Treatment for dengue fever
Reading File
Finding Sources
Searching PubMed
dengue fever treatment management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
WHO dengue treatment guidelines 2024 2025 management
Loading Image
I now have everything needed for a thorough, well-sourced answer.
Treatment of Dengue Fever
There is no specific antiviral therapy for dengue. Management is entirely supportive and guided by disease severity. - Red Book 2021, p. 523; Rosen's Emergency Medicine, p. 2630; Washington Manual of Medical Therapeutics, p. 570
WHO Classification of Dengue Severity
The 2009 WHO framework divides dengue into three categories:
| Category | Definition |
|---|---|
| Dengue without warning signs | Fever + ≥2 of: nausea/vomiting, rash, aches/pains, leukopenia, positive tourniquet test |
| Dengue with warning signs | Above + abdominal pain/tenderness, persistent vomiting, fluid accumulation (ascites/pleural effusion), mucosal bleeding, lethargy, liver enlargement >2 cm |
| Severe dengue | Severe plasma leakage leading to shock, respiratory distress, severe bleeding, or severe organ involvement (AST/ALT ≥1000 IU/L, impaired consciousness, organ failure) |
- Red Book 2021, p. 520
Phases of Illness
- Febrile phase (days 1-7): Fever, myalgia, headache, retro-orbital pain, rash, leukopenia
- Critical phase (days 3-7, around defervescence): Risk of plasma leakage, hemoconcentration - lasts 24-48 hours
- Convalescent phase: Gradual improvement; watch for fluid reabsorption and overload
1. Uncomplicated Dengue Fever (Outpatient)
For patients tolerating oral fluids and urinating at least every 6 hours with no warning signs:
-
Fluids: Oral rehydration solution (ORS), fruit juices, electrolyte-containing drinks. Adequate oral hydration reduces hospitalizations.
-
Antipyretics: Paracetamol (acetaminophen) to keep temperature below 39°C; interval no less than 6 hours.
-
Avoid: Aspirin, ibuprofen, and all NSAIDs - these increase bleeding risk and aspirin is associated with Reye's syndrome in children.
-
Return precautions: Patients should return immediately if they develop severe abdominal pain, persistent vomiting, cold/clammy extremities, altered sensorium, bleeding, or no urine for >4-6 hours.
-
Park's Textbook of Preventive and Social Medicine, p. 295; Red Book 2021, p. 523
2. Dengue Hemorrhagic Fever (DHF) Grades I & II - Hospitalized
- Continue paracetamol for fever control
- Oral fluids as tolerated; IV fluids if vomiting persistently
- Monitor haematocrit daily from day 3 onwards - rising Hct signals plasma leakage and need for IV fluids
- IV fluids if Hct rises ≥20%: Start crystalloid (e.g., Lactated Ringer's) at 6 ml/kg/h for 1-2 hours, then reassess
IV fluid algorithm for DHF Grades I & II:
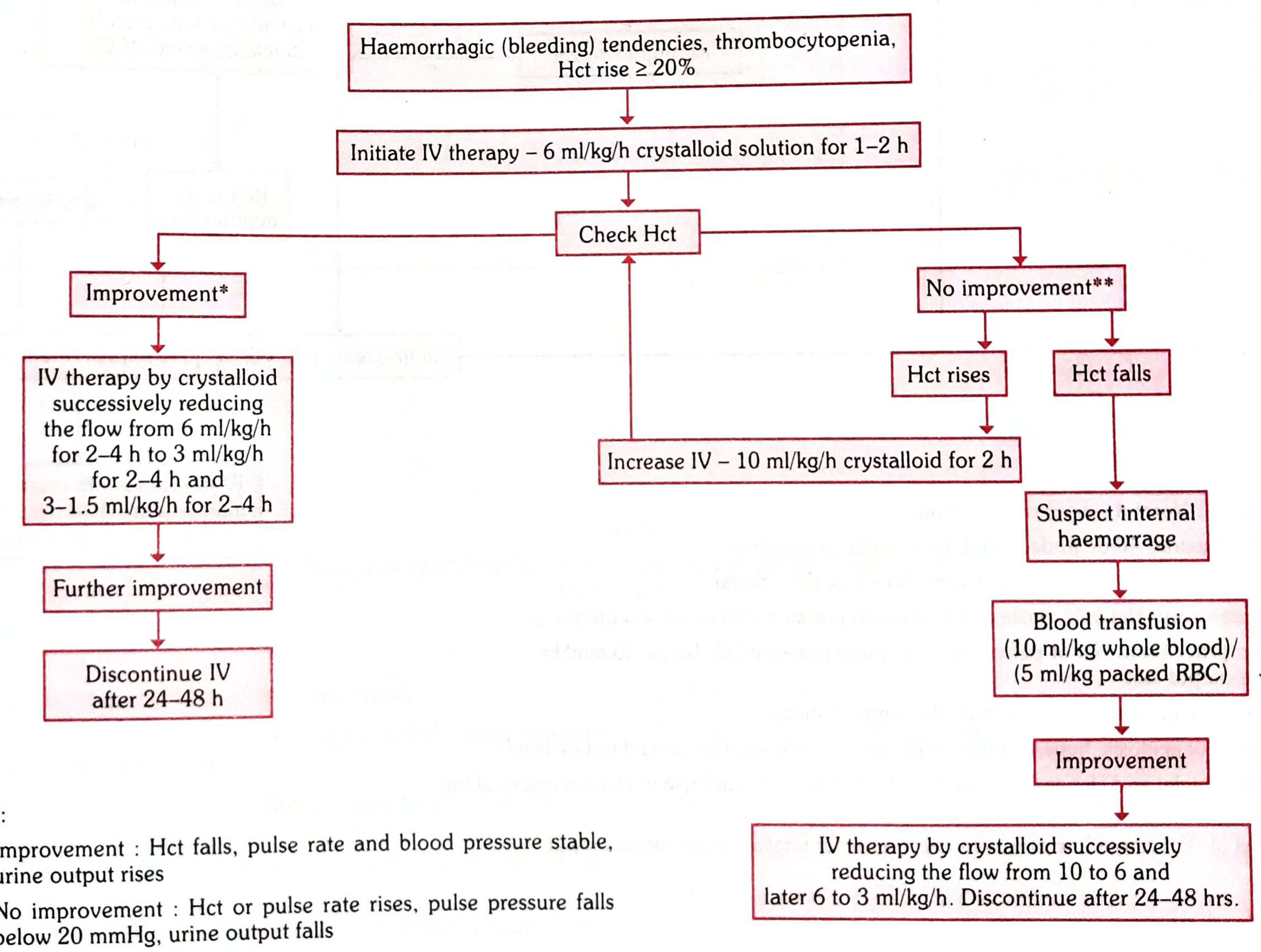
-
If improvement (Hct falls, BP stable, urine output rises): taper IV fluids 6 → 3 → 1.5 ml/kg/h, discontinue after 24-48 hours
