AMPUTATION of lower limb orthopedic exam documentation
Reading File
Finding Sources
Finding Sources
Searching the Web
lower limb amputation orthopedic clinical examination documentation stump assessment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have sufficient content from multiple authoritative textbooks to write a comprehensive lower limb amputation orthopedic exam documentation guide. Let me compose the full response.
Lower Limb Amputation - Orthopedic Examination & Documentation
A structured examination of a lower limb amputee follows the standard orthopedic approach: History → Look → Feel → Move → Special Tests → Neurovascular → Functional Assessment. Thorough documentation is essential for rehabilitation planning, prosthetic fitting, and complication management.
1. HISTORY
Patient Demographics
- Age, sex, dominant side
- Date and level of amputation
- Surgeon and institution
Reason for Amputation (document clearly)
The classic surgical framework: the limb was dead, deadly, or a dead loss - Bailey & Love's Short Practice of Surgery, 28th Ed.
| Category | Examples |
|---|---|
| Dead limb | Dry gangrene (atherosclerosis, embolism, DM small vessel disease) |
| Deadly limb | Wet gangrene, spreading cellulitis, gas gangrene, malignancy (e.g. osteosarcoma), AV fistula |
| Dead loss limb | Severe rest pain (unreconstructable CLI), contracture, paralysis, major trauma |
Relevant Medical History
- Diabetes mellitus, peripheral arterial disease, renal failure
- Cardiac status, hypertension, smoking history
- Trauma mechanism (if traumatic amputation)
- Prior vascular interventions (bypass, angioplasty)
- Functional status pre-amputation
Symptoms to Document
- Residual limb pain (stump pain)
- Phantom limb sensation - patient feels the amputated part is still present
- Phantom limb pain - painful sensation in the amputated part
- Back pain (biomechanical consequence of altered gait)
- Contralateral limb symptoms (critical - see below)
2. LEVEL OF AMPUTATION - DOCUMENT PRECISELY
Levels from distal to proximal:
| Level | Technical Name | Notes |
|---|---|---|
| Single toe | Digital amputation | Minor; DM/vascular |
| Ray excision | Digit + metatarsal head | For MTP joint involvement |
| Transmetatarsal | TMA | Preserves plantar weight-bearing; requires good vascularity to mid-foot |
| Syme | Ankle disarticulation with heel flap | End-bearing stump; for ankle/foot pathology |
| Transtibial | Below-knee (BKA) | Most common major amputation; preserves knee |
| Through-knee | Knee disarticulation | Rarely definitive; used emergently for ascending infection |
| Transfemoral | Above-knee (AKA) | Reserved for failed BKA candidate, proximal tissue loss |
| Hip disarticulation | - | Proximal thigh ischemia/trauma; high morbidity |
Key functional documentation: BKA requires ~50% less energy expenditure for ambulation than AKA. This directly impacts rehabilitation prognosis. - Current Surgical Therapy, 14th Ed.
3. LOOK (Inspection)
Residual Limb (Stump)
Shape and length
- Cylindrical (ideal for prosthetic fitting) vs. bulbous (poor fit) vs. conical
- Stump length in centimeters (from fixed bony landmark - e.g. tibial tuberosity for transtibial, greater trochanter for transfemoral)
Skin and soft tissue
- Healed vs. open wound
- Scar: position (end, posterior, medial, lateral), adherence to underlying bone/fascia
- Skin condition: redundant dog-ears, skin folds, adherent scarring
- Discoloration, erythema, breakdown, pressure ulcers
- Oedema/swelling (use figure-of-8 measurement or volumetry)
- Sinuses (suggest osteitis or sequestrum)
Wound healing (if post-op)
- Wound dehiscence: partial vs. complete
- Flap viability: evidence of ischaemia, necrosis
- Signs of infection: purulence, warmth, cellulitis
Posture and alignment
- Hip/knee contracture: critically important - document early
- Transtibial: look for knee flexion contracture
- Transfemoral: look for hip flexion/abduction contracture
- Standing posture and trunk balance (if bilateral amputee)
Contralateral Limb
This must not be forgotten. - Bailey and Love's, 28th Ed.
