Applied anatomy of teeth and gums
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed answer.
Applied Anatomy of Teeth and Gums
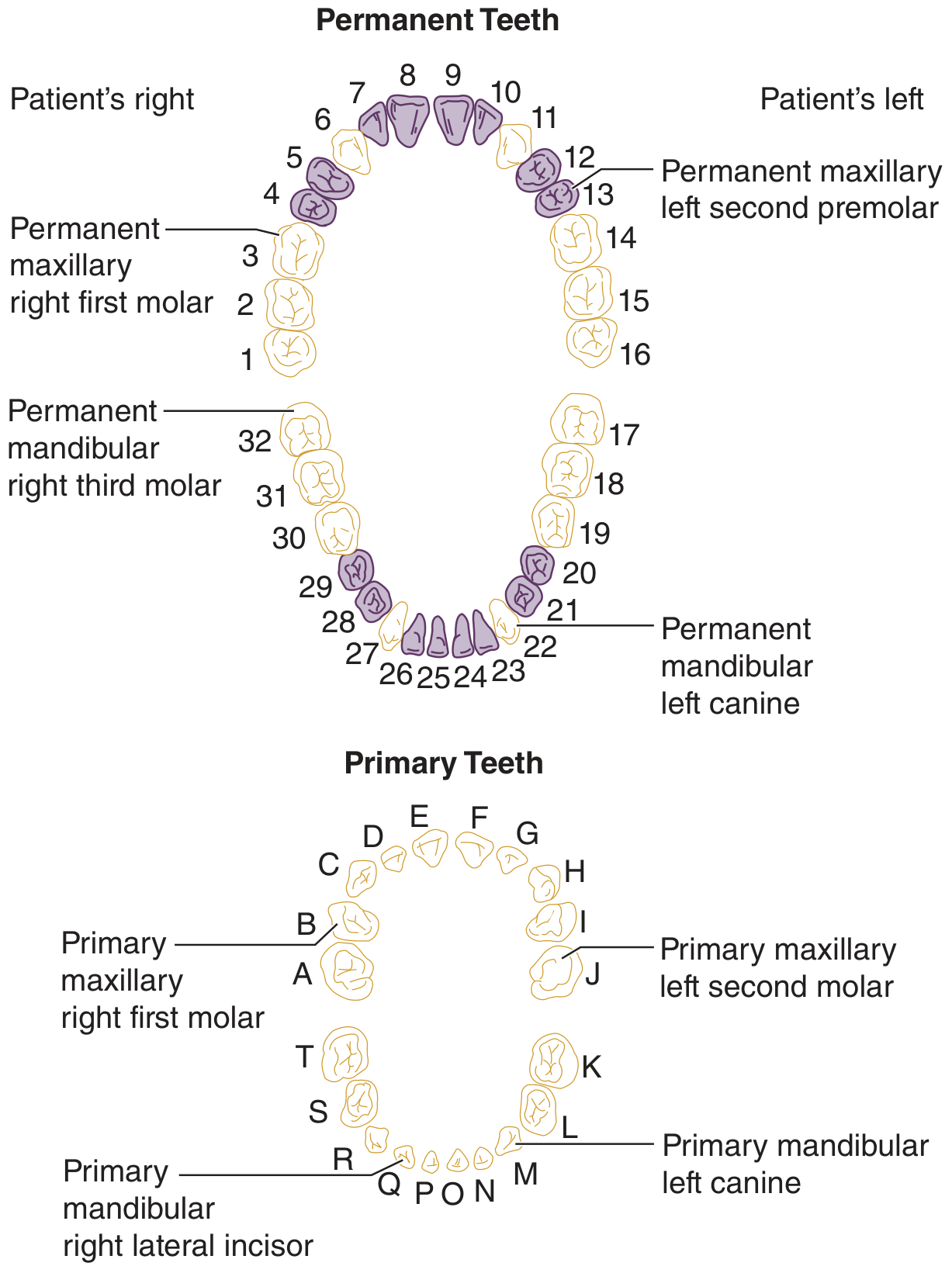
1. Dentition - Overview
The human lifespan involves two sets of teeth:
- Primary (deciduous) dentition: 20 teeth - 8 incisors, 4 canines, 8 molars. Fully erupted by age 3, shed by age 13.
