optic neuritis
Reading File
Finding Sources
Searching PubMed
"optic neuritis"[MeSH Terms] AND diagnosis AND treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive, high-quality content from multiple authoritative sources. Here is the full synthesis:
Optic Neuritis
Definition and Pathophysiology
Optic neuritis (ON) is an inflammatory optic neuropathy most commonly caused by demyelinating disease. The pathobiology mirrors that of multiple sclerosis (MS) - idiopathic inflammatory demyelination of the optic nerve followed by secondary axonal injury. It typically involves the retrobulbar portion of the nerve, though the optic nerve head (papillitis) may also be affected.
Etiology
ON is not a single disease but a syndrome with several underlying causes:
| Cause | Notes |
|---|---|
| Multiple sclerosis | Most common association (50-75%) |
| Idiopathic | 25-50% of cases |
| Neuromyelitis Optica Spectrum Disorder (NMOSD) | AQP4-IgG positive; bilateral, severe, tends to not recover |
| MOGAD | MOG-IgG positive; bilateral synchronous ON; papillitis common |
| Infections | Measles, mumps, varicella, herpes zoster, EBV, syphilis, TB, cryptococcus, Lyme disease, HIV |
| Inflammatory/systemic | Sarcoidosis, SLE, Sjogren syndrome, chronic relapsing inflammatory optic neuropathy (CRION) |
| Post-vaccination | Rare, reported after childhood vaccines |
| Contiguous spread | From meningitis, orbital cellulitis, sinusitis |
- Goldman-Cecil Medicine, p. 1328
- Tintinalli's Emergency Medicine, p. 706
Clinical Features
Typical presentation:
- Monocular visual loss developing over hours to a few days (bilateral in NMOSD/MOGAD)
- Periorbital/brow pain worsening with lateral eye movement - present in ~90% of cases; typically lasts 3-5 days
- Decreased color vision and contrast sensitivity - often disproportionately more affected than acuity (red desaturation test)
- Visual field defects - diffuse or discrete scotomas (non-specific)
Examination findings:
- Afferent pupillary defect (APD/RAPD) - commonly present
- Fundoscopy:
- Normal in ~two-thirds (retrobulbar neuritis)
- Mild disc edema (papillitis) in ~one-third - less prominent than papilledema
- No hemorrhages or cotton-wool spots in typical ON (their presence suggests another diagnosis)
- OCT - atrophy of retinal nerve fiber layer (RNFL) and ganglion cell layer develops over weeks after acute episode; reliable structural marker
Pain duration > 7 days should prompt consideration of alternative diagnoses.
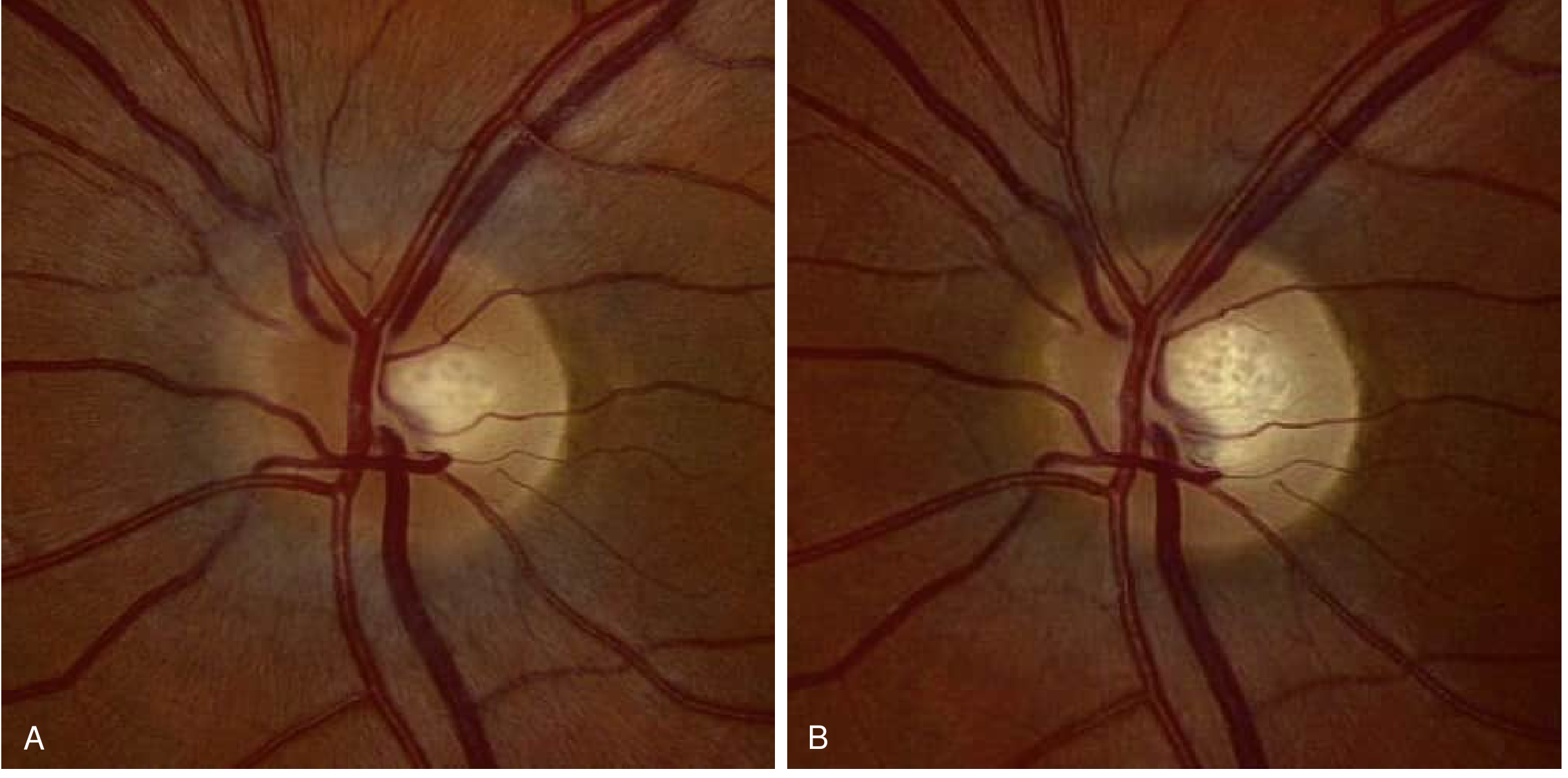
Fig. 16.20 - Bradley & Daroff's Neurology: (A) Acute left optic neuritis with mild nasal nerve fiber layer edema, without hemorrhages. (B) Same eye 3 months later - resolution of edema with mild temporal pallor, indicating axonal loss.
