Raised monocyte cause
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Here is the full answer:
Monocytosis - Causes
Definition: Monocytosis is an absolute monocyte count above 1.0 x 10⁹/L (some sources use >500/µL as the lower threshold). It is frequently a reactive finding, but persistent unexplained monocytosis should raise suspicion for a hematologic neoplasm.
1. Infections (most classic reactive cause)
- Tuberculosis (classic and most commonly cited)
- Subacute bacterial endocarditis (monocytes may show phagocytosis of RBCs and other leukocytes)
- Syphilis
- Granulomatous/fungal infections
- Rickettsial infections
- Protozoal infections
- Viral infections (various)
Paradoxically, while infections are the most classically taught cause, in practice hematologic malignancies account for the majority of cases (>50% in one classic series of 160 patients).
2. Inflammatory / Autoimmune Diseases
- Systemic lupus erythematosus (SLE)
- Rheumatoid arthritis
- Giant cell arteritis / temporal arteritis
- Vasculitis and polyarteritis nodosa
- Inflammatory bowel disease (chronic ulcerative colitis, Crohn's)
- Sarcoidosis
- Myositis
- Celiac disease (sprue)
3. Hematologic Malignancies (most common cause overall)
- Chronic myelomonocytic leukemia (CMML) - defined by persistent monocytosis >1.0 x 10⁹/L (monocytes ≥10% of leukocytes) for >3 months once reactive causes excluded
- Acute myelomonocytic leukemia (AML-M4) and acute monocytic leukemia (AML-M5)
- Lymphoma (Hodgkin lymphoma most frequently, also non-Hodgkin)
- Multiple myeloma
- Myeloproliferative disorders
4. Recovery States
- Recovery from neutropenia / agranulocytosis (considered a favorable sign)
- Recovery from bone marrow suppression (chemotherapy, etc.)
5. Other / Miscellaneous
- Post-splenectomy
- Solid tumors (various carcinomas)
- Immune thrombocytopenic purpura (ITP)
- Chronic neutropenia (compensatory response)
- Histiocytosis
Key Clinical Pearls
| Feature | Significance |
|---|---|
| Monocytosis + promonocytes on smear | Suggests neoplasm (CMML) |
| Monocytosis + splenomegaly | Neoplastic cause likely |
| Monocytosis during febrile illness | Usually reactive/transient |
| Serum lysozyme elevated | Monocytic proliferation, but does NOT distinguish reactive from neoplastic |
| Automated counters | May misclassify hairy cells, blasts, abnormal T cells as monocytes |
Approach to Persistent Monocytosis
- Rule out infections (TB, SBE, syphilis, fungi)
- Rule out inflammatory/autoimmune disease (ANA, RF, ESR/CRP)
- If unexplained and persists >3 months → evaluate for CMML (bone marrow biopsy, flow cytometry, cytogenetics)
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods; Goldman-Cecil Medicine; Quick Compendium of Clinical Pathology 5th ed.
Pt having fever with cough
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have excellent source material from Harrison's and Goldman-Cecil. Here is a comprehensive differential for an adult with fever and cough:
Differential Diagnosis: Adult with Fever + Cough
The combination of fever and cough in an adult points primarily to respiratory tract infections, but the differential is broad. Narrowing it requires attention to acuity, cough character, associated symptoms, exposure history, and risk factors.
MOST COMMON - Respiratory Tract Infections
1. Community-Acquired Pneumonia (CAP) - Rule out first
Fever, productive cough (mucoid/purulent/blood-tinged sputum), dyspnea, tachycardia, pleuritic chest pain. Physical exam: crackles, bronchial breathing, dullness on percussion. Requires CXR to confirm new infiltrate.
- Key pathogens: Streptococcus pneumoniae (most common), Haemophilus influenzae, Moraxella catarrhalis, atypicals (Mycoplasma, Chlamydophila, Legionella), S. aureus (including CA-MRSA - can cause necrotizing pneumonia with hemoptysis)
2. Acute Bronchitis
Fever (often low-grade), productive cough lasting days-weeks, no CXR consolidation. Most cases are viral. Predominantly self-limited - antibiotics usually NOT indicated.
3. Influenza
Abrupt onset, high fever, dry cough, myalgia, headache, fatigue ("flu" syndrome). Seasonal (Nov-March). Specific rapid antigen tests available.
4. COVID-19 (SARS-CoV-2)
Fever, cough, shortness of breath, fatigue, myalgia, headache. Loss of taste/smell is relatively specific. Can progress to severe pneumonia/ARDS.