- Permanent dentition: 32 teeth - 8 incisors, 4 canines, 8 premolars, 12 molars. Begin erupting at age 6 and are complete by ~age 14, except third molars ("wisdom teeth") which may erupt later.
2. Gross Anatomy of a Single Tooth
Each tooth is divided into two major anatomical regions:
Crown
The visible portion above the gumline. It is covered by enamel - the hardest substance in the human body, composed largely of hydroxyapatite, produced by ameloblasts before tooth eruption. Once formed, enamel cannot regenerate because ameloblasts are lost at eruption.
Root
The portion submerged in the alveolar bone, not visible in the healthy mouth. It is covered by a thin layer of cementum rather than enamel.
Neck (Cervix)
The constriction at the junction of crown and root, where the gingiva attaches.
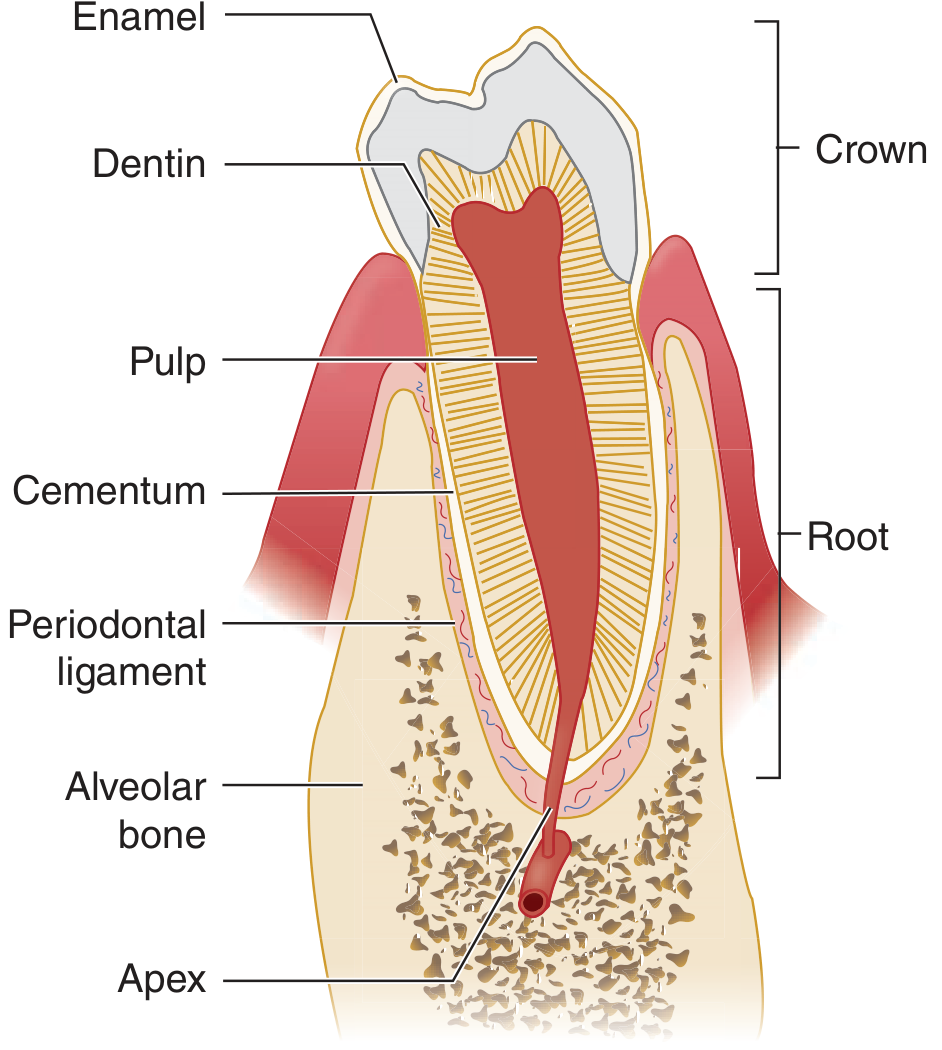
3. Tissue Layers of the Tooth
Enamel
- Outermost layer of the crown
- ~96% inorganic (hydroxyapatite crystals arranged as enamel rods)
- Hardest biological tissue; no cells remain after formation
- Produced by ameloblasts (from ectoderm) prior to eruption
- Vulnerable to acid demineralization by bacterial metabolites (e.g., Streptococcus mutans)
Dentin
- Constitutes the bulk of the tooth, underlying both enamel (in the crown) and cementum (in the root)
- Denser than bone, exquisitely sensitive to pain
- Produced by odontoblasts (from neural crest-derived mesenchyme) throughout life