MOGAD vs. MS vs. NMOSD - Key Differentiating Features in Optic Neuritis
| Feature | MS-associated ON | NMOSD (AQP4+) | MOGAD |
|---|---|---|---|
| Laterality | Unilateral | Bilateral, severe | Bilateral, synchronous |
| Papillitis on fundoscopy | Variable, usually unilateral | Rare | Common |
| MRI optic nerve | Short, posterior | Long, chiasmal | Longitudinally extensive, perineural sheath enhancement |
| Visual recovery | Good | Poor | Usually good |
| CSF oligoclonal bands | Present (~85%) | Present (~20%) | Rare (~6-13%) |
| Antibody | - | AQP4-IgG | MOG-IgG (cell-based assay) |
- Harrison's Principles 22E, p. 3001-3023
- Bradley & Daroff's Neurology, p. 3175-3182
Risk of Progression to MS
The Optic Neuritis Treatment Trial (ONTT) - the landmark dataset:
-
Brain MRI with ≥1 characteristic lesion at onset: 72% risk of MS at 15 years
-
Normal brain MRI at onset: 25% risk of MS at 15 years
-
Atypical features (painless loss, severe disc edema, disc/peripapillary hemorrhages, macular exudate) = negligible MS risk
-
Bradley & Daroff's Neurology, p. 3167
Differential Diagnosis
- Anterior ischemic optic neuropathy (AION): sudden onset, painless, age >50, pallid disc edema
- Papilledema: bilateral, painless, preserved visual acuity (early)
- Compressive optic neuropathy: orbital tumor (proptosis), intracranial tumor
- Hypertensive retinopathy
- Hereditary optic neuropathies: Leber hereditary optic neuropathy (LHON), Charcot-Marie-Tooth 2a
- Toxic/metabolic: alcohol, tobacco, heavy metals, chloroquine
Investigations
- MRI brain and orbits - most important for prognosis and MS risk stratification; orbital MRI with fat suppression shows optic nerve signal change
- Visual fields (Humphrey perimetry)
- Color vision testing
- OCT - RNFL and ganglion cell layer thinning
- VEP (Visual Evoked Potentials) - delayed P100
- Serum AQP4-IgG - screen for NMOSD
- Serum MOG-IgG (cell-based assay) - screen for MOGAD; CSF MOG-IgG if seronegative but suspected
- CSF - oligoclonal bands (supports MS), pleocytosis
- Where indicated: ANA, ANCA, ACE (sarcoidosis), RPR/VDRL, Lyme serology, HIV
Treatment
Acute Phase
- High-dose IV methylprednisolone (1 g/day for 3 days) - hastens visual recovery but does not significantly affect long-term visual outcome
- Oral prednisone alone (1 mg/kg) - AVOID - associated with increased risk of recurrence of ON without providing benefit (ONTT finding)
- Plasmapheresis - may be beneficial in acute NMOSD/MOGAD unresponsive to steroids
Long-term
-
MS disease-modifying therapy (interferon-beta, natalizumab, etc.) - indicated for high-risk patients (≥1 MRI lesion) to reduce risk of conversion to MS
-
NMOSD (AQP4+): Immunosuppressants; FDA-approved agents include eculizumab, inebilizumab, and satralizumab
