45 years old male patients with sugar and Blood pressure getting chest pain & git discomfort what's should be deignoses
chest pain diabetes hypertension acute coronary syndrome diagnosis
Diagnostic Approach: 45-Year-Old Male with Diabetes, Hypertension, Chest Pain & GI Discomfort
Patient Risk Profile at a Glance
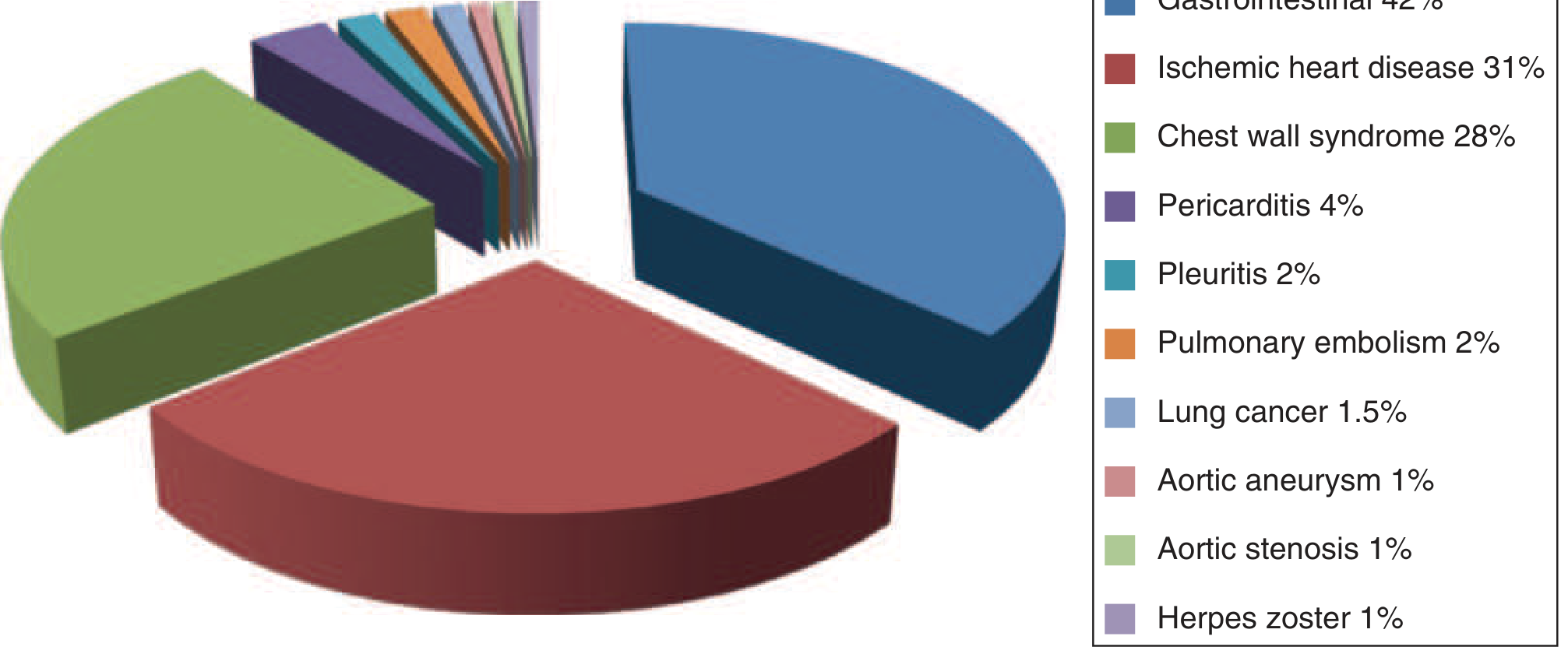
Distribution of Diagnoses in Acute Chest Pain (Reference Chart)
Priority Differential Diagnoses
1. MUST NOT MISS (Life-Threatening) - Rule Out First
| Diagnosis | Why Suspect | Key Features |
|---|---|---|
| Acute Coronary Syndrome (ACS) - STEMI, NSTEMI, Unstable Angina | DM + HTN = high CAD risk; GI sx are a known ACS atypical feature | Pressure/squeezing chest pain, radiation to arm/jaw, nausea, diaphoresis, exertional onset |
| Acute MI (Silent / Atypical) | Diabetics with autonomic neuropathy may present with only GI sx, fatigue or vague discomfort | Minimal or absent classic chest pain; GI sx may dominate |
| Aortic Dissection | HTN is the leading risk factor | Sudden tearing/ripping pain radiating to back, unequal BP in arms |
| Pulmonary Embolism | DM/HTN increase thrombotic risk | Pleuritic pain, dyspnea, tachycardia, hypoxia |
Red flag: Radiation to the right arm/shoulder (LR+ 4.7), both arms (LR+ 4.1), or left arm (LR+ 2.3) and exertional onset (LR+ 2.4) are the highest-risk features for ACS. - Tintinalli's Emergency Medicine
2. HIGH PROBABILITY (Common with This Presentation)
| Diagnosis | Why Suspect | Key Features |
|---|---|---|
| Stable Angina / IHD | Long-standing DM+HTN accelerates atherosclerosis | Predictable exertional chest tightness, relieved by rest, duration 2-10 min |
| Hypertensive Emergency / Crisis | Uncontrolled BP | Very high BP + end-organ damage (chest pain, headache, visual changes) |
| GERD / Esophageal Reflux | Common in middle-aged males; GI discomfort fits | Burning, postprandial, related to posture; heartburn; responds to antacids |
