Muscle relaxers drugs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of muscle relaxant drugs, drawn from Firestein & Kelley's Textbook of Rheumatology, The Essentials of Forensic Medicine and Toxicology (2026), and Morgan & Mikhail's Clinical Anesthesiology.
Muscle Relaxant Drugs
Muscle relaxants fall into two broad categories:
- Centrally acting skeletal muscle relaxants (spasmolytics/antispasmodics) - used for spasticity and musculoskeletal pain
- Neuromuscular blocking agents (NMBAs) - used in anesthesia and ICU settings
Category 1: Centrally Acting Skeletal Muscle Relaxants
These are further split into antispastic agents (for upper motor neuron disorders) and antispasmodic agents (for peripheral musculoskeletal pain).
A. Antispastic Agents (for Spasticity)
Used in multiple sclerosis, spinal cord injury, stroke, traumatic brain injury, and cerebral palsy - conditions where loss of descending inhibition causes muscular hypertonicity ("clasp-knife" phenomenon).
| Drug | Mechanism | Dose | Key Side Effects / Notes |
|---|---|---|---|
| Baclofen (Lioresal) | GABA-B receptor agonist; disrupts polysynaptic and monosynaptic reflexes at spinal cord | 5 mg TID oral, max 80 mg/day; also available intrathecally | Sedation, weakness, hypotension, nausea, depression; withdrawal = hallucinations, seizures; adjust for renal impairment |
| Dantrolene (Dantrium) | Direct muscle action - blocks Ca²+ release from sarcoplasmic reticulum | Up to 800 mg/day | Black box warning: hepatotoxicity; stop after 45 days if no benefit |
| Tizanidine (Zanaflex) | Central alpha-2 adrenergic agonist; reduces excitatory amino acid release from spinal interneurons | 2-4 mg/night, max 36 mg/day | Hypotension, sedation, dry mouth; metabolized via CYP1A2 - contraindicated with ciprofloxacin or fluvoxamine; monitor LFTs; acute withdrawal = hypertension, tachycardia |
| Diazepam (Valium) | Central GABA-A blockade | Variable | First drug used for spasticity; significant sedation, abuse potential, drug interactions - not first-line |