- Skin: ulcers, callus, nail care
- Vascular: colour, hair loss, atrophy
- Oedema
4. FEEL (Palpation)
Stump end
- Tenderness over bony prominences - suggests bone spur, inadequate soft tissue padding
- Point tenderness along scar - suggests neuroma
- Palpable bony spur or prominent bone end
- Skin mobility over bone (adherent = poor prosthetic tolerance)
Temperature
- Warmth (infection, inflammation)
- Coolness (vascular compromise)
Neuroma assessment
- Tinel's sign: percuss along the course of divided nerves; a shooting electric pain into the stump/phantom territory = positive; suggests neuroma formation
Oedema
- Pitting vs. non-pitting
- Measure circumference at fixed distances from bony landmark (e.g. 5 cm, 10 cm, 15 cm distal to tibial tuberosity)
Tissue quality
- Adequate muscle bulk for padding
- Subcutaneous tissue firmness
- Bony prominences (fibular head, tibial crest, condyles)
5. MOVE (Range of Motion)
Document all adjacent joint movements using a goniometer. Contracture is the most common preventable complication, delaying prosthetic fitting.
Transtibial Amputee
| Joint | Movements to Assess | Document |
|---|---|---|
| Knee | Flexion, Extension | Active & passive ROM, fixed flexion deformity (FFD) in degrees |
| Hip | Flexion, Extension, Abduction, Adduction, IR, ER | FFD, abduction contracture |
Transfemoral Amputee
| Joint | Movements to Assess | Document |
|---|---|---|
| Hip | Flexion/Extension (Thomas test for FFD), Abduction/Adduction, IR/ER | FFD degree, abduction contracture |
| Lumbar spine | Extension (if hip flexion restricted, lumbar hyperlordosis compensates) |
Contralateral Lower Limb
- Full ROM documentation of ankle, knee, hip
- Any contracture on the sound side will impair ambulation with prosthesis
6. MUSCLE STRENGTH TESTING
Grade using MRC 0-5 scale:
- Transtibial: Hip flexors, extensors, abductors; knee flexors and extensors
- Transfemoral: Hip flexors, extensors, abductors, adductors; contralateral full assessment
- Bilateral amputee: Upper limb strength (critical for transfers and crutch walking)
- Core strength (stability for prosthetic gait)
7. NEUROVASCULAR ASSESSMENT
Residual Limb
- Sensation: light touch, pinprick along stump and around scar
- Identify areas of altered sensation (potential neuroma territory)
- Document phantom sensations if present
Contralateral Limb (mandatory)
- Peripheral pulses: femoral, popliteal, dorsalis pedis, posterior tibial
- ABPI (Ankle-Brachial Pressure Index) if vascular cause
- Capillary refill time
- Sensation: peripheral neuropathy testing (10g monofilament in diabetics)
- Vibration sense (128 Hz tuning fork)
8. COMPLICATIONS - ASSESS AND DOCUMENT
Early (Post-Operative)
| Complication | Clinical Signs to Document |
|---|---|
| Haemorrhage | Soaked dressings, drain output, haematoma |
| Infection/haematoma | Erythema, fluctuance, pyrexia, purulent discharge |
| Wound dehiscence | Extent (cm), depth, tissue viability |
| Gas gangrene | Crepitus, bullae, severe pain out of proportion - emergency |
| DVT/PE | Calf tenderness, Homan's sign, dyspnoea |
| Flap necrosis | Colour change, demarcation line |
Late (Chronic Amputee)
| Complication | Clinical Signs to Document |
|---|---|
| Bone spur | Tender bony prominence at stump end on palpation |
| Neuroma | Positive Tinel's, point tenderness along nerve course |
| Adherent scar | Skin fixed to underlying bone, painful with prosthetic |
| Sinus/osteitis | Chronic discharge, probe-to-bone, XR changes |
| Stump ulcer | From prosthetic pressure, ischaemia; measure size, depth, Wagner grade |
| Contracture | Fixed flexion/abduction at hip or knee - prevents prosthetic use |
| Phantom pain | Ongoing burning, shooting, cramping in absent limb territory |
Phantom pain management: firm reassurance that sensation usually resolves; gabapentin or amitriptyline may help. - Bailey and Love's, 28th Ed.