| Peptic Ulcer Disease | DM increases GI vulnerability; NSAIDs use common in HTN | Epigastric burning, worse with food or fasting, relief with antacids |
3. CONSIDER (Less Likely but Important)
| Diagnosis | Features |
|---|---|
| Esophageal Spasm | Severe episodic chest pain mimicking cardiac; GI symptoms overlap |
| Pancreatitis | Epigastric/chest pain radiating to back; nausea/vomiting; DM connection |
| Diabetic Gastroparesis | Chronic DM complication; GI bloating, nausea, early satiety |
| Pericarditis | Sharp retrosternal pain, worse lying flat, relieved sitting forward |
| Musculoskeletal / Chest Wall | Reproducible on palpation, positional |
Recommended Diagnostic Workup
Immediate (Emergency Priority)
| Test | Purpose |
|---|---|
| 12-lead ECG (stat + serial at 0, 3, 6 hrs) | Detect ST elevation, depression, T-wave changes, new LBBB |
| Cardiac Troponin I/T (serial, 0 & 3-6 hrs) | Detect myocardial injury/necrosis - high sensitivity troponin preferred |
| CK-MB | Complementary to troponin |
| Blood pressure (both arms) | Rule out aortic dissection |
| SpO2 + Chest X-Ray | Rule out pulmonary edema, widened mediastinum, pneumothorax |
| CBC, BMP (K+, Cr, glucose) | Baseline; hyperkalemia can cause ECG changes in DM; assess renal function |
| HbA1c | Diabetic control status |
| Lipid panel | CAD risk assessment |
Second-Line (Based on Initial Results)
| Test | Purpose |
|---|---|
| Stress Test / Stress Echo | If troponins negative, evaluate for inducible ischemia |
| CT Pulmonary Angiography | If PE suspected |
| CT Aorta | If aortic dissection suspected |
| Upper GI Endoscopy / PPI trial | If cardiac ruled out and GI cause suspected |
| Esophageal pH monitoring / manometry | If GERD or spasm suspected |
| Abdominal Ultrasound | If gallstones/pancreatitis suspected |
Clinical Decision Logic
Chest pain + DM + HTN
|
↓
[ECG + Troponin STAT]
|
┌───┴───┐
Positive Negative
| |
ACS Repeat at 3-6 hrs
Protocol |
Still negative?