- Deposited as a system of microtubules filled with odontoblastic processes and extracellular fluid
- Contains dentinal tubules that transmit stimuli (thermal, tactile, osmotic) to the pulp, explaining dentinal hypersensitivity
Pulp
- Occupies the central pulp chamber and root canals
- Consists of loose connective tissue (myxomatous pulp) containing:
- Blood vessels (arterial supply via apical foramen)
- Lymphatics
- Sensory nerve fibers (branches of V2/V3)
- Odontoblasts lining the periphery
- The apical foramen at the root tip is the entry point for neurovascular supply
- Clinical relevance: pulpitis (reversible or irreversible) and pulp necrosis follow bacterial invasion through caries
Cementum
-
Thin layer of mineralized connective tissue covering the root dentin
-
Resembles bone but is avascular
-
Produced by cementoblasts; mature cells (cementocytes) reside in lacunae with processes in canaliculi
-
Less metabolically active than bone but undergoes gradual remodeling
-
Provides the anchor point for Sharpey fibers of the periodontal ligament
-
Junqueira's Basic Histology, 17e - p. 751
-
Harrison's Principles of Internal Medicine, 22e - p. 1880
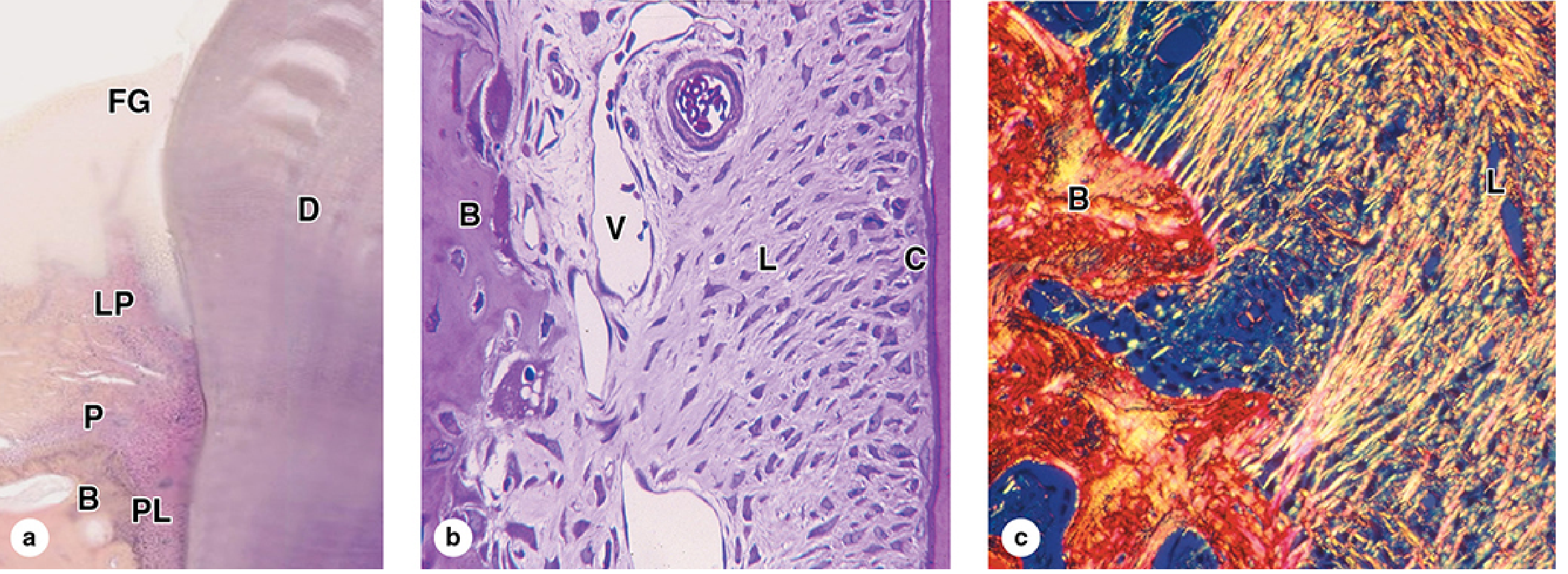
4. The Periodontium (Supporting Structures)
The periodontium (Greek: "around the tooth") is the collective term for all tissues that anchor the tooth in the jaw and protect the root from bacterial invasion.