9. PROSTHETIC ASSESSMENT
Document for patients who are prosthetic users:
- Current prosthesis: type, age, condition
- Socket fit: comfortable, loose, tight, skin breakdown areas
- Suspension mechanism: suction, pin lock, sleeve, belt
- Liner condition: integrity, hygiene
- Prosthetic components: foot type (SACH, dynamic response, hydraulic), knee joint type (transfemoral)
- Walking aids used: none, crutch, stick, frame
10. FUNCTIONAL & REHABILITATION ASSESSMENT
Mobility Level (K-Level / Medicare Functional Classification)
| K Level | Description | Document |
|---|---|---|
| K0 | No potential for ambulation | Non-ambulatory; transfers only |
| K1 | Household ambulation (limited, flat surfaces) | Walking aid type, distance |
| K2 | Limited community ambulation | Uneven terrain, stairs (with rail) |
| K3 | Community ambulation | Variable cadence, most surfaces |
| K4 | Child/athlete/high demand | High activity, prosthetic stress |
Activities of Daily Living
- Transfers: independent / supervised / assisted
- Stair ascent/descent
- Donning/doffing prosthesis
- Distance walked (metres or blocks)
- Walking speed (Timed Up and Go test)
- Falls history and fall risk
11. PSYCHOLOGICAL & SOCIAL ASSESSMENT
- Body image and acceptance of amputation
- Depression/anxiety screening (PHQ-9 or similar)
- Social support at home
- Home environment (stairs, accessibility)
- Occupation and vocational goals
- Patient's prosthetic expectations and motivation
12. INVESTIGATIONS TO DOCUMENT
| Investigation | Indication |
|---|---|
| Plain X-ray of residual limb | Bone spur, osteitis, sequestrum, fracture |
| Stump doppler / ABPI | Vascular status, healing potential of revision |
| TcPO2 (transcutaneous oxygen) | Healing potential at a given amputation level |
| MRI/CT | Suspected infection, tumour recurrence, soft tissue mass |
| Blood: FBC, CRP, ESR | Infection workup |
| HbA1c, glucose | Diabetic amputee wound healing |
| Albumin, pre-albumin | Nutritional status for wound healing |
13. DOCUMENTATION TEMPLATE (SOAP FORMAT)
SUBJECTIVE:
- Age/sex, side, level of amputation, date
- Reason for amputation (vascular/traumatic/oncological/septic)
- Chief complaint: stump pain / phantom pain / poor prosthetic fit / wound breakdown
- Functional status: K-level, walking aids, distance
OBJECTIVE:
LOOK:
- Stump shape: cylindrical / bulbous / conical
- Length: ___ cm from [landmark]
- Skin: healed / wound (___ x ___ cm) / sinus / ulcer / adherent scar
- Oedema: present / absent; circumference at ___ cm = ___ cm
- Contracture: knee FFD ___°, hip FFD ___°
- Contralateral limb: [findings]
FEEL:
- Tenderness: stump end / over scar / neuroma (Tinel positive/negative)
- Temperature: warm / cool
- Skin mobility: free / adherent
- Oedema: pitting / non-pitting
MOVE:
- Knee: Flexion ___° / Extension ___° (FFD ___°)
- Hip: Flexion ___° / Extension ___° / Abduction ___° (FFD ___°)
- Muscle strength: [MRC grades]
NEUROVASCULAR:
- Sensation: intact / impaired [distribution]
- Pulses: [bilateral documentation]
- ABPI: ___
SPECIAL TESTS:
- Tinel's: positive / negative at [location]
- Thomas test: FFD ___°
PROSTHETIC:
- Type: [BK/AK], socket fit: good / loose / tight
- Skin under socket: intact / pressure areas at ___
ASSESSMENT:
- Level: [Transtibial / Transfemoral / etc.]