5. Upper Respiratory Tract Infection (Common Cold/Viral URI)
Mild fever, dry or minimally productive cough, rhinorrhea, sore throat. Usually rhinovirus, coronavirus, RSV, adenovirus. Self-limiting in 7-10 days.
6. Acute Exacerbation of Chronic Bronchitis / COPD
Worsening productive cough, dyspnea, change in sputum color/volume. Pathogens: H. influenzae, M. catarrhalis, S. pneumoniae.
LESS COMMON BUT IMPORTANT
7. Tuberculosis (TB)
Chronic cough (>2-3 weeks), low-grade fever, night sweats, weight loss, hemoptysis. Upper-lobe cavitating lesion on CXR. Consider in immigrants, HIV+, incarcerated, homeless, healthcare workers, close contacts.
8. Atypical Pneumonia ("Walking Pneumonia")
Insidious onset, mild-to-moderate fever, non-productive or minimally productive cough, prominent headache/malaise out of proportion to CXR findings. Mycoplasma pneumoniae (young adults), Chlamydophila pneumoniae, Legionella pneumophila (Pontiac fever/Legionnaires' - associated with contaminated water sources, air conditioning, severe disease).
9. Lung Abscess
High fever, purulent/foul-smelling sputum, often in patients with aspiration risk (poor dentition, alcohol, seizures, unconsciousness). CXR shows cavitation with air-fluid level.
10. Fungal Pneumonias
- Histoplasma capsulatum - fever, cough, mediastinal lymphadenopathy; exposure to bird/bat droppings in endemic areas (Ohio/Mississippi River valleys)
- Coccidioides immitis - fever, cough, rash (erythema nodosum); exposure in southwestern US/desert regions
- Aspergillus - primarily in immunocompromised
11. Viral Pneumonitis
RSV, parainfluenza, adenovirus, hantavirus (rare, rodent exposure), CMV (in immunocompromised).
SERIOUS / MUST NOT MISS
| Condition | Key Clue |
|---|---|
| Pulmonary embolism | Pleuritic chest pain, hemoptysis, tachycardia, DVT risk factors; fever is possible |
| Acute heart failure | Orthopnea, PND, bilateral crackles, S3 gallop, BNP elevated |
| Lung malignancy with post-obstructive pneumonia | Recurrent pneumonia in same segment, smoker, constitutional symptoms |
| Sepsis | Tachycardia, hypotension, altered mental status, high WBC - respiratory source |
RARER / SPECIAL CONTEXTS
- Pertussis (Bordetella pertussis) - prolonged cough with paroxysms/"whoop," post-tussive vomiting, lymphocytosis; adults often only cough without classic whoop
- Q fever (Coxiella burnetii) - animal exposure (farm, livestock), atypical pneumonia pattern
- Psittacosis (Chlamydophila psittaci) - bird exposure
- Rickettsial infections - tick exposure, rash
- SARS/MERS - travel history, contact with confirmed cases
- Sarcoidosis - bilateral hilar adenopathy, non-caseating granulomas (non-infectious but can mimic)
Clues That Help Narrow the Diagnosis
| Feature | Points Toward |
|---|---|
| Abrupt onset, high fever, myalgia | Influenza |
| Gradual onset, dry cough, "feel too well to be this sick" | Atypical pneumonia (Mycoplasma) |
| Productive purulent cough, lobar consolidation | Bacterial CAP |
| Loss of taste/smell | COVID-19 |
| Night sweats + weight loss + chronic cough | TB or malignancy |
| Cough >3 weeks | TB, malignancy, bronchiectasis |
| Pleuritic pain + hemoptysis | PE, cavitating pneumonia, TB |
| Recent hospital/healthcare exposure | HAP, MRSA, resistant pathogens |
| Immunocompromised | Atypical + opportunistic infections (PCP, CMV, Aspergillus) |
| Water exposure (hotel, hot tub, cooling towers) | Legionella |
Initial Investigations to Consider
- CXR - mandatory first step to identify consolidation, effusion, cavitation, hilar adenopathy
- CBC - neutrophilia (bacterial), lymphocytosis (viral/TB), leucopenia (viral/atypical)
- CRP / Procalcitonin - helps distinguish bacterial from viral (PCT more specific)
- Sputum Gram stain + culture (productive cough)
- Rapid flu/COVID antigen or PCR
- Blood cultures (if hospitalizing)
- Urine Legionella antigen (severe/atypical CAP)
- Sputum AFB if TB suspected (3 morning samples)
Sources: Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Henry's Clinical Diagnosis and Management by Laboratory Methods
How to do mannuever exersice for vertigo
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I have all the information needed. Here is the complete guide:
Maneuvers & Exercises for Vertigo (BPPV)
Most positional vertigo is Benign Paroxysmal Positional Vertigo (BPPV) - caused by loose calcium carbonate crystals (otoconia/canalith) displaced into the semicircular canals, most commonly the posterior canal. The goal of all maneuvers is to reposition these particles back into the utricle where they cause no symptoms.