-
MOGAD: Typically treated with steroids ± mycophenolate/azathioprine for relapsing disease; differs from MS - avoid MS DMTs
-
Bradley & Daroff's Neurology, p. 3171-3173
-
Goldman-Cecil Medicine, p. 1338
Prognosis
- Visual recovery begins within 1 month in typical ON
- Prognosis correlates with severity of initial deficit
- Post-episode: optic nerve pallor (temporal pallor) on fundoscopy is expected - reflects axonal loss
- NMOSD-associated ON carries a significantly worse visual prognosis than MS-associated or idiopathic ON
Recent Evidence (2024-2026)
Recent systematic reviews are refining the ability to distinguish MS, NMOSD, and MOGAD using MRI lesion characteristics. A 2025 meta-analysis in JNNP examined MRI lesion distribution criteria for differentiating all three conditions, and a 2024 systematic review in J. Neurol analyzed MRI-based biomarkers. A 2025 systematic review on herpes zoster-associated ON highlights that infectious ON deserves dedicated workup, particularly in immunocompromised patients.
Sources: Bradley & Daroff's Neurology in Clinical Practice | Goldman-Cecil Medicine | Harrison's Principles 22E | Tintinalli's Emergency Medicine | Kanski's Clinical Ophthalmology 10e
episcleritis in ophtha ak khurana
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have all the content needed. Note that AK Khurana's Comprehensive Ophthalmology is not in our textbook library. I'll clearly note this and provide the answer from the best available ophthalmology references (Kanski's Clinical Ophthalmology 10th edition and Wills Eye Manual), which cover the same content as Khurana.
Episcleritis
Note: AK Khurana's Comprehensive Ophthalmology is not available in this library. The following is compiled from Kanski's Clinical Ophthalmology (10th ed.) and the Wills Eye Manual - two leading ophthalmology references that cover this topic in the same depth as Khurana.
Anatomy Relevant to Episcleritis
The episclera has three pre-equatorial vascular layers:
| Layer | Location | Notes |
|---|---|---|
| Conjunctival vessels | Most superficial | Arteries tortuous, veins straight |
| Superficial episcleral plexus | Radial, straight configuration | Maximal congestion in episcleritis - blanches with phenylephrine 2.5% and 10% |
| Deep vascular plexus | Superficial sclera | Maximal congestion in scleritis - purplish hue; does NOT blanch |
- Kanski's Clinical Ophthalmology 10e, p. 306
Definition
Episcleritis is a common, usually idiopathic, benign, recurrent, and frequently bilateral condition involving inflammation of the episcleral tissue (between the conjunctiva/Tenon's capsule and the sclera). It is typically self-limiting, lasting a few days to 3 weeks.