B. Antispasmodic Agents (for Musculoskeletal Pain/Spasms)
Used for fibromyalgia, tension headaches, myofascial pain, and nonspecific back pain - without signs of upper motor neuron disease. Typically restricted to 2-3 weeks of use.
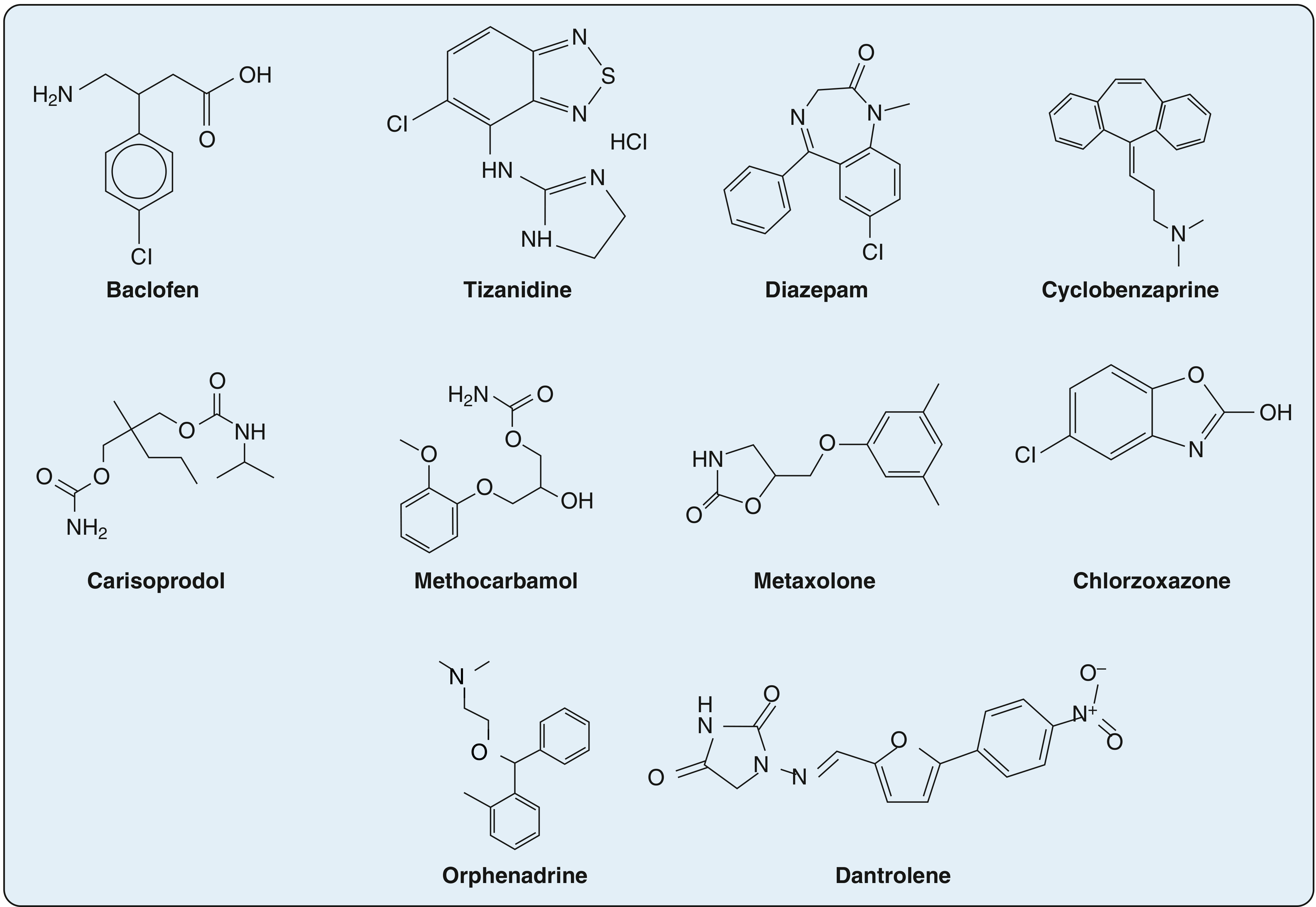
Chemical structures of centrally-acting skeletal muscle relaxants - Firestein & Kelley's Textbook of Rheumatology
| Drug | Mechanism | Dose | Key Notes |
|---|---|---|---|
| Cyclobenzaprine (Flexeril) | Structurally related to TCAs; acts at brainstem to reduce tonic somatic motor activity (alpha + gamma motoneurons); anticholinergic sedation | 5-10 mg TID, max 30 mg/day; also 15/30 mg ER | Contraindicated with MAO inhibitors, in acute MI recovery, arrhythmias, CHF, hyperthyroidism; risk of serotonin syndrome with SSRIs |
| Carisoprodol (Soma) | Alters interneuronal activity in spinal cord and descending reticular formation; metabolized to meprobamate (GABA-A agonist, Schedule IV) | 250 mg QID, max 1400 mg/day | Significant abuse potential; contraindicated in acute intermittent porphyria; CYP2C19 interactions (omeprazole, rifampin) |
| Methocarbamol (Robaxin) | Carbamate derivative of guaifenesin; CNS depressant - no direct muscle action | 500-750 mg QID, max 8 g/day | IV form risk of thrombophlebitis/skin sloughing; caution in myasthenia gravis |
| Metaxalone (Skelaxin) | CNS depression; no direct muscle action | 800 mg TID-QID | Less sedating than others; contraindicated in hemolytic anemia, renal/hepatic impairment |
| Chlorzoxazone (Parafon Forte) | Centrally acting; inhibits multisynaptic reflex arcs at spinal cord and subcortical brain | 250-500 mg TID-QID | Hepatocellular toxicity reported |
| Orphenadrine (Norflex) | Derived from diphenhydramine; strong anticholinergic properties; no direct muscle relaxation | 100 mg BID | Contraindicated in glaucoma, prostatic hyperplasia, myasthenia gravis, peptic ulcer obstruction |
Tizanidine and benzodiazepines are approved for both spasticity and musculoskeletal disorders.