- Complications present: [list]
- Rehabilitation potential: [K-level]
PLAN:
- Wound management / compression therapy / physiotherapy
- Prosthetic review / socket revision
- Pain management (gabapentin/amitriptyline for phantom pain)
- Contralateral limb protection
- MDT referral: prosthetist / physio / OT / vascular / psychologist
Key Documentation Pearls
- Always document the contralateral limb - a pressure ulcer on the remaining foot will delay mobilisation despite satisfactory stump healing.
- Contracture prevention starts at surgery - document flexion deformities early because they prevent prosthetic fitting.
- Amputation is not failure - document it as a reconstructive procedure; studies show improved quality of life and satisfaction after appropriate amputation.
- Energy expenditure matters - AKA requires ~50% more energy than BKA for ambulation; this directly affects whether a patient will achieve community walking.
- Phantom pain - document its character, severity (VAS/NRS), and current management. It is real and requires treatment.
- Nutritional and vascular status - document these for every wound/healing assessment.
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed. | Campbell's Operative Orthopaedics, 15th Ed. 2026 | Current Surgical Therapy, 14th Ed. | Miller's Review of Orthopaedics, 9th Ed.
Lisfranc and chopart
Finding Sources
Finding Sources
Searching the Web
Lisfranc Chopart amputation orthopedic examination documentation levels
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed - including the key anatomical diagram. Let me now deliver the comprehensive response.
Lisfranc & Chopart - Orthopedic Exam Documentation
These are the two mid-level foot amputation levels, and also important injury complexes of the foot. Both are covered below in full.
PART 1: ANATOMY - THE LEVELS
The diagram below from Sabiston's Textbook of Surgery shows exactly where these levels fall:
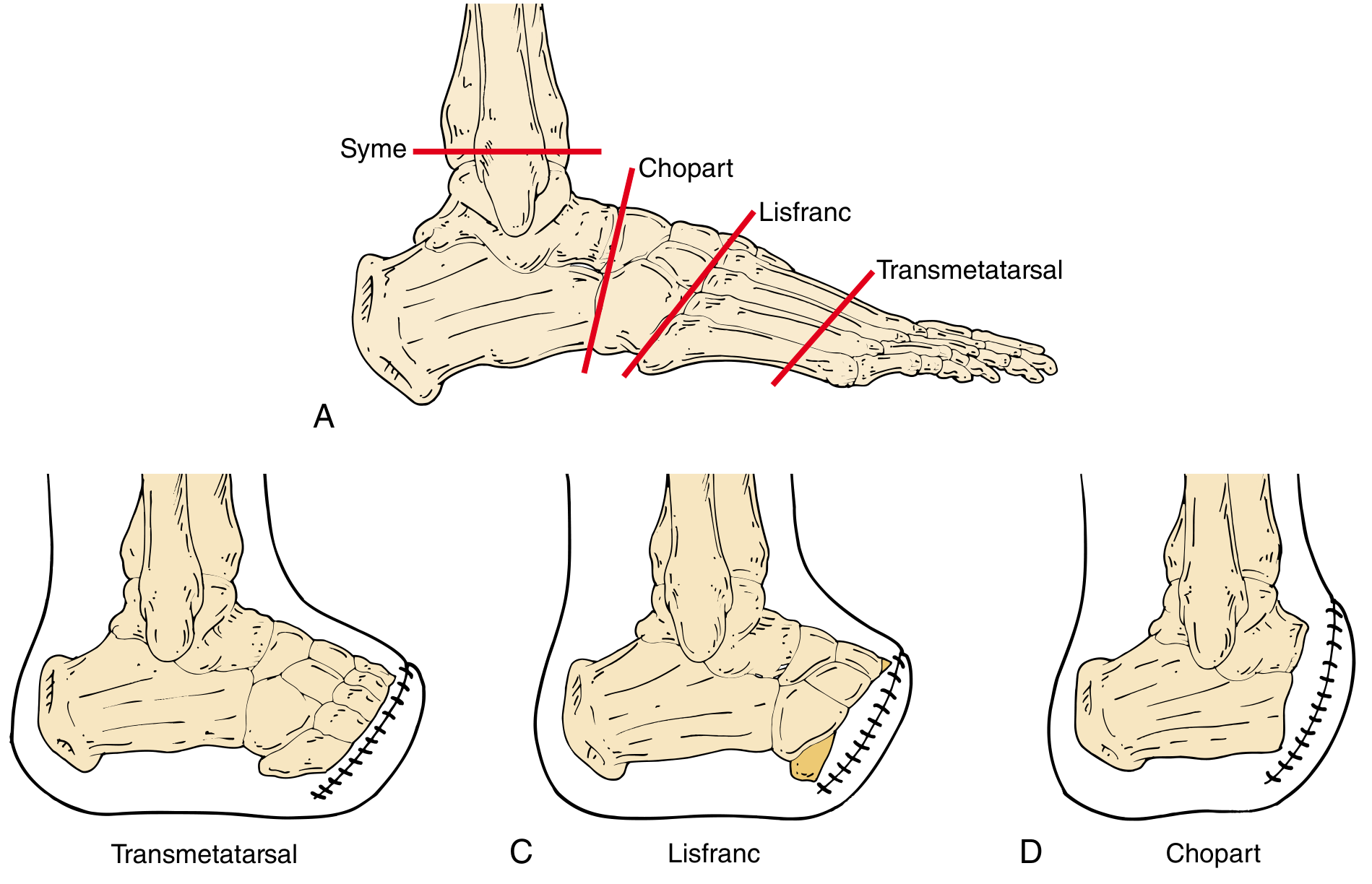
| Level | Joint | Bones Preserved | Bones Removed |
|---|---|---|---|
| Transmetatarsal | Through metatarsal shafts | Hindfoot + midfoot + metatarsal bases | Metatarsal heads + all toes |
| Lisfranc | Tarsometatarsal (TMT) joints | Hindfoot + all tarsals (cuneiforms, cuboid, navicular) | All 5 metatarsals + toes |
| Chopart | Transverse tarsal (midtarsal) joint = talocalcaneonavicular + calcaneocuboid | Talus + calcaneus only | Navicular, cuboid, cuneiforms, metatarsals, toes |
| Syme | Ankle (tibiotalar) | Tibia + fibula | Entire foot |
PART 2: LISFRANC
A. Lisfranc INJURY (Fracture-Dislocation)
Anatomy
- The tarsometatarsal (TMT) joint complex sits at the apex of the longitudinal arch - a high-stress zone
- The Lisfranc ligament runs from the medial cuneiform to the base of the 2nd metatarsal - the key stabiliser