|
Consider: Stress test, GERD, PUD,
Esophageal, PE (if hypoxic),
Dissection (if tearing + BP asymmetry)
Key Clinical Pearls
-
Diabetic patients can have completely atypical or "silent" ACS - GI symptoms, fatigue, or vague discomfort may be the only presentation due to autonomic neuropathy. Never dismiss chest/epigastric discomfort in a diabetic without a proper cardiac workup first. - Rosen's EM; Murray & Nadel's Respiratory Medicine
-
Do not be misled by a GI picture: "Patients with a burning or indigestion-type pain may initially be suspected of having a GI cause; however, because of the visceral nature of chest pain, all causes must be considered." - Rosen's Emergency Medicine, p. 258
-
Antacid response does NOT exclude ACS - 18-45% of ACS patients get pain relief from antacids. Similarly, lack of nitroglycerin response is unreliable (65% of ACS patients do not fully respond). - Tintinalli's Emergency Medicine
-
GERD should only be diagnosed after cardiac causes are excluded - "Cardiac causes should be excluded in patients with chest pain before beginning a GI evaluation." - Symptom to Diagnosis, 4th Ed.
-
Patients with DM + HTN have a ~50% likelihood of coexisting diabetic autonomic neuropathy; myocardial ischemia or old infarction may be evident on ECG despite a negative history. - Morgan & Mikhail's Clinical Anesthesiology 7e
But ECG is normal & bp is 160
Updated Assessment: Normal ECG + BP 160 mmHg
Critical Point: Normal ECG Does NOT Rule Out ACS
"Initial biomarkers of injury may be in the normal range, even in patients with STEMI. Cardiac troponin is the preferred biomarker... Troponin should be measured at presentation and repeated at 1-3 h using high-sensitivity troponin and 3-6 h using conventional troponin assays."
- Harrison's Principles of Internal Medicine 22E
"A single normal serum troponin measurement is insufficient to exclude MI in a patient with a very recent onset of symptoms."
- Goldman-Cecil Medicine
What the Normal ECG + BP 160 Changes
| Finding | Clinical Interpretation |
|---|---|
| ECG normal | STEMI unlikely. NSTEMI/UA still very possible. Proceed with serial troponins. |
| BP = 160 mmHg | Hypertensive urgency (no end-organ damage yet) vs. pain-driven BP spike vs. poorly controlled baseline HTN. Either way, needs BP management. |
| GI discomfort persists | Now rises in differential - GERD, PUD, esophageal spasm. But still secondary until troponin is negative. |
Revised Diagnostic Priority Order
Step 1 - Still Do This NOW (Cannot Skip)
| Test | Why |
|---|---|
| Serial High-Sensitivity Troponin I/T (0 hr + 1-3 hr) | A negative hs-Troponin at 2-3 hrs after symptom onset has a negative predictive value >99% for MI. This is the key gate. - Harrison's 22E |
| Repeat ECG at 3-6 hrs or with any pain recurrence | Dynamic ECG changes (new ST depression, T-wave inversions) may appear later |
| Chest X-Ray | Rule out widened mediastinum (aortic dissection), pulmonary edema (LV failure from HTN) |
| Blood glucose + HbA1c | DM control; hyperglycemia worsens ischemia outcomes |
| Renal function (Cr, eGFR) | HTN-related nephropathy; also affects medication choice |
| Echocardiogram | If ECG is non-diagnostic, echo can detect regional wall motion abnormalities (hypokinesis/akinesis) during pain - strongly suggests ischemia. - Goldman-Cecil Medicine |
Step 2 - After Serial Troponins Are Negative x2
| Test | Purpose |
|---|---|
| Stress Test (Exercise ECG or Stress Echo) | Detect inducible ischemia; defines exercise tolerance. Recommended within 72 hours. - Goldman-Cecil |
| CT Coronary Angiography | High negative predictive value (>98%) for excluding CAD in low-to-intermediate risk; can reduce hospital stay - Goldman-Cecil |
| Upper GI Endoscopy / PPI Trial | GERD, peptic ulcer, esophagitis now become real targets once cardiac ruled out |
| 24-hr Ambulatory BP Monitoring | Assess BP pattern, white-coat effect vs. true uncontrolled HTN |