-
If no improvement and Hct rises further: increase to 10 ml/kg/h crystalloid for 2 hours
-
If no improvement and Hct falls: suspect internal haemorrhage - blood transfusion (10 ml/kg whole blood or 5 ml/kg packed RBCs)
-
Park's Textbook of Preventive and Social Medicine, pp. 295-296
3. Severe Dengue / DHF Grades III & IV / Dengue Shock Syndrome (DSS)
- ICU admission required
- Immediate haematocrit, platelet count, and vital signs on arrival
- IV fluid resuscitation promptly
- If >1000 ml of IV crystalloid already given with ongoing shock: switch to colloid (Dextran 40 or haemaccel)
- If Hct is declining: fresh whole blood 10-20 ml/kg/h
- Oxygen for all patients in shock
- In refractory shock with declining Hct: suspect occult internal bleeding; give fresh whole blood as a routine precaution (10 ml/kg/h)
Indications for red cell transfusion:
- Overt blood loss ≥10% of total blood volume
- Refractory shock with declining Hct despite adequate fluids
- 10 ml/kg body weight at a time; check coagulogram
- If fluid overload present: use packed RBCs instead of whole blood
- Park's Textbook of Preventive and Social Medicine, p. 296
Key principle: Early recognition of shock and intensive supportive therapy can reduce the case fatality rate from 5-10% down to less than 1%. - Red Book 2021, p. 523
4. Monitoring Parameters
- Temperature pattern
- Fluid intake and output (urine volume and frequency)
- Warning signs (any of the above)
- Serial haematocrit (the key guide to fluid therapy)
- Platelet count and WBC
- Signs of plasma leakage (rising Hct, pleural effusion, ascites)
- Watch for fluid overload during convalescence - reabsorption of extravascular fluid causes Hct to fall; diuresis may be needed
5. What to Avoid
| Drug | Reason to Avoid |
|---|---|
| Aspirin | Increases bleeding risk; Reye's syndrome in children |
| NSAIDs (ibuprofen, etc.) | Aggravates gastritis and bleeding tendencies |
| Corticosteroids | Evidence from studies is inconclusive; not currently recommended |
- Rosen's Emergency Medicine, p. 2630; Red Book 2021, p. 523
6. Disposition
- Outpatient: Uncomplicated dengue with adequate oral intake and no warning signs
- Hospital ward: DHF, dehydration, warning signs present, need for IV rehydration
- ICU: Dengue shock syndrome (DSS), Grade III/IV DHF
7. Vaccine (Prevention)
Dengvaxia (CYD-TDV): A recombinant live attenuated tetravalent vaccine approved in the US for individuals aged 9-16 years who live in dengue-endemic areas AND have laboratory-confirmed prior dengue infection. It is contraindicated in dengue-naive individuals as it may increase the risk of severe dengue on subsequent natural infection. - Red Book 2021, pp. 523-524
Recent evidence note: A 2025 systematic review (PMID 41037858) confirms current supportive-care-only management remains the standard with no approved antiviral therapy, consistent with the above guidelines.