- The 2nd metatarsal is recessed as the "keystone" between medial and lateral cuneiforms - providing transverse stability
- There is no intermetatarsal ligament between the 1st and 2nd metatarsal bases (hence the vulnerability)
- Three columns:
- Medial: 1st MT + medial cuneiform + navicular facet
- Middle: 2nd & 3rd MT + corresponding cuneiforms
- Lateral: 4th & 5th MT + cuboid
Mechanism
- Forced plantarflexion of the midfoot (e.g. fall from height, horsefall - historically Jacques Lisfranc noted this in cavalry)
- Crush injury (heavy weight forcing foot flat)
- Low-energy: twisting in sport (often purely ligamentous "subtle" injury)
Classification (Myerson modification of Quénu-Küss / Hardcastle)
| Type | Pattern | Description |
|---|---|---|
| A | Homolateral | All 5 metatarsals displaced as a unit (usually lateral/dorsolateral) |
| B1 | Partial medial | Medial displacement; may involve intercuneiform or naviculocuneiform joint |
| B2 | Partial lateral | Lateral displacement; may involve 1st MT-cuneiform joint |
| C1 | Divergent partial | Some metatarsals go medial, others lateral |
| C2 | Divergent complete | High-energy; all metatarsals involved; high risk of compartment syndrome |
Clinical Examination
LOOK
- Swelling over the dorsal midfoot (can be massive in high-energy)
- Plantar ecchymosis - a highly specific sign of significant ligamentous disruption; examine the sole carefully
- Inability to bear weight
- Gross deformity / step deformity visible in complete dislocations
FEEL
- Tenderness directly over the TMT joints - palpate each joint individually:
- 1st MT-medial cuneiform joint
- 2nd MT-middle cuneiform joint (most commonly involved)
- Lateral column (4th/5th MT-cuboid)
- Tenderness at the Lisfranc ligament (between medial cuneiform and 2nd MT base)
MOVE / SPECIAL TESTS
- Piano key test (axial load test): dorsally applied axial force along the shaft of each metatarsal - pain at the TMT joint = positive
- Passive pronation-abduction stress: reproduction of pain at midfoot
- Inability to perform single-leg heel rise (painful / weak)
- Check for compartment syndrome in high-energy injuries (tight compartments, pain on passive stretch of toes, sensory deficit)
Radiology Documentation
- Weight-bearing AP, oblique, and lateral X-rays of both feet (compare sides) - must be weight-bearing to detect subtle instability
- Key radiographic alignments to document:
- AP view: Medial shaft of 2nd MT aligns with medial border of middle cuneiform
- Oblique view: Medial border of 4th MT aligns with medial border of cuboid
- AP view: Medial border of 2nd MT aligns with medial border of 2nd cuneiform
- "Fleck sign": avulsion fracture at base of 2nd MT or medial cuneiform = pathognomonic of Lisfranc ligament avulsion