| Lipid panel, fasting glucose | Complete cardiovascular risk profile |
BP 160 - Immediate Management
- Pain-induced sympathetic surge (will fall if pain treated)
- Poorly controlled baseline HTN
- Possibly hypertensive urgency (no acute end-organ damage based on current info)
- Do NOT aggressively drop BP until ACS is excluded - hypotension in ACS is dangerous
- If troponins are negative and chest X-ray shows no pulmonary edema, begin oral antihypertensive adjustment (optimize existing medications)
- Sublingual nifedipine is NOT recommended for hypertensive urgency (reflex tachycardia risk)
- If ACS confirmed, BP management follows ACS protocol (beta-blockers, nitrates, ACE inhibitors)
Revised Diagnostic Picture
Normal ECG + BP 160 + DM + HTN + Chest Pain + GI discomfort
|
Serial Troponin (MANDATORY)
/ \
Positive (rising) Negative x2
| |
ACS Protocol Stress Test / Echo
(NSTEMI/UA) + GI workup (GERD/PUD)
+ BP management
+ CT Coronary Angio
(if intermediate risk)
Most Likely Diagnoses Right Now (Ranked)
- NSTEMI or Unstable Angina - top priority until troponins exclude it (DM + HTN makes this high pretest probability)
- Hypertensive urgency with chest pain (BP 160 + known HTN)
- GERD / Peptic Ulcer Disease - rises in probability as GI component is prominent and ECG is normal
- Stable angina (CAD) - if troponins are negative, stress test will clarify
- Esophageal spasm - can perfectly mimic cardiac pain with GI symptoms
Now parents take cyra d & unienzyme tab after getting food
Cyra D rabeprazole domperidone uses indications diabetes hypertension
Unienzyme tablet composition uses fungal diastase papain activated charcoal
domperidone QT prolongation cardiac risk hypertension diabetes warning
Medication Review: Cyra-D & Unienzyme in This Patient
What These Drugs Are
Cyra-D (Rabeprazole 20mg + Domperidone 30mg SR)
- Rabeprazole - Proton Pump Inhibitor (PPI): blocks gastric H+/K+-ATPase, suppresses acid production
- Domperidone - Prokinetic: dopamine D2 receptor antagonist, speeds gastric emptying, reduces nausea/bloating
Unienzyme (Fungal Diastase + Papain + Activated Charcoal)
- Fungal Diastase (from Aspergillus oryzae) - breaks down starch
- Papain (from Carica papaya) - proteolytic enzyme, aids protein digestion
- Activated Charcoal 75mg - adsorbs intestinal gas, relieves bloating and flatulence
Clinical Interpretation: What This Treatment Tells Us
| Implied Diagnosis | Evidence from Prescription |
|---|---|
| GERD / Acid Reflux | Rabeprazole (PPI) is first-line for GERD |
| Functional Dyspepsia | Domperidone prokinetic + digestive enzymes = classic dyspepsia regimen |
| Diabetic Gastroparesis | Domperidone is used specifically for delayed gastric emptying in diabetics |
| Bloating / Flatulence | Activated charcoal + fungal diastase target gas and fermentation |
| Post-meal GI discomfort | "After food" instruction = symptom pattern is postprandial |
Is This Prescription Appropriate? - Critical Analysis
Cyra-D: Partially Appropriate, BUT With a Major Warning
- Cardiac causes have been excluded with serial troponins
- GERD/dyspepsia is the confirmed working diagnosis
- Take before food (30 min before meals for best efficacy - this is important, see below)
Domperidone is associated with QT interval prolongation, serious ventricular arrhythmias, and sudden cardiac death. - MedSafe NZ Safety Review | Health Canada Safety Review 2021
| Risk Factor in This Patient | Relevance |
|---|---|
| Male, 45 years | QT risk exists but higher risk is >60 yrs |
| Hypertension | Often associated with LV hypertrophy, which can predispose to arrhythmias |
| Diabetes | Autonomic neuropathy can affect cardiac conduction |
| Chest pain | If any underlying cardiac ischemia present, QT prolongation is dangerous |
| Dose: 30mg SR | The EMA recommends max 10mg x3/day = 30mg/day total - this is at the threshold dose |
Unienzyme - Appropriate and Safe