- More common in females (except in children, where it is rare)
- Average patient is middle-aged
Etiology
| Category | Examples |
|---|---|
| Idiopathic | Most common - ~60% have no systemic disease |
| Collagen vascular | Rheumatoid arthritis, SLE, ankylosing spondylitis, psoriatic arthritis |
| Infectious | Herpes zoster ophthalmicus, STIs, protozoa |
| GI/metabolic | Crohn disease, gout |
| Skin | Rosacea, atopy |
| Ocular causes | Dry eye, contact lens wear |
| Drugs/medications | Various |
Types of Episcleritis
1. Simple Episcleritis (75% of cases)
Clinical features:
- More acute onset; features often peak within 24 hours, then gradually fade
- Recurs in ~60% of cases (frequency decreases with time)
-
50% of cases are simultaneously bilateral
- Redness is sectoral (triangular, base at limbus) or diffuse - interpalpebral distribution
- Symptoms range from absent (up to 50%) to moderate - grittiness, mild photophobia
- Visual acuity: normal
- Chemosis, raised IOP, anterior uveitis, keratitis - all rare
2. Nodular Episcleritis (25% of cases)
Clinical features:
- Affects females > males; less acute onset, more prolonged course than simple variant
- Red eye first noted on waking; redness enlarges and becomes uncomfortable over 2-3 days
- Tender, red vascular nodule - almost always within the interpalpebral fissure; occasionally more than one nodule
- Slit lamp: flat anterior scleral surface (confirms no scleritis)
- IOP very occasionally elevated
- Anterior chamber reaction in ~10%
- After several episodes, inflamed vessels may become permanently dilated
- Must exclude: phlyctenulosis (phlycten is within the conjunctiva, not beneath it) and conjunctival granuloma
Key Examination Steps
- History - rash, arthritis, venereal disease, recent viral illness
- External exam in natural light - look for violaceous hue (suggests scleritis)
- Slit lamp - anesthetize, move conjunctiva with cotton-tipped applicator to assess depth of vessels; check for corneal/AC involvement; measure IOP
- Phenylephrine 2.5% test - instill and re-examine after 10-15 min:
- Episcleral vessels blanch → episcleritis
- Deep scleral vessels do not blanch → scleritis
Episcleritis vs. Scleritis - Key Differences
| Feature | Episcleritis | Scleritis |
|---|---|---|
| Age | Young to middle-aged | Usually older |
| Pain | Mild/absent | Deep, severe, radiates to head/face |
| Systemic disease | Often absent | Frequently associated |
| Vascular layer affected | Superficial episcleral plexus | Deep vascular plexus |
| Colour | Bright red | Violaceous/bluish hue (natural light) |
| Phenylephrine 2.5% | Blanches | Does NOT blanch |
| Corneal involvement | Rare | Can occur (peripheral stromal keratitis) |
| Anterior uveitis | Rare | Can occur |
| Prognosis | Benign, self-limiting | Can threaten vision |
Investigations
For recurrent cases or suspected systemic disease:
-
CBC, CMP
-
ANA, RF, anti-CCP
-
ESR, CRP
-
Serum uric acid (gout)
-
RPR/VDRL + FTA-ABS (syphilis)
-
ANCA (vasculitis)
-
Investigate for herpes zoster, Lyme, etc. as indicated
-
Wills Eye Manual, p. 339
Treatment
Simple Episcleritis
| Severity | Treatment |
|---|---|
| Mild | No treatment needed; cool compresses, refrigerated artificial tears q.i.d. |
| Moderate-severe | Topical NSAID (diclofenac 0.1% q.i.d., bromfenac daily) OR mild topical steroid (fluorometholone 0.1-0.25% q.i.d.) for 1-2 weeks |
| Severe/resistant | More potent topical steroid with rapid tapering |
| Systemic | Oral NSAID - ibuprofen 200-600 mg t.i.d.-q.i.d., naproxen 250-500 mg b.i.d., or indomethacin (take with food/antacids) for at least 10-14 days |
Note: Many physicians prefer oral NSAIDs to topical NSAIDs or steroids as initial therapy. Oral prednisone alone is NOT preferred for episcleritis.