It has two components:
A. Gingival Component (the "Gums")
- Junctional epithelium - specialized non-keratinized epithelium that forms a cuff around the tooth at the base of the gingival sulcus, sealing the periodontium from the oral cavity
- Gingival tissue - keratinized stratified squamous epithelium divided into:
- Free gingiva (marginal gingiva): the unattached margin that forms the 2-3 mm deep gingival sulcus in health. Probing depth >3 mm indicates a periodontal pocket.
- Attached gingiva: firmly adherent to underlying alveolar bone periosteum; firmly bound, stippled, immovable
- Interdental papilla: the gingiva filling the space between adjacent teeth
- Gingival fibers - collagen fiber groups within the free gingiva that maintain the sulcular seal
The mucoginigval junction demarcates the attached gingiva from the looser, non-keratinized alveolar mucosa (which extends to the vestibule). The alveolar mucosa is darker pink and more mobile.
B. Periodontal Component (Attachment Apparatus)
-
Periodontal ligament (PDL)
- Dense fibrous connective tissue occupying the space between cementum and alveolar bone (width: 150-350 µm, decreasing with age)
- Contains short bundles of collagen (Sharpey fibers) inserting into cementum on one side and alveolar bone on the other
- Unlike most ligaments: highly cellular, richly vascularized, and innervated
- Functions: tooth support (cushioning masticatory forces), proprioception (tooth position sense), nutrition of cementum, and serves as periosteum for the alveolar bone socket
- Contains PDL stem cells capable of regenerating periodontal tissues
-
Alveolar bone
- The bony socket (alveolus) housing each tooth root
- The inner wall of the socket is called the lamina dura (visible on X-ray as a dense white line)
- Lacks typical lamellar pattern; undergoes continuous remodeling by osteoblasts and osteoclasts
- Loss of alveolar bone is the defining feature of periodontitis
-
Cementum (described above under tooth layers, but functionally part of the periodontium as the attachment site for PDL fibers)
- Junqueira's Basic Histology, 17e - pp. 750-752
- Tintinalli's Emergency Medicine - pp. 1621-1622
5. Embryological Development
Tooth development begins at week 6 of embryonic life and follows a defined sequence:
| Stage | Event |
|---|---|
| Bud stage | Oral ectoderm invaginates into jaw mesenchyme at 20 future tooth sites |
| Cap stage | Enamel organ forms (wine-glass shape); dental papilla differentiates inside |
| Bell stage | Ameloblasts (inner enamel epithelium) and odontoblasts organize facing each other |
| Maturation | Odontoblasts lay down predentin -> dentin; ameloblasts lay down enamel rods outward |
| Eruption | Root formation completes, PDL anchors tooth, enamel maturation finishes |
Key cell-tissue origins:
-
Enamel: ectodermal (ameloblasts)
-
Dentin, pulp, cementum, PDL: neural crest mesenchyme (odontoblasts, cementoblasts, fibroblasts)
-
Alveolar bone: intramembranous ossification from mesenchyme
-
Junqueira's Basic Histology, 17e - p. 749
6. Nerve Supply (Clinical Relevance)
| Region | Nerve |
|---|---|
| Upper teeth (maxillary) | Anterior, middle, posterior superior alveolar nerves (branches of V2 - maxillary division of trigeminal) |
| Lower teeth (mandibular) | Inferior alveolar nerve (branch of V3 - mandibular division) |
| Buccal gingiva (lower) | Long buccal nerve (V3) |
| Lingual gingiva (lower) | Lingual nerve (V3) |
| Palatal gingiva (upper) | Greater palatine nerve (V2), nasopalatine nerve |
Applied point: Dental pain is frequently diffuse, referring as headache, sinus pain, eye pain, jaw pain, or neck pain due to convergence of trigeminal afferents. Myocardial infarction can also present with jaw pain and must be excluded.
