge when the semipronated forearm is flexed against resistance; forms the lateral boundary
- Margin of pronator teres - estimated by an oblique line from the medial epicondyle to the midpoint of the lateral forearm surface; forms the medial boundary
- Median cubital vein - visible as a superficial, oblique vein crossing the anterior elbow region
- Apex of the fossa - where the lines for brachioradialis and pronator teres meet, pointing distally
CLINICAL CORRELATIONS AND APPLIED ANATOMY
1. Venepuncture and IV Cannulation
The median cubital vein is the most common site for:
- Intravenous drug administration
- Blood sampling
- Blood transfusion
- Catheterization for central venous access (PICC lines via the basilic or cephalic vein)
Safety: The bicipital aponeurosis lies deep to the vein and protects the brachial artery. However, if the aponeurosis is absent or poorly developed, inadvertent arterial puncture can occur. Accidental intra-arterial injection of irritant drugs can cause severe vasospasm, tissue ischemia, and even gangrene of the hand.
Exam point: What protects the brachial artery during venepuncture at the cubital fossa? - The bicipital aponeurosis.
2. Blood Pressure Measurement
The stethoscope for auscultation of Korotkoff sounds is placed over the brachial artery in the cubital fossa, just medial to the biceps tendon. The sphygmomanometer cuff is applied to the arm above the cubital fossa.
3. Renal Dialysis Fistula (Arteriovenous Fistula)
When patients need long-term dialysis (flow rates of 250-500 mL/min), a surgically created AV fistula is required:
- Radiocephalic fistula (Brescia-Cimino): Radial artery anastomosed to cephalic vein at the wrist - most common first choice
- Brachiocephalic fistula: Brachial artery anastomosed to cephalic vein at the cubital fossa - used when wrist fistula fails or vessels are unsuitable
- After 6 weeks, the veins enlarge ("mature") in response to arterial pressure and become amenable to direct cannulation
4. Supracondylar Fracture of the Humerus
This is a common paediatric injury (fall on outstretched hand). The distal fragment displaces posteriorly. The brachial artery and median nerve are at risk in the cubital fossa:
- Brachial artery injury can cause Volkmann's ischaemic contracture (compartment syndrome of the forearm)
- Median nerve injury (anterior interosseous nerve) causes loss of thumb, index, and middle finger flexion ("hand of benediction")
- Anterior interosseous nerve palsy: Loss of pronation of forearm, flexion of thumb IP joint and index DIP joint - classic "pinch sign"
Exam point: Supracondylar fracture is the most common cause of Volkmann's ischaemic contracture in children, due to brachial artery injury.
5. Cubital Tunnel Syndrome (Ulnar Nerve Entrapment)
Although the ulnar nerve does not pass through the cubital fossa, it passes through the cubital tunnel just posterior to the medial epicondyle. Entrapment here causes:
- Pain and paraesthesia in the ring and little fingers (ulnar nerve territory)
- Weakness of intrinsic hand muscles
- Claw hand (more pronounced in ring and little fingers)
This condition is exacerbated by prolonged elbow flexion.
6. Pronator Teres Syndrome
Compression of the median nerve as it passes between the heads of pronator teres:
- Pain in the proximal forearm
- Weakness of lateral two lumbricals, thenar muscles (except adductor pollicis), and pronator teres
- Loss of sensation in the lateral 3.5 fingers and palm
- Unlike carpal tunnel syndrome, there is no nocturnal exacerbation and Phalen's/Tinel's tests at the wrist are negative
7. Posterior Interosseous Nerve (Deep Branch of Radial) Entrapment - Radial Tunnel Syndrome
The deep branch of the radial nerve passes through the arcade of Frohse (fibrous arch at the proximal margin of supinator). Compression here causes:
- Weakness of wrist and finger extensors
- No sensory loss (pure motor nerve)
- Pain over the lateral elbow
8. Brachial Artery in Surgery
The brachial artery is used in Blalock-Taussig shunts (now rarely), and its pulse is used to guide arterial line placement. In cardiac catheterisation, the Sones technique uses brachial artery cutdown in the cubital fossa. The artery may be injured in elbow dislocations and fractures.
9. Supracondylar Process and Struthers' Ligament
In approximately 0.7% of the population, there is an anomalous bony projection (supracondylar process) on the medial distal humerus. A fibrous band - Struthers' ligament - connects this process to the medial epicondyle. This creates a fibro-osseous tunnel that can entrap both the brachial artery and median nerve, causing distal ischemia and median nerve palsy. This is an important anatomical variant in exams.