Nodular Episcleritis
Treatment is similar to simple episcleritis.
Prognosis
- Benign and self-limiting
- Recurrences are common but decrease in frequency with time
- Does NOT progress to scleritis in the vast majority
- Vision is not at risk
Sources: Kanski's Clinical Ophthalmology 10th ed. | Wills Eye Manual
headache from davison and Harrison
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Note on Davidson's: Davidson's Principles and Practice of Medicine is not available in this library. The answer below is drawn entirely from Harrison's Principles of Internal Medicine 22E (2025), which covers headache in equivalent (and more extensive) depth across Chapters 17 and 441.
Headache
Harrison's Principles of Internal Medicine 22E - Chapters 17 & 441
Classification (ICHD-III Based)
| PRIMARY HEADACHE | % | SECONDARY HEADACHE | % |
|---|---|---|---|
| Tension-type | 69 | Systemic infection | 63 |
| Migraine | 16 | Head injury | 4 |
| Idiopathic stabbing | 2 | Vascular disorders | 1 |
| Exertional | 1 | Subarachnoid hemorrhage | <1 |
| Cluster | 0.1 | Brain tumor | 0.1 |
- Primary headaches - headache and its features form the disorder itself
- Secondary headaches - caused by an exogenous/underlying disorder
Anatomy and Physiology of Headache
Pain-producing cranial structures include: scalp, meningeal arteries, dural sinuses, falx cerebri, and proximal segments of large pial arteries. The ventricular ependyma, choroid plexus, pial veins, and brain parenchyma are NOT pain-producing.
Key structures in primary headache:
- Large intracranial vessels and dura mater + peripheral terminals of the trigeminal nerve (trigeminovascular system)
- Trigeminocervical complex (TCC) - caudal trigeminal nucleus extending into dorsal horns of C1-C2
- Rostral pain-processing regions: ventroposteromedial thalamus, cortex
- Pain-modulating systems: hypothalamus, dorsal raphe, locus coeruleus, nucleus raphe magnus
The innervation of large intracranial vessels and dura mater by the trigeminal nerve = trigeminovascular system.
Clinical Evaluation of Acute, New-Onset Headache
"Red flag" features requiring urgent workup:
- Sudden onset ("thunderclap") - worst headache of life → SAH until proven otherwise
- Fever + neck stiffness → meningitis
- New headache in patient >50 → temporal arteritis, mass lesion
- Progressive worsening headache
- Headache with exertion, bending, Valsalva → posterior fossa mass, Chiari, low CSF pressure
- Neurologic deficits
- Headache in known malignancy → metastases or carcinomatous meningitis
PRIMARY HEADACHE DISORDERS
1. MIGRAINE
Epidemiology: ~15% of women, 6% of men; most common neurologic cause of disability worldwide. Usually episodic.
Phases of migraine:
| Phase | Features |
|---|---|
| Premonitory | Yawning, food craving, mood change, fatigue (hours-days before) |
| Aura | Focal neurologic symptoms (visual, sensory, speech) - typically 20-30 min; precede headache |
| Headache | Unilateral throbbing pain; nausea/vomiting; photophobia, phonophobia, osmophobia; allodynia; vertigo |
| Postdrome | Tiredness, weariness, concentration impairment |
Aura: Positive and/or negative visual phenomena (fortification spectra, scotoma), sensory symptoms, or speech disturbance lasting 20-30 min. Migraine with brainstem aura replaces "basilar migraine" - features dysarthria, diplopia, tinnitus, vertigo, bilateral sensory symptoms.
Acephalgic migraine (typical aura without headache): Recurrent neurologic symptoms + nausea, without significant headache. Vertigo can be prominent - vestibular migraine accounts for ~1/3 of vertigo referrals.