- No significant drug interactions with current medications
- Activated charcoal can reduce absorption of other drugs if taken simultaneously - should be taken 2 hours apart from other medications, especially antihypertensives and antidiabetics
- Suitable for bloating and indigestion complaints in this patient
- No cardiac risks
Correct Timing Issue - Important Note
| Drug | Correct Timing | Current Instruction |
|---|---|---|
| Cyra-D (Rabeprazole) | 30 min BEFORE food for optimal acid suppression | ❌ "After food" reduces PPI efficacy |
| Unienzyme | With or just after food | ✓ Correct - enzymes work during digestion |
What Still Needs to Be Done
| Pending Action | Reason |
|---|---|
| Serial Troponin (if not done) | Cannot fully exclude NSTEMI without this |
| Check QTc on ECG | Before continuing Domperidone in a cardiac-risk patient |
| Confirm BP control | BP 160 still needs management; check if antihypertensive was also prescribed |
| Review antidiabetic medications | Metformin/insulin/oral agents must be listed to check interactions |
| Check if Activated Charcoal timing is spaced from antihypertensives | Charcoal adsorbs drugs non-selectively |
Summary for the Clinician
Current approach = GI-focused treatment (GERD/Dyspepsia/Gastroparesis)
✓ Reasonable IF cardiac causes excluded
✓ Unienzyme is safe and appropriate
⚠ Rabeprazole should be taken BEFORE food, not after
⚠ Domperidone carries QT prolongation risk - check QTc
⚠ Activated charcoal must be spaced from other medications
❓ Is serial troponin result available/done?
❓ Is antihypertensive also prescribed for BP 160?
But patient has already taken daily medication for sugar and Blood pressure which is glemster m2 & Telmikind amh
Glemstar M2 composition glimepiride metformin diabetes uses
Telmikind AM composition telmisartan amlodipine hypertension uses
glimepiride hypoglycemia chest pain GI symptoms interaction domperidone rabeprazole
Complete Medication Review - Full Drug Profile
All 4 Medications at a Glance
| Drug | Brand | Class | Indication |
|---|---|---|---|
| Glimepiride 2mg + Metformin 500mg | Glemstar M2 | Sulfonylurea + Biguanide | Type 2 Diabetes |
| Telmisartan 40mg + Amlodipine 5mg | Telmikind AM | ARB + CCB | Hypertension |
| Rabeprazole 20mg + Domperidone 30mg | Cyra-D | PPI + Prokinetic | GERD / Dyspepsia |
| Fungal Diastase + Papain + Charcoal | Unienzyme | Digestive enzyme | Bloating / Indigestion |
How Each Drug Works
Glemstar M2 (Glimepiride 2mg + Metformin 500mg)
- Glimepiride (Sulfonylurea): stimulates pancreatic beta-cells to release insulin regardless of blood glucose level - risk of hypoglycemia even if patient eats late or skips a meal
- Metformin: reduces hepatic glucose output, improves insulin sensitivity - does NOT cause hypoglycemia alone, but potentiates glimepiride-induced hypoglycemia
- Taken: typically with or just before food to reduce GI side effects of metformin (nausea, bloating, diarrhoea)
Telmikind AM (Telmisartan 40mg + Amlodipine 5mg)
- Telmisartan (ARB - Angiotensin Receptor Blocker): blocks AT1 receptors, reduces vasoconstriction and aldosterone release; also has PPAR-gamma agonist activity (beneficial mild insulin-sensitizing effect)
- Amlodipine (Calcium Channel Blocker): relaxes vascular smooth muscle, reduces peripheral resistance; also reduces coronary vasospasm - has mild antianginal effect
- BP still 160 mmHg despite this combination - suggests inadequate control or poor adherence
Critical Drug Interaction Analysis
⚠ ALERT 1: Hypoglycemia Risk - Glimepiride + Domperidone
- Postprandial hypoglycemia (low sugar 2-3 hrs after eating)
- Hypoglycemia symptoms: sweating, palpitations, chest pain, GI discomfort - which can mimic or worsen the patient's presenting complaints
This is clinically important: Some of this patient's chest pain and GI discomfort may actually be hypoglycemia symptoms, not GERD or cardiac disease.