10. Drug Abuse - Forensic Point
In intravenous drug abuse, the median cubital vein and other forearm veins are repeatedly injected. This leads to:
- Abscess formation along injection routes
- Pigmented scars at the cubital fossa ("rail-road track" appearance)
- Thrombosed veins
- Risk of septicaemia, AIDS, and hepatitis
QUICK SUMMARY TABLE FOR REVISION
| Feature | Key Point |
|---|---|
| Location | Anterior to elbow joint, triangular depression |
| Base | Interepicondylar line (between medial and lateral epicondyles) |
| Medial boundary | Pronator teres (medial epicondyle origin) |
| Lateral boundary | Brachioradialis (lateral supraepicondylar ridge origin) |
| Apex | Where brachioradialis and pronator teres meet |
| Floor | Brachialis (medial 2/3) + supinator (lateral 1/3) |
| Roof | Skin, superficial fascia, deep fascia + bicipital aponeurosis |
| Contents (lat to med) | Biceps tendon → Brachial artery → Median nerve (TAN) |
| Radial nerve position | Outside fossa, deep to brachioradialis |
| Ulnar nerve position | DOES NOT pass through; goes posterior to medial epicondyle |
| Key vein in roof | Median cubital vein (connects cephalic to basilic) |
| Protection of artery | Bicipital aponeurosis separates artery from superficial vein |
| Brachial artery bifurcation | At apex of fossa → radial + ulnar arteries |
| Clinical: BP measurement | Brachial artery, medial to biceps tendon |
| Clinical: venepuncture | Median cubital vein, safe due to bicipital aponeurosis |
| Clinical: fracture risk | Supracondylar fracture → brachial artery + median nerve |
HIGH-YIELD EXAM QUESTIONS
Q1. What are the boundaries of the cubital fossa?
Base = interepicondylar line; Medial = pronator teres; Lateral = brachioradialis; Floor = brachialis + supinator; Roof = skin + deep fascia + bicipital aponeurosis.
Q2. List the contents of the cubital fossa from lateral to medial.
Tendon of biceps brachii → Brachial artery → Median nerve (mnemonic: TAN).
Q3. Which nerve does NOT pass through the cubital fossa?
The ulnar nerve (passes posterior to the medial epicondyle).
Q4. What is the clinical significance of the bicipital aponeurosis?
It forms part of the roof of the cubital fossa and protects the brachial artery and median nerve during venepuncture at the median cubital vein.
Q5. Where does the brachial artery bifurcate?
At the apex of the cubital fossa into radial (lateral) and ulnar (medial) arteries.
Q6. Where does the radial nerve divide into its branches?
At the level of the lateral epicondyle, outside the cubital fossa (deep to brachioradialis) into superficial (sensory) and deep (posterior interosseous nerve/motor) branches.
Q7. Which vein is preferred for IV access at the elbow and why?
The median cubital vein - it is large, superficial, relatively fixed, and separated from the brachial artery by the bicipital aponeurosis.
Q8. What is Volkmann's ischaemic contracture?
Ischaemic contracture of forearm flexor muscles secondary to brachial artery injury, classically following supracondylar fracture of the humerus. The cubital fossa structures are directly implicated.
Q9. What is the floor of the cubital fossa?
Medial two-thirds - brachialis muscle; lateral one-third - supinator muscle.
Q10. Name the cutaneous nerves over the cubital fossa.
Medially - medial cutaneous nerve of forearm; laterally - lateral cutaneous nerve of forearm (terminal branch of musculocutaneous nerve).
MNEMONICS SUMMARY
| Mnemonic | What it helps remember |
|---|---|
| TAN (Tendon-Artery-Nerve) | Contents of cubital fossa, lateral to medial |
| "Really Need to Be Paid" | Radial N, Biceps tendon, Brachial a., Pronator teres (lateral to medial) |
| "Bicep's Medial = Brachial Artery" | Brachial artery lies just medial to the biceps tendon |
| "Ulnar = Under (posterior)" | Ulnar nerve passes behind (posterior to) the medial epicondyle |
SOURCES
- Gray's Anatomy for Students, 4th Ed. - Chapter 7 (Upper Limb), pp. 889-891
- Thieme Atlas of Anatomy: General Anatomy and Musculoskeletal System - Section 5.10 (The Elbow/Cubital Region), pp. 412-414
- Imaging Anatomy: Text and Atlas, Volume 3 - Upper Limb
This is a shared conversation. Sign in to Orris to start your own chat.