Step 0 - First Diagnose the Affected Side (Dix-Hallpike Test)
Before any maneuver, identify which ear is affected:
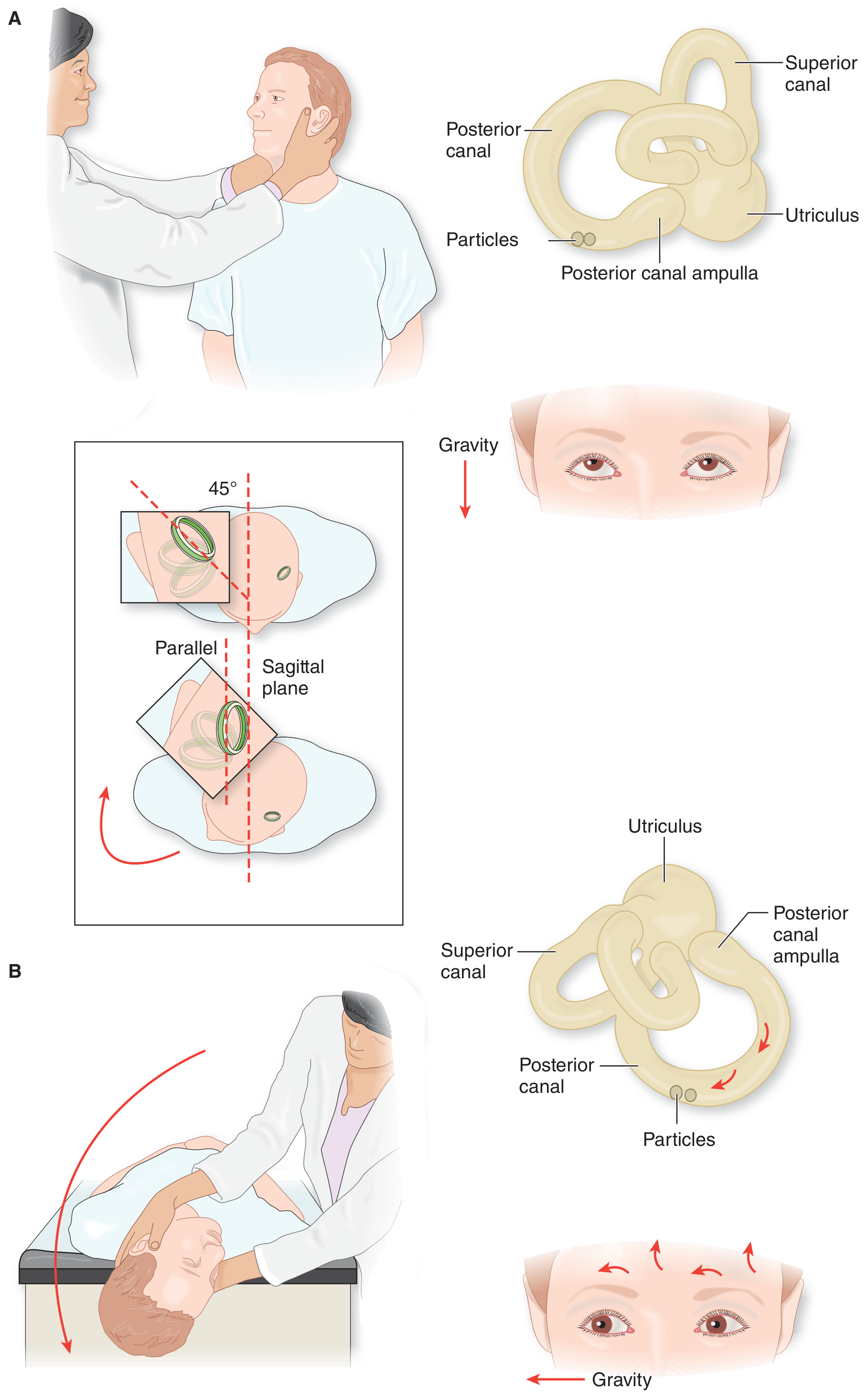
- Patient sits on the exam table, head turned 45° toward the suspected ear
- Rapidly lay the patient back so the head hangs slightly below the table edge
- Positive test: Rotatory/upbeat nystagmus + vertigo within seconds - the ear that is DOWN is the affected side
- Wait for nystagmus to stop, then sit the patient up - nystagmus should reverse direction briefly
- If negative, repeat with the head turned to the other side
1. Epley Canalith Repositioning Maneuver (CRM) - First-Line Treatment
Indication: BPPV due to posterior canal canalolithiasis (most common type)
Success rate: ~80% with a single session
Assume the right ear is affected (mirror for left):
| Step | Position | Hold Time |
|---|---|---|
| 1 | Sit upright, turn head 45° to the right (affected side) | Ready position |
| 2 | Quickly lie back with head hanging (Dix-Hallpike position) - right ear down, head extended slightly, chin up | 20-30 sec (wait for nystagmus to stop) |
| 3 | Turn head 45-60° toward the left (opposite ear), still lying flat | 20 sec |
| 4 | Roll the entire body onto the left side, turning the head an additional 45° so it faces almost downward (nose toward floor) | 20 sec |
| 5 | Slowly return to the upright seated position | Done |
Key points:
- Each position is held for ~20 seconds or until vertigo and nystagmus stop
- The final face-down step (Step 4) is critical and often omitted - do not skip it
- A second sequence immediately after the first can help a few more patients
- ~80% respond to one treatment; additional maneuvers in the same session add no benefit
- Mastoid vibration can be added in resistant cases to help mobilize crystals
- Post-procedure sleep restriction (upright for 24 hrs) is no longer recommended by recent evidence
2. Semont (Liberatory) Maneuver
Indication: BPPV due to cupulolithiasis (particles attached to the cupula rather than free-floating), or as an alternative to Epley
Again assuming left ear affected (as shown in source diagrams):
| Step | Action | Hold |
|---|---|---|
| 1 | Sit on edge of bed/table, turn head 45° to the right (unaffected side) | Sitting |
| 2 | Rapidly drop sideways to the left (affected side), head turns so face points upward at 45° | 30+ sec or until vertigo stops |