- CT foot if X-ray equivocal - superior for detecting subtle injuries and fracture comminution
- A standing radiograph of both feet on the same cassette allows comparison and highlights subtle diastasis
Treatment Options (document which was performed)
- Conservative (non-displaced, stable): Non-weight-bearing cast x 6 weeks
- ORIF (displaced): Screws or dorsal bridge plating across TMT joints
- Primary arthrodesis: For purely ligamentous injuries (recent RCT evidence favours this for medial column)
- Post-fixation: Hardware removal typically at 3-6 months if symptomatic
B. Lisfranc AMPUTATION
Definition
Disarticulation through the tarsometatarsal joints - all 5 metatarsals and the toes are removed, preserving the full complement of tarsal bones (cuneiforms, cuboid, navicular, talus, calcaneus).
Surgical Key Points (document intraoperatively)
- Uses a long plantar flap (preferred over fish-mouth dorsal-plantar flaps)
- 1st, 3rd, 4th, 5th TMT joints are disarticulated
- 2nd metatarsal is transected 2 cm distal to the medial cuneiform (not disarticulated, to preserve stability)
- Base of 5th metatarsal is preserved with peroneus brevis and tertius insertion to prevent inversion deformity during gait
- Achilles tendon lengthening (percutaneous) is performed to prevent equinus/equinovarus deformity
- Plantar fascia approximated to dorsal fascia/periosteum
- Plaster cast applied with talus in slight dorsiflexion
Critical Complication to Document and Examine For
| Complication | Examination Finding | Notes |
|---|---|---|
| Equinus contracture | Ankle fixed in plantarflexion; Thomas test equivalent at ankle; reduced dorsiflexion | Most important late complication; prevented by Achilles lengthening at surgery |
| Equinovarus deformity | Foot inverted and plantarflexed | Failure to preserve 5th MT base / peroneus brevis |
| Wound breakdown | Flap necrosis, ulceration | Failed wound healing in ~20% of Lisfranc amputees |
| Re-amputation | Higher-level surgery needed | Often to Syme or transtibial level |
| Plantar pressure ulcer | Over residual bone ends | If TMA done through distal metaphysis |
Functional Outcome
- 85% of patients can ambulate without prosthesis for short distances (direct end-loading possible) - [systematic review, PMC9997832]
- Requires custom footwear with toe filler and rocker sole for longer distances
- Better functional outcome than transtibial amputation for low-demand patients
PART 3: CHOPART
A. Chopart INJURY
Anatomy
The transverse tarsal joint (midtarsal joint) = two joints acting together:
- Talonavicular joint (medial)
- Calcaneocuboid joint (lateral)
These two joints work in concert with subtalar motion. Together they form the "Chopart joint" (named after François Chopart).