⚠ ALERT 2: Activated Charcoal (Unienzyme) - Absorbs Everything
- Glimepiride (less sugar control)
- Metformin
- Telmisartan / Amlodipine (less BP control - explains BP 160!)
⚠ ALERT 3: Domperidone QTc Risk (Revisited)
- Amlodipine is generally safe with domperidone
- But telmisartan + domperidone together slightly increase QT risk
- Check QTc on ECG before continuing domperidone long-term
✓ SAFE Combinations
| Pair | Status |
|---|---|
| Telmisartan + Metformin | Safe; telmisartan may modestly improve insulin sensitivity |
| Amlodipine + Glimepiride | Safe; no significant interaction |
| Rabeprazole + Telmisartan | Safe |
| Rabeprazole + Metformin | Safe |
Timing Schedule - Optimised
| Time | Medication | Notes |
|---|---|---|
| Morning - 30 min before breakfast | Cyra-D (Rabeprazole + Domperidone) | PPI must be before food to work properly |
| With breakfast | Glemstar M2 (Glimepiride + Metformin) | Take with first bite; metformin with food reduces nausea |
| With breakfast or morning | Telmikind AM | Once daily, same time every day |
| 2 hours after breakfast (or with lunch/dinner) | Unienzyme | Must be separated from all other medications |
Why BP is Still 160 - Possible Reasons
- Activated charcoal (Unienzyme) taken at same time as Telmikind AM - absorbing the antihypertensive before it is absorbed
- Poor medication adherence - "forgot today's dose" before symptoms started
- Pain/anxiety-driven sympathetic surge - BP elevated reactively due to chest pain
- Subtherapeutic dose - Telmisartan 40mg + Amlodipine 5mg may be insufficient; dose escalation needed
- Uncontrolled diabetes contributing - chronic hyperglycemia causes vascular stiffness
New Differential Diagnosis to Add
| New Diagnosis | Mechanism |
|---|---|
| Hypoglycemia episode | Glimepiride + domperidone (faster absorption) + possibly late/missed meal = low blood sugar causing chest pain, sweating, palpitations, GI discomfort |
Summary - Complete Patient Medication Map
TYPE 2 DIABETES
Glemstar M2 (Glimepiride 2mg + Metformin 500mg)
+ Domperidone (from Cyra-D)
↓
⚠ Risk of hypoglycemia → can cause chest pain + GI sx
⚠ Check blood glucose NOW
HYPERTENSION (BP 160 despite treatment)
Telmikind AM (Telmisartan 40mg + Amlodipine 5mg)
+ Unienzyme charcoal (if taken together)
↓
⚠ Charcoal may be absorbing antihypertensive → explains poor BP control
⚠ Space medications 2 hrs apart
GI SYMPTOMS
Cyra-D (Rabeprazole before food ✓ | Domperidone after food ✓)
Unienzyme (after food ✓ but space from other drugs)
CARDIAC SAFETY
⚠ Domperidone QTc risk - check ECG QTc interval
⚠ Serial troponins still needed if not done
Now what should I do
Immediate Action Plan - What To Do Right Now
Step 1 - Bedside Checks (Next 5 Minutes)
| Action | Why |
|---|---|
| Fingerstick Blood Glucose | Rule out hypoglycemia as cause of chest pain + GI sx (glimepiride risk) |
| Check BP both arms | Rule out aortic dissection; confirm true BP reading |
| SpO2 (pulse oximetry) | Rule out PE / pulmonary cause |
| Ask: Is chest pain at rest or exertional? Any radiation to arm/jaw? | Refine cardiac risk immediately |