7. Blood Supply
- Maxillary teeth: branches of the maxillary artery (posterior superior alveolar, anterior superior alveolar arteries)
- Mandibular teeth: inferior alveolar artery (from maxillary artery) entering via the mandibular foramen
- Gingiva: gingival branches of the same vessels plus lingual and facial arteries
8. Types of Teeth and Functions
| Type | Number (permanent) | Location | Function |
|---|---|---|---|
| Incisors | 8 | Central and lateral, front of each arch | Cutting/biting |
| Canines | 4 | One per quadrant, beside incisors | Tearing, guiding occlusion |
| Premolars | 8 | Between canines and molars | Crushing, grinding |
| Molars | 12 (including 4 wisdom) | Posterior-most | Heavy grinding |
9. Clinical Correlations
Dental Caries
Begins as bacterial acid (principally S. mutans) demineralizes enamel at pits, fissures, and interproximal surfaces. Progression: enamel caries -> dentin involvement -> reversible pulpitis (pain resolves when stimulus removed) -> irreversible pulpitis (spontaneous, prolonged pain) -> pulp necrosis (constant/intermittent pain, cold sensitivity lost) -> periapical abscess.
Periapical Abscess
Pulpal infection tracks through the apical foramen into periapical tissue. Radiolucency appears at root apex on X-ray. Can spread to produce:
- Periapical granuloma or cyst (chronic)
- Parulis (gum-boil) - intraoral sinus tract
- Ludwig's angina - life-threatening cellulitis of the submandibular space and floor of the mouth
Gingivitis
Reversible inflammation of the gingiva only - caused by dental plaque accumulation. Gingiva bleeds on probing; no bone loss. Fully reversible with oral hygiene.
Periodontitis
Inflammation extends to the PDL, alveolar bone, and cementum. The gingival sulcus deepens into a periodontal pocket (>3 mm probing depth). Irreversible bone loss leads to tooth mobility and eventual tooth loss. Predominantly caused by anaerobic Gram-negative bacteria (Porphyromonas gingivalis, Treponema denticola).
Pericoronitis
Inflammation of the operculum (gingival flap over an erupting tooth, most commonly the lower third molar). Debris trapped under the operculum creates a severe inflammatory response that can spread to the masticator space and cause trismus, and potentially into parapharyngeal spaces (life-threatening).
Necrotizing Periodontal Diseases
Polymicrobial (Fusobacterium + spirochetes): range from necrotizing gingivitis (ANUG/"trench mouth") to necrotizing periodontitis to necrotizing stomatitis. Extension to tonsils/pharynx = Vincent's angina.
10. The Gingival Sulcus - Key Landmark
- Normal depth: 1-3 mm
- Floor formed by the junctional epithelium
- Contains gingival crevicular fluid (GCF) - an exudate with immunoglobulins and leukocytes that has bactericidal properties
- Clinical probe inserted here to measure periodontal health
- Depth >3 mm = periodontal pocket = disease
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Ch. 245, pp. 1620-1622
- Junqueira's Basic Histology: Text and Atlas, 17e - Ch. 15, pp. 749-752
- Harrison's Principles of Internal Medicine, 22e - Diseases of the Teeth and Periodontal Structures, pp. 1880-1882
- Rosen's Emergency Medicine: Concepts and Clinical Practice - Ch. 56, pp. 859-860
Applied anatomy of teeth and gums ..... milestones related to teething
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
I now have everything needed. Here is the comprehensive answer:
Applied Anatomy of Teeth and Gums: Teething Milestones
Overview of Human Dentition
Humans have two successive sets of teeth separated by a transitional mixed dentition period:
| Feature | Primary (Deciduous) | Permanent |
|---|---|---|
| Total number | 20 | 32 |
| Types | Incisors, canines, molars | Incisors, canines, premolars, molars |
| Onset | 6-8 months postnatal | 6-7 years |
| Completion | ~2-3 years | ~14 years (wisdom teeth: 17-40) |
Period 1 - Primary (Deciduous) Dentition
How Eruption Begins
Primary teeth erupt after the crown is completely formed but while the root is still incomplete and the root canal is wide. Before a tooth breaks through, the overlying gingiva becomes swollen and discolored, and the white apex of the tooth is visible beneath the gingival epithelium before it perforates. After eruption, root growth continues substantially and the PDL differentiates. The enamel cuticle covering the erupted crown is gradually resorbed.