Clinical Examination of Chopart Injury
LOOK
- Swelling over the dorsal midfoot/hindfoot junction
- Bruising at mid-arch (dorsal and plantar)
- Deformity in severe dislocations (foot deviated relative to hindfoot)
FEEL
- Tenderness over:
- Talonavicular joint (just distal to the talar head, medial side)
- Calcaneocuboid joint (lateral, distal to the anterior calcaneus)
- Palpate navicular tuberosity (common fracture site)
- Palpate anterior process of calcaneus (frequently fractured in Chopart injuries)
MOVE
- Subtalar motion: restricted and painful (talocalcaneal joint stress)
- Midfoot abduction/adduction: reproduce pain at Chopart joint
- Weight-bearing: often impossible
Radiology
- Weight-bearing X-rays: AP, oblique, lateral
- CT is mandatory for full characterisation of Chopart injuries (often underestimated on plain films)
- Document: talonavicular dislocation, calcaneocuboid subluxation, associated navicular/cuboid fractures
B. Chopart AMPUTATION
Definition
Disarticulation through the talocalcaneonavicular joint AND calcaneocuboid joint simultaneously - only the talus and calcaneus are preserved.
Two Types
| Type | Description |
|---|---|
| Conventional Chopart | Disarticulation only; relies on soft tissue balance |
| Modified Chopart | Includes tendon transfer of tibialis anterior (and long extensors) to the neck of the talus to counterbalance the Achilles tendon pull |
The modified technique is now standard because it prevents the dominant complication of equinus contracture.
Surgical Key Points (document)
- Long plantar flap ("fish-mouth" with longer plantar limb)
- Achilles tendon tenectomy performed first (2 cm excised, sheath preserved) to prevent equinus
- Transverse tarsal joints are disarticulated by releasing dorsal and plantar ligaments
- Tibialis anterior + long extensor tendons transferred to the neck of the talus via bone tunnel or suture anchor
- Wound closed with fascial approximation plantarly and dorsally
- Well-padded dorsiflexion rigid dressing applied
Post-Operative Care
- Dorsiflexion rigid dressing changed intermittently for wound checks
- Sutures kept 4-6 weeks (longer than standard - poor vascularity)
- Splint in 5 degrees of dorsiflexion for 6-8 weeks to prevent equinus
Prosthetic / Orthotic Requirement
- Ankle-foot orthosis (AFO) in a rocker-sole shoe (e.g. running shoe) for ambulation
- Cannot use a simple toe filler like Lisfranc - needs custom AFO because the forefoot lever arm is absent
Complications - Examine For
| Complication | Exam Finding | Frequency |
|---|---|---|
| Equinus contracture | Fixed plantarflexion of hindfoot; the dominant late complication if Achilles not released | Very common with conventional technique |
| Wound breakdown | Flap necrosis; failed primary healing | ~46% conventional, ~28% modified |
| Re-amputation (usually to transtibial level) | Documented at follow-up | High rate with conventional technique |
| Stump ulceration | From prosthetic/AFO pressure over the talus or calcaneus | |
| Varus deformity | Foot inverted at rest | Corrected by tibialis anterior transfer to talus neck |
Functional Outcome
- 74% ambulatory without prosthesis after modified Chopart (for short distances)