Search for recent research on dengue antiviral drug candidates
Reading File
Searching PubMed
dengue antiviral drug candidates clinical trial
Searching the Web
dengue antiviral drug candidates 2024 2025 clinical trials pipeline
Reading Article
PMID: 42247469
Reading Article
PMID: 41561567
Reading Article
PMID: 39274895
Searching PubMed
dengue antiviral NS3 NS5 protease inhibitor direct-acting
Searching PubMed
dengue virus NS4B NS5 inhibitor JNJ EYU688 mosnodenvir
Searching PubMed
dengue antiviral molnupiravir favipiravir ivermectin repurposing
Reading Web Page
https://journals.plos.org/plosntds/article?id=10.1371%2Fjour…
I now have highly detailed information from the most up-to-date sources (including a June 2026 systematic review and a May 2026 INTREPID Alliance landscape report). Let me compile a thorough answer.
Recent Research on Dengue Antiviral Drug Candidates
The short story: no antiviral has yet been approved or proven effective in clinical trials for dengue. But the pipeline is more active than ever, with both repurposed drugs and novel direct-acting antivirals advancing in 2025-2026.
1. The State of Play - What the Evidence Says
A June 2026 systematic mapping review by Huyen et al. analyzed 121 clinical studies across the entire dengue therapeutics landscape and found:
- Of 10 antiviral trials identified, none demonstrated statistically significant virological or clinical benefit
- All published antiviral RCTs tested repurposed drugs, not dengue-specific compounds
- 45% of published trials had high or critical risk of bias
- Non-standardized endpoints across trials have made meta-analysis impossible
- The authors conclude that dengue-specific direct-acting antivirals are the most promising path forward, rather than repurposing
"Progress in this field will likely depend on the development of dengue-specific direct-acting antivirals, rather than relying on repurposed treatments." - Huyen et al., PLoS NTDs, 2026 [PMID: 42247469]
2. Repurposed Drugs That Have Been Clinically Tested
| Drug | Original Use | Dengue Target | Trial Result |
|---|---|---|---|
| Ivermectin | Antiparasitic | Inhibits NS3 helicase; blocks nuclear transport | 2 RCTs - no significant antiviral or clinical benefit |
| Chloroquine | Antimalarial | Endosomal acidification inhibition | 1 RCT - no significant benefit |
| Celgosivir | Alpha-glucosidase inhibitor (HCV) | ER glycoprotein processing | 1 RCT - no significant benefit |
| Balapiravir | Nucleoside analogue (HCV) | NS5 RNA polymerase inhibition | 1 RCT - no significant benefit |
None of these have demonstrated efficacy. - Huyen et al. (PMID 42247469)
3. Direct-Acting Antivirals in Clinical Development (2024-2026)
EYU688 (Novartis) - Phase 2 ONGOING
- Target: NS4B protein (viral replication complex)
- Status: Phase 2 dose-ranging trial (ClinicalTrials.gov: NCT060066559) - currently ongoing as of mid-2026
- Significance: One of the only dengue-specific small-molecule inhibitors currently in active Phase 2 trials
- Listed in the INTREPID Alliance 5th Edition Landscape (May 2026)
Mosnodenvir (KU Leuven, Belgium) - Phase 2
- Target: NS3/4B replication complex
- Status: Phase 2 clinical trial active as of January 2026 (INTREPID 5th Edition)
- Developed at Katholieke Universiteit Leuven
Molnupiravir (Brazil trial) - Phase 2 ONGOING
- Target: Viral RNA polymerase (broad-spectrum nucleoside analogue, originally for COVID-19/influenza)
- Status: Phase 2 trial for dengue and chikungunya ongoing in Brazil (Brazilian Clinical Trials Registry: U1111-1306-1425)
- A repurposing effort leveraging its broad-spectrum mechanism