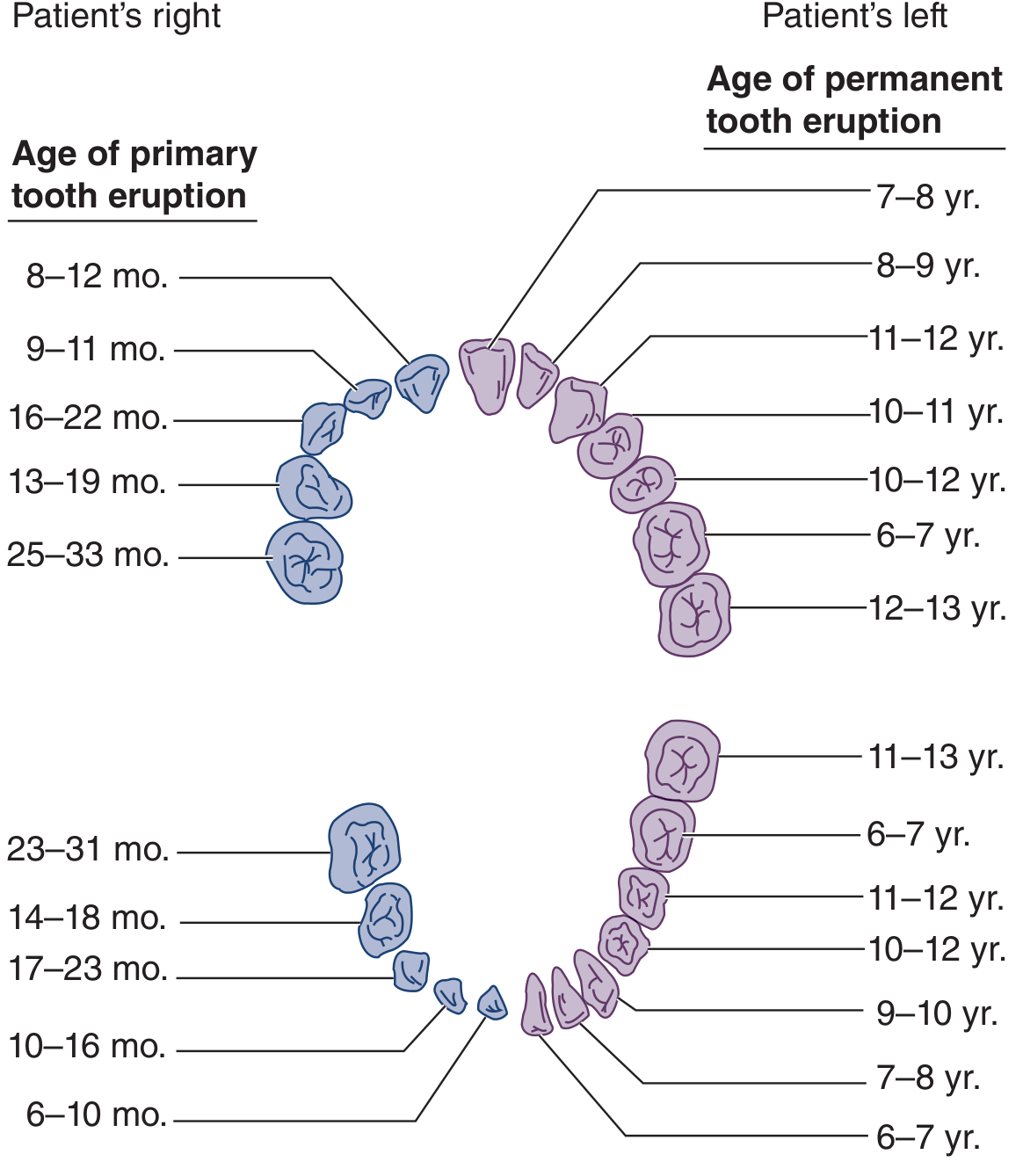
Eruption Sequence and Ages
The sequence follows a predictable pattern - incisors first, then first molars, then canines, then second molars:
| Tooth | Eruption Age |
|---|---|
| Central incisors (lower then upper) | 6-12 months |
| Lateral incisors | 9-16 months |
| First primary molars | 13-19 months |
| Canines | 16-23 months |
| Second primary molars | 23-33 months |
Full primary dentition complete: by ~2-3 years of age
A commonly used memory rule: lower teeth erupt before their upper counterparts, and bilateral pairs erupt roughly together.
Period 2 - Mixed Dentition (6-12 years)
This transitional phase begins at age 6 with eruption of the first permanent molar - a landmark event. Primary teeth are shed (exfoliated) as their roots are resorbed by the pressure of the erupting permanent successors below. The child simultaneously has both primary and permanent teeth.