- Direct loading of the calcaneus is possible - an advantage over transtibial
- However, both Lisfranc and Chopart are controversial in vascular/diabetic patients due to high wound complication rates - Miller's Review of Orthopaedics 9th Ed.: "most experts recommend avoiding amputation at these levels if possible in patients with diabetes or vascular disease"
PART 4: COMPARATIVE EXAM DOCUMENTATION TABLE
| Feature | Lisfranc Amputation | Chopart Amputation |
|---|---|---|
| Level | Tarsometatarsal joints | Transverse tarsal joints |
| Retained bones | All tarsals (7 bones) | Talus + calcaneus only |
| Stump length | Mid-foot | Hindfoot only |
| Key complication | Equinovarus deformity | Equinus contracture |
| Prevention | Preserve 5th MT base + Achilles lengthening | Achilles tenectomy + tibialis anterior transfer |
| Prosthetic need | Custom shoe + toe filler | AFO + rocker sole shoe |
| Ambulation without prosthesis | ~85% (short distances) | ~74% modified technique |
| Wound healing failure | ~20% | ~28-46% |
| Examine for at follow-up | Equinovarus, flap breakdown, ulcer | Equinus, flap breakdown, AFO socket sores |
PART 5: EXAMINATION DOCUMENTATION TEMPLATE
LISFRANC / CHOPART EXAMINATION
HISTORY:
- Level: [ ] Lisfranc disarticulation [ ] Chopart (conventional / modified)
- Date of surgery:
- Indication: DM / vascular / trauma / tumour / infection
- Achilles released at surgery: yes / no
- Tendon transfer performed: yes / no
LOOK:
- Stump shape: adequate plantar flap / bulbous / necrotic flap
- Wound: healed / breakdown (___cm x ___cm) / sinus
- Skin: intact / callus / ulcer (location: ___; Wagner grade: ___)
- Alignment: plantigrade / equinus (degree: ___°) / varus / valgus
- Erythema / signs of infection: yes / no
FEEL:
- Tenderness: stump end / dorsum / plantar surface
- Neuroma: Tinel at ___
- Temperature: warm / cool (vascular concern)
- Oedema: present / absent
MOVE:
- Ankle dorsiflexion: ___° (Lisfranc stump)
- Hindfoot: neutral / equinus ___° / varus ___° (Chopart stump)
- Hip and knee ROM (full; document any contracture)
PROSTHETIC / ORTHOTIC:
- Lisfranc: custom shoe with toe filler - fit: good / poor
- Chopart: AFO with rocker sole - fit: good / poor; socket sores: yes / no
FUNCTIONAL:
- Weight-bearing: full / partial / non-weight-bearing
- Walking without prosthesis/orthosis: yes / no; distance: ___
- Walking with device: distance / terrain ability
- K-level: ___
INVESTIGATIONS:
- X-ray (standing): equinus / varus deformity; bony prominences
- Vascular: ABPI ___, TcPO2 ___ (if wound healing concern)
- Blood: CRP/WCC/ESR (if infection)
PLAN:
- [ ] Wound management
- [ ] Equinus correction (stretching / serial casting / surgical Achilles release)
- [ ] Varus correction (tibialis anterior tendon transfer to talus neck)
- [ ] Prosthetic / orthotic revision
- [ ] Re-amputation if healing failure (document level: Syme / BKA)
- [ ] Vascular review
Sources: Sabiston Textbook of Surgery, latest Ed. | Campbell's Operative Orthopaedics, 15th Ed. 2026 | Miller's Review of Orthopaedics, 9th Ed. | Bailey and Love's Short Practice of Surgery, 28th Ed. | Lisfranc and Chopart amputation: A systematic review, PMC9997832
This is a shared conversation. Sign in to Orris to start your own chat.