| 3 | In one brisk swing, move to the opposite side (right side lying), head now faces downward at 45° | 30 sec |
| 4 | Slowly return to seated upright position | Done |
Key: The swing in Step 3 must be rapid and decisive - this is what dislodges the debris from the cupula.
3. Brandt-Daroff Exercises
Indication:
- Persistent BPPV not resolved by CRM or Semont maneuver
- Residual dizziness without nystagmus
- Patient who cannot tolerate the Epley maneuver
- Home self-treatment option
How to do it:
- Start: Sit upright on the side of the bed
- Step 1: Quickly lie down on one side with the head angled upward (nose up ~45°) - stay for 30 seconds or until vertigo subsides
- Return: Sit back up for 30 seconds
- Step 2: Quickly lie down on the other side with head angled upward (nose up ~45°) - stay 30 seconds
- Return: Sit up
Frequency: Repeat the whole cycle 5 times, 3 times per day
Duration: Most patients improve within 3-14 days
Note: Brandt-Daroff exercises work by habituation - they intentionally provoke dozens of vertigo episodes to desensitize the vestibular system. They are less effective than CRM (23% resolution in 1 week vs ~80% for Epley), so they are a second-line/adjunct option.
Which Maneuver to Choose?
| Situation | Best Maneuver |
|---|---|
| Posterior canal BPPV (most common) | Epley CRM first-line |
| Cupulolithiasis | Semont (Liberatory) maneuver |
| Persistent BPPV after CRM failure | Brandt-Daroff exercises |
| Patient cannot tolerate clinic maneuvers | Brandt-Daroff at home |
| Lateral canal BPPV | Barbecue roll (Lempert) maneuver (roll 360° in 4 steps) |
Important Cautions
- Always rule out central causes of vertigo first (stroke, cerebellar lesion) before attributing symptoms to BPPV. Red flags: direction-changing nystagmus, vertical nystagmus without torsion, neurological signs, severe headache.
- An incompletely performed Epley maneuver can convert posterior canal BPPV to the harder-to-treat lateral canal variant.
- If patient has neck or back problems, modify as needed or refer to specialist.
Sources: Adams and Victor's Principles of Neurology 12th Ed; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Shambaugh Surgery of the Ear
This is a shared conversation. Sign in to Orris to start your own chat.