| Ask: When was last meal and last Glemstar M2 dose? | Timing gap = hypoglycemia risk |
Step 2 - Laboratory (Same Visit / Emergency)
| Test | Priority | Why |
|---|---|---|
| Serial Troponin I/T (NOW + repeat at 3 hrs) | 🔴 URGENT | Cannot exclude NSTEMI without this |
| 12-lead ECG (repeat if first was done >3 hrs ago) | 🔴 URGENT | Dynamic changes may appear later |
| Fasting / Random Blood Glucose + HbA1c | 🔴 URGENT | Assess diabetic control, rule out hypo/hyperglycemia |
| Renal Function (Cr, eGFR, BUN) | 🟡 Important | Metformin safety; hypertensive nephropathy |
| Electrolytes (K+, Na+) | 🟡 Important | Telmisartan can raise K+; affects QTc |
| Lipid Panel | 🟢 Routine | Complete CVD risk profile |
| CBC | 🟢 Routine | Anaemia can worsen angina |
| Liver Function Tests | 🟢 Routine | Baseline before long-term PPI/medications |
Step 3 - Immediate Medical Decisions
If Troponin is POSITIVE (Rising) → ACS Protocol
- Admit to coronary care / monitored bed
- Aspirin 325mg loading dose (unless contraindicated)
- Refer to cardiology immediately
- Stop domperidone - cardiac monitoring needed
- Continue Telmikind AM (ARBs + CCBs are cardioprotective post-ACS)
- Hold Metformin if contrast imaging (angiography) is planned
If Troponin is NEGATIVE x2 + No ECG changes
- Outpatient stress test / stress echo within 72 hours
- Continue GI treatment but fix medication timing (see below)
- Optimize BP - consider dose escalation of Telmikind AM to 80mg telmisartan
- Follow up in 1 week
Step 4 - Fix Medication Timing TODAY
| Time | Medicine | Change Needed |
|---|---|---|
| 7:00 AM - Empty stomach | Cyra-D | ⚠ Change from "after food" to 30 min BEFORE breakfast |
| 7:30 AM - With breakfast | Glemstar M2 | ✓ Correct - with food |
| 7:30 AM - With breakfast | Telmikind AM | ✓ Once daily, same time |
| 9:30 AM (2 hrs after breakfast) | Unienzyme | ⚠ Must be separated from all other drugs - charcoal absorbs them |
Step 5 - Patient Counselling Points (Tell the Patient)
- Never skip or delay a meal after taking Glemstar M2 - glimepiride will cause hypoglycemia (dizzy, sweating, chest tightness)
- Take Cyra-D before food - not after - otherwise it does not work
- Do NOT take Unienzyme with other tablets - take it 2 hours separately
- Monitor BP at home daily - morning before medications, record readings
- Check blood sugar daily - fasting (before breakfast) and 2 hours after meals
- Return immediately if: chest pain worsens, pain radiates to arm or jaw, sweating, breathlessness, or fainting
Step 6 - Follow-Up Plan
| Timeline | Action |
|---|---|
| Today | Troponin x2, ECG repeat, glucose check, fix medication timing |
| Within 72 hours | Stress test (if troponins negative) |
| 1 week | Review BP (should be lower with correct Telmikind timing), recheck fasting glucose |
| 1 month | HbA1c, lipid panel review, assess if Telmikind dose needs escalation |
| 3 months | Full diabetic + cardiovascular risk review |
One-Line Summary
Right now: check fingerstick glucose + serial troponin + repeat ECG. Fix medication timing today. If troponin positive → admit for ACS. If negative → stress test within 3 days + optimize BP and sugar control as outpatient.