Category 2: Neuromuscular Blocking Agents (NMBAs)
Used in anesthesia, rapid sequence intubation (RSI), mechanical ventilation, and ECT. They block acetylcholine (ACh) at nicotinic receptors at the neuromuscular junction.
A. Depolarizing NMBAs
| Drug | Notes |
|---|---|
| Succinylcholine (Suxamethonium) | Mimics ACh - produces persistent depolarization of the motor endplate; fastest onset of any NMBA; short duration (metabolized by pseudocholinesterase); key risk: malignant hyperthermia, hyperkalemia (dangerous in burns, crush injury, denervation); increases IOP by ~8-10 mmHg |
B. Non-Depolarizing NMBAs
These competitively antagonize ACh at nicotinic receptors and can be reversed with neostigmine/sugammadex.
| Drug | Duration | Notes |
|---|---|---|
| Rocuronium | Intermediate | Can be reversed rapidly with sugammadex; minimal histamine release |
| Vecuronium | Intermediate | Minimal cardiovascular effects; minimal histamine release |
| Atracurium | Intermediate | Hoffman elimination (organ-independent); some histamine release |
| Cisatracurium | Intermediate | Cisatracurium isomer of atracurium; less histamine release; preferred in organ failure |
| Mivacurium | Short-acting | Metabolized by pseudocholinesterase |
| Pancuronium | Long-acting | Tachycardia due to vagolytic effects |
Key Adverse Effects of NMBAs:
- Respiratory: prolonged apnea, paralysis of respiratory muscles
- Cardiovascular: bradyarrhythmia, tachyarrhythmia, hypotension/hypertension
- Histamine-mediated: bronchospasm, vasodilation (mainly with atracurium)
- Metabolic: hyperkalemia (succinylcholine)
- Malignant hyperthermia: triggered by succinylcholine + volatile anesthetics - hypermetabolic crisis with rhabdomyolysis and acute tubular necrosis
- ICU neuromyopathy: prolonged weakness after sustained paralysis (recovery up to 6 months)
Summary Comparison
| Class | Examples | Setting | Reversible? |
|---|---|---|---|
| Antispastic (central) | Baclofen, Dantrolene, Tizanidine, Diazepam | Neurology/Rehab | Yes (oral) |
| Antispasmodic (central) | Cyclobenzaprine, Carisoprodol, Methocarbamol | Primary care/Acute pain | Yes (oral, short-term) |
| Depolarizing NMBA | Succinylcholine | Anesthesia/Emergency | Via pseudocholinesterase |
| Non-depolarizing NMBA | Rocuronium, Vecuronium, Atracurium | Anesthesia/ICU | Yes (neostigmine, sugammadex) |
Key clinical takeaways:
- Skeletal muscle relaxants have no primary role in chronic pain due to limited true muscle effects and significant side effect profiles.
- Most antispasmodic medications are restricted to 2-3 weeks of use, though they are frequently prescribed long-term.
- Meta-analysis evidence supports cyclobenzaprine, tizanidine, carisoprodol, and orphenadrine as superior to placebo for musculoskeletal conditions; evidence for chlorzoxazone, methocarbamol, baclofen, and dantrolene is more limited.
- Sugammadex is the preferred reversal agent for rocuronium/vecuronium in modern anesthesia.
Sources: Firestein & Kelley's Textbook of Rheumatology; The Essentials of Forensic Medicine and Toxicology (2026); Morgan & Mikhail's Clinical Anesthesiology
This is a shared conversation. Sign in to Orris to start your own chat.