Pathophysiology:
- Trigeminovascular input from meningeal vessels → trigeminal ganglion → TCC → quintothalamic tract → thalamus
- CGRP (calcitonin gene-related peptide) is the key neuropeptide mediator
- Cortical spreading depression underlies the aura
Treatment of Migraine
Assessment: Use the MIDAS (Migraine Disability Assessment Score) to gauge disease burden.
Non-pharmacologic:
- Identify and avoid triggers
- Regulated lifestyle: regular sleep, diet, exercise
- Avoid excess caffeine, alcohol
- Biofeedback, relaxation, yoga, meditation (adjuncts)
Acute (abortive) treatment:
| Drug Class | Examples | Notes |
|---|---|---|
| NSAIDs | Ibuprofen, aspirin, naproxen | Most effective when taken early; less effective in moderate-severe attacks |
| Aspirin + acetaminophen + caffeine | Excedrin | FDA-approved for mild-moderate migraine |
| Triptans (5-HT1B/1D agonists) | Sumatriptan, rizatriptan, zolmitriptan | Mainstay for moderate-severe; do not repeat dose within 2h (ineffective); use SC/nasal for rapid onset |
| Gepants (CGRP receptor antagonists) | Ubrogepant, rimegepant | Repeat dosing at 2h IS effective; useful when triptans contraindicated |
| Ditans (5-HT1F agonists) | Lasmiditan | No vasoconstrictive effect |
| Dopamine antagonists (antiemetics) | Metoclopramide, prochlorperazine | Also relieve nausea; useful parenterally |
Key principle: Take an adequate dose as soon as possible after onset. If inadequate relief within 60 min, increase dose for next attack or switch class.
Prophylactic treatment (indicated when attacks frequent/disabling):
| Class | Drugs |
|---|---|
| Beta-blockers | Propranolol, metoprolol |
| Antidepressants | Amitriptyline |
| Anticonvulsants | Valproate, topiramate |
| CGRP monoclonal antibodies | Erenumab, fremanezumab, galcanezumab (monthly SC injection) |
| Calcium channel blockers | Verapamil |
| OnabotulinumtoxinA | For chronic migraine (≥15 days/month) |
2. TENSION-TYPE HEADACHE (TTH)
- Most common headache (69% of all headaches)
- Bilateral, pressing/tightening (non-pulsating), mild-moderate intensity
- No nausea/vomiting; no aggravation by routine physical activity
- Featureless headache - migraine is headache WITH features; TTH is headache WITHOUT features
Treatment:
- Acute: acetaminophen, aspirin, NSAIDs
- Behavioral: relaxation therapy
- Triptans NOT effective in pure TTH (effective only if patient also has migraine)
- Chronic TTH: amitriptyline is the only proven preventive treatment
- SSRIs, benzodiazepines - NOT proven effective
- Botulinum toxin A - negative in controlled trials for chronic TTH
3. TRIGEMINAL AUTONOMIC CEPHALALGIAS (TACs)
TACs = cluster headache + paroxysmal hemicrania + SUNCT/SUNA + hemicrania continua. Characterized by short-lasting unilateral pain + ipsilateral cranial autonomic symptoms (lacrimation, conjunctival injection, nasal congestion, rhinorrhea, ptosis, aural fullness). Often misdiagnosed as "sinus headache."