Dengue Monoclonal Antibody - SII (Serum Institute of India) - Phase 2 COMPLETED
- Target: Dengue virus envelope protein (passive immunotherapy)
- Phase 2 dose-ranging trial completed; results pending publication (CTRI/2021/07/035290)
4. Drugs That Were Terminated
Two promising Phase 2 trials were terminated early due to industry deprioritization - a major setback for the field:
- AT-752 (Atea Pharmaceuticals) - nucleotide prodrug inhibitor of DENV NS5 polymerase (NCT05466240) - terminated, recruitment challenges + sponsor deprioritization
- JNJ-64281802 (Janssen/J&J) - NS3-NS4B inhibitor (NCT04906980) - terminated October 2024 as part of J&J's "strategic reprioritization" of infectious disease programs
This highlights a recurring problem: pharmaceutical companies withdrawing from dengue R&D due to insufficient financial incentives.
5. Preclinical Pipeline Highlights (from Molecules Review, 2024)
Per Cavina et al. [PMID: 39274895], several NS2B-NS3 protease inhibitors show preclinical promise:
| Compound | Target | Status |
|---|---|---|
| Compound 71 | NS2B-NS3 protease (competitive inhibitor) | Top preclinical candidate - high cellular efficacy, low cytotoxicity, favorable PK |
| SYC-1307 | NS2B-NS3 (allosteric inhibitor) | High in vivo efficacy in animal models |
| Temoporfin / Methylene blue | NS2B-NS3 (orthosteric, non-competitive) | Promising preclinical data |
| Doxycycline | NS2B-NS3 inhibition proposed | Only NS2B-NS3 inhibitor that has reached clinical trials; mechanism/efficacy still uncertain |
6. Novel Approaches in Early Discovery (INTREPID 5th Edition, 2026)
- MLT201 (Meletios Therapeutics) - exploits defective viral genome (DVG) biology; novel mechanism; hit-stage
- Protinhi viral protease inhibitors (Protinhi) - two pan-flavivirus broad-spectrum candidates; hit-stage
- Pan-flavivirus broad-spectrum antivirals - targeting dengue alongside Zika, WNV, yellow fever
7. The Key Challenge: Narrow Treatment Window
A core scientific problem identified by the Dengue Therapeutics Consortium 2025 [PMID: 41561567] is that the window for antiviral intervention is very narrow. Most patients present late in the febrile phase when viral load is already falling - antivirals must be given very early (days 1-3) to make a meaningful difference. This has led to proposals for:
- Human challenge models (controlled infection studies) to rapidly screen antiviral activity
- Viral clearance rate studies as surrogate endpoints before large Phase 3 trials
- Factorial randomization designs to test multiple drugs simultaneously
- Europe's DG HERA committing EUR 20 million to advance at least two new dengue medicines
Summary
| Category | Examples | Status |
|---|---|---|
| Approved antivirals | None | - |
| Active Phase 2 | EYU688 (Novartis), Mosnodenvir, Molnupiravir (Brazil) | Ongoing |
| Phase 2 completed, results pending | Dengue mAb (SII) | Awaiting publication |
| Terminated Phase 2 | AT-752, JNJ-64281802 | Withdrawn 2024 |
| Repurposed - failed RCTs | Ivermectin, chloroquine, celgosivir, balapiravir | No benefit shown |
| Leading preclinical | Compound 71, SYC-1307 | Animal models |
| Early discovery | MLT201, Protinhi compounds | Hit stage |
The field has renewed momentum after years of industry neglect, with EYU688 and mosnodenvir being the most advanced dengue-specific compounds currently in trials. Sustained public funding and international collaboration (Dengue Therapeutics Consortium, INTREPID Alliance, EU/HERA) are filling the gap left by pharmaceutical withdrawals.
This is a shared conversation. Sign in to Orris to start your own chat.