Critical clinical point: Primary teeth serve as placeholders for permanent teeth. Premature loss leads to adjacent teeth drifting into the gap, misdirecting permanent tooth eruption, inhibiting jaw growth, and creating a discrepancy between upper and lower jaws requiring orthodontic treatment.
Period 3 - Permanent Dentition
Permanent eruption proceeds in three waves with resting periods between each wave. The resting periods allow the dental-facial complex to grow and create space for the next eruption phase.
Wave 1 (Ages 6-9 years)
| Tooth | Age |
|---|---|
| First molars (the "6-year molars") | 6-7 yr |
| Central incisors | 7-8 yr |
| Lateral incisors | 8-9 yr |
Wave 2 (Ages 9-13 years)
| Tooth | Age |
|---|---|
| Canines | 11-13 yr |
| First premolars | 9-11 yr |
| Second premolars | 11-13 yr |
| Second molars (the "12-year molars") | 12-14 yr |
Wave 3 (Ages 17-22+ years)
| Tooth | Age |
|---|---|
| Third molars ("wisdom teeth") | 17-22+ yr (highly variable) |
Full permanent dentition complete: ~14 years, excluding third molars
Clinical Symptoms of Teething (Primary Eruption)
Teething in infants produces a well-recognized symptom cluster:
| Symptom | Frequency |
|---|---|
| Gingival irritation/swelling | 86% |
| Irritability | 68% |
| Drooling | 56% |
| Mildly elevated temperature | Common, but rarely true fever |
Important distinction: Teething may cause a mild temperature elevation but it is not a cause of true fever. Fever during the teething period should be investigated for other causes (e.g., viral illness). Attributing fever solely to teething is a diagnostic error.
- Tintinalli's Emergency Medicine - p. 1622
Tooth Development Begins in Utero
Tooth formation starts at week 6 of embryonic life and continues in stages through adolescence:
| Stage | Timing |
|---|---|
| Enamel organ bud formation | ~6 weeks in utero |
| Crown formation (primary teeth) | Prenatal |
| Crown formation (permanent teeth) | Prenatal to early postnatal |
| Root formation | After birth, continues post-eruption |
| Third molar root closure | Late teens/early 20s |
This explains why systemic illness, nutritional deficiency, or drug exposure (e.g., tetracyclines) during critical periods can produce enamel hypoplasia or discoloration in teeth that have not yet erupted.
Why Timing Varies
Dental eruption timing is influenced by:
- Sex: girls generally erupt teeth slightly earlier than boys
- Genetics: strong heritable component
- Nutrition: malnutrition delays eruption
- Systemic disease: hypothyroidism, Down syndrome, rickets delay eruption; preterm birth may accelerate some stages
- Local factors: early extraction of primary teeth may accelerate or delay permanent eruption depending on timing
Pericoronitis - The Complication of Eruption
When a tooth (most often the lower third molar) only partially erupts, the overlying gingival flap (the operculum) traps food and bacteria beneath it. This triggers pericoronitis - inflammation of the operculum.
- Presents with: pain, swelling, trismus (due to proximity of masticator space), halitosis
- Can spread to parapharyngeal spaces - potentially life-threatening
- Most common in the 2nd-3rd decade during wisdom tooth eruption
- Worsened by impacted or malerupted teeth
- Treatment: irrigation, antibiotics, analgesia; definitive = surgical removal of operculum or tooth
Quick Reference Summary Table
| Period | Age Range | Teeth |
|---|---|---|
| Primary dentition (teething) | 6 months - 3 years | 20 deciduous teeth |
| Mixed dentition | 6-12 years | Primary + permanent together |
| Permanent (Wave 1) | 6-9 years | 1st molars, central + lateral incisors |
| Permanent (Wave 2) | 9-13 years | Canines, premolars, 2nd molars |
| Permanent (Wave 3) | 17-22+ years | 3rd molars (wisdom teeth) |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - Ch. 245, pp. 1621-1622
- Color Atlas of Human Anatomy, Vol. 2: Internal Organs - Table 4.1, p. 273-274
- Forensic Anthropology: A Comprehensive Introduction, 2nd ed. - Table A.1 & A.2, pp. 385-386
- Harrison's Principles of Internal Medicine, 22e - p. 1880
This is a shared conversation. Sign in to Orris to start your own chat.