Comparison Table:
| Feature | Cluster Headache | Paroxysmal Hemicrania | SUNCT/SUNA |
|---|---|---|---|
| Gender | M >> F (3:1) | F = M | F ~ M |
| Pain type | Stabbing, boring | Throbbing, boring, stabbing | Burning, stabbing, sharp |
| Severity | Excruciating | Excruciating | Severe to excruciating |
| Site | Orbit, temple | Orbit, temple | Periorbital |
| Duration | 15-180 min | 2-30 min | 5-240 seconds |
| Attack frequency | 1/alternate day - 8/day | 1-20/day | 3-200/day |
| Alcohol trigger | Yes | No | No |
| Indomethacin response | - | Yes (pathognomonic) | - |
| Acute Rx | Sumatriptan SC/nasal; O₂ | No effective treatment | Lidocaine IV |
| Prevention | Verapamil, prednisone | Indomethacin | Lamotrigine |
Cluster Headache - Key Features
- Population frequency ~0.1%; men affected 3x more than women
- Deep, retroorbital, excruciating, nonfluctuating, explosive pain
- Periodicity - attacks recur at the same hour daily for a cluster bout (8-10 weeks/year)
- Pain-free interval averages ~1 year
- Nocturnal onset in ~50%
- Patients pace and rock during attacks (contrast: migraine patients lie still)
- Ipsilateral autonomic features: conjunctival injection, lacrimation, rhinorrhea, ptosis
- Involves central pacemaker neurons in posterior hypothalamic region
Acute treatment:
- 100% O₂ at 10-12 L/min for 15-20 min (very effective)
- Sumatriptan 6 mg SC - shortens attack to 10-15 min; no tachyphylaxis
- Sumatriptan 20 mg nasal spray or zolmitriptan 5 mg nasal spray
- Non-invasive vagus nerve stimulation (nVNS) - FDA cleared for episodic cluster headache
- Oral sumatriptan NOT effective for cluster headache
Preventive treatment:
| Short-term | Long-term |
|---|---|
| Prednisone 1 mg/kg (up to 60 mg), taper over 21 days | Verapamil 160-960 mg/day |
| Verapamil 160-960 mg/day | Lithium |
| Topiramate | |
| Melatonin 9-12 mg at night |
4. OTHER PRIMARY HEADACHE DISORDERS
| Type | Features |
|---|---|
| Primary cough headache | Sudden onset with Valsalva (cough, sneeze, strain); bilateral; benign or Chiari-related |
| Primary exercise headache | Pulsating, bilateral, with strenuous exercise |
| Primary sex headache | Dull bilateral neck/head pain building to orgasm; or explosive at orgasm ("thunderclap") |
| Primary stabbing headache | Transient stabs (ice-pick pains); periorbital; treat with indomethacin |
| Hypnic headache | Wakes from sleep; >50 years; diffuse; no autonomic features; treat with caffeine, lithium |
| Medication-overuse headache | Headache >15 days/month with regular use of acute headache Rx >10 days/month |
SECONDARY HEADACHE - Important Causes
Meningitis
- Acute severe headache + stiff neck + fever → LP mandatory
- Pain accentuated by eye movement; can mimic migraine (photophobia, nausea, vomiting)
Intracranial Hemorrhage (SAH)
- Sudden onset, maximal in <5 min, severe, lasting >5 min + stiff neck without fever → SAH until proven otherwise
- CT head; if CT negative → LP required (small or infraforamen magnum bleeds can be CT-negative)
Brain Tumor
- ~30% of brain tumor patients report headache as chief complaint
- Usually intermittent, deep, dull, moderate intensity; worsens with exertion/position change
- Vomiting preceding headache by weeks = highly characteristic of posterior fossa tumor
- Headache disturbs sleep in ~10%
- Brain tumor is a rare cause of headache; migraine far more common
Temporal (Giant Cell) Arteritis
- Annual incidence 77/100,000 in age ≥50; average onset age 70; women 65%
- Dull, boring head pain - unilateral or bilateral; temporal in 50%
- Jaw claudication, scalp tenderness, fever, weight loss, polymyalgia rheumatica
- ESR usually elevated (but normal ESR does NOT exclude it)
- 50% risk of blindness if untreated - ischemic optic neuropathy is the major cause of rapid bilateral blindness in >60 years
- Treat promptly with prednisone 80 mg/day for 4-6 weeks; temporal artery biopsy
Glaucoma (Acute Angle Closure)
- Prostrating headache + nausea/vomiting + severe eye pain
- Red eye, fixed, moderately dilated pupil
Chronic Daily Headache (CDH)
- Headache on ≥15 days/month
- Not a single diagnosis - encompasses chronic migraine, chronic TTH, medication-overuse headache, new daily persistent headache
- Medication-overuse headache: regular use of any acute headache medication on >10 days/month leads to chronic daily headache
Source: Harrison's Principles of Internal Medicine 22E (2025) - Chapters 17 (Headache as a Cardinal Symptom) and 441 (Migraine and Other Primary Headache Disorders)
This is a shared conversation. Sign in to Orris to start your own chat.