Failure to thrive in pediatrics long case
Reading File
Finding Sources
Finding Sources
Searching PubMed
"failure to thrive" pediatric evaluation management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full long-case answer.
Failure to Thrive (FTT) in Pediatrics - Long Case
Definition
Failure to thrive is not a diagnosis but a sign - it describes inadequate physical growth in a child, most commonly defined as:
- Weight consistently below the 3rd (or 5th) percentile for age and sex on standard growth charts, OR
- Weight crossing two major percentile lines downward over time, OR
- Weight for height below the 5th percentile (wasting)
The term "pediatric undernutrition" or "growth faltering" is increasingly preferred in the literature. FTT occurs most commonly in children under 2 years of age, with weight being the first parameter affected, followed by height, then head circumference.
Classification
FTT is broadly divided into three categories (though most cases are mixed):
| Type | Description | Fraction of cases |
|---|---|---|
| Nonorganic (Psychosocial) | No underlying disease; due to inadequate intake from psychosocial/environmental causes | ~70-80% |
| Organic | Underlying medical disease causing inadequate intake, absorption, or utilization | ~20-30% |
| Mixed | Both organic disease AND psychosocial factors coexist | Common |
Causes
Nonorganic / Psychosocial
- Maternal deprivation, parental neglect, or ignorance of infant feeding needs
- Poverty and food insecurity
- Errors in formula preparation (over-dilution)
- Inappropriate feeding practices (early solids, improper positioning)
- Disturbed caregiver-infant relationship (maternal depression, postnatal depression)
- Psychosocial dwarfism - in older children: growth retardation with bizarre eating behaviors (e.g., eating from garbage cans, binge-purge), accompanied by reversible GH deficiency that normalizes when the child is removed from the dysfunctional environment
Organic Causes - Classified by Mechanism
1. Inadequate Caloric Intake
- Oral-motor dysfunction, cleft palate, tracheoesophageal fistula
- GERD, pyloric stenosis
- Congenital heart disease (fatigue during feeding)
- Central nervous system abnormalities
- Laryngomalacia (dyspnea on feeding)
2. Inadequate Absorption / Malabsorption
- Cystic fibrosis (most common cause of FTT with malabsorption)
- Celiac disease
- Cow's milk protein intolerance
- Short bowel syndrome
- Biliary atresia, neonatal hepatitis
- Inflammatory bowel disease
3. Increased Metabolic Demand
- Congenital heart disease (left-to-right shunts, cyanotic heart disease)
- Chronic lung disease, bronchopulmonary dysplasia
- Chronic infections (HIV, TB, recurrent bacterial infections)
- Malignancy
- Inborn errors of metabolism
4. Impaired Utilization
- Chromosomal disorders (Down syndrome, Turner syndrome)
- Hypothyroidism
- Renal tubular acidosis, chronic kidney disease
- Diabetes insipidus
- Severe combined immunodeficiency (SCID)
- Inborn errors of metabolism (glycogen storage diseases, organic acidemias)
Clinical Approach - History
Presenting Complaints
- Poor weight gain / not gaining weight appropriately
- Feeding difficulties - slow feeding, vomiting, choking, refusal
- Recurrent infections, chronic diarrhea, loose stools
- Delayed milestones
Dietary History (KEY)
- Detailed feeding record - breastfed vs. formula, frequency, duration, volume
- If formula: preparation technique (is it being diluted?)
- Introduction of solids: timing, types, amounts
- 3-day food diary is extremely helpful
- Any food aversions, textures refused
- Who feeds the child and how?
Birth History
- Birth weight and gestational age
- Intrauterine growth restriction (IUGR)
- Perinatal complications, anoxia
Past Medical History
- Recurrent hospitalizations, infections
- Chronic illnesses, medications
- Developmental milestones (motor, speech, social)
Family/Social History
- Parental heights - mid-parental height calculation
- Parental education, employment, socioeconomic status
- Mental health of caregivers (maternal depression)
- Substance abuse in household
- Family history of CF, celiac, metabolic disorders, short stature
Developmental History
- Global developmental delay may indicate a syndrome or CNS cause
- Milestones appropriate vs. delayed
Clinical Approach - Physical Examination
Anthropometry (MANDATORY and most important)
- Weight (most sensitive early indicator, affected first)
- Height/Length (affected later - chronic malnutrition)
- Head circumference (last to be affected; if decreased = chronic severe malnutrition or CNS pathology)
- Plot all parameters on appropriate age/sex growth charts
- For premature infants: use corrected gestational age on special preterm growth charts
Pattern Recognition
| Growth parameter affected | Implies |
|---|---|
| Weight only | Acute malnutrition / early FTT |
| Weight + Height | Chronic malnutrition |
| Weight + Height + Head circumference | Severe chronic malnutrition or intrinsic CNS/chromosomal cause |
Signs of Malnutrition
- Wasting: loss of subcutaneous fat over buttocks, inner thighs, suprascapular region (examine these areas!)
- Prominent ribs, narrow face, thin limbs
- Edema (in severe protein deficiency - kwashiorkor)
- Dermatitis: peeling skin, diaper rash, hyperpigmentation/depigmentation in protein-calorie malnutrition
- Hair changes: sparse, depigmented, easily plucked hair
- Muscle wasting - assess biceps and quadriceps
Micronutrient Deficiency Signs
- Vitamin D deficiency: rachitic rosary, widened wrists/ankles, craniotabes, genu varum/valgum, frontal bossing
- Vitamin C deficiency: perifollicular hemorrhage, bleeding gums
- Iron deficiency: pallor, koilonychia
- Zinc deficiency: perioral/perianal dermatitis, vesicobullous lesions
- Vitamin A deficiency: Bitot spots, xerophthalmia
Dysmorphic Features
- Suggest chromosomal cause (Down, Turner, Williams syndrome)
Organomegaly
- Hepatomegaly - liver disease, metabolic storage disorders, heart failure
- Lymphadenopathy - HIV, TB, malignancy
Cardiorespiratory
- Heart murmur - congenital heart disease
- Crepitations - chronic lung disease, CF
Neglect Indicators
- Poor hygiene, dirty clothing, uncut nails, diaper rash
- Flat affect, listlessness, poor eye contact, developmental regression
- Observe parent-child interaction carefully
Investigations
Principle: Routine "shotgun" investigations are low yield and generally not recommended. Workup must be guided by history and physical examination. Most cases (especially nonorganic) are diagnosed clinically.
Initial / First-Line (if organic FTT suspected or workup warranted)
| Test | Reason |
|---|---|
| Full blood count | Anemia (iron deficiency, infection, malignancy) |
| Complete metabolic panel (electrolytes, BUN, creatinine, LFTs) | Renal disease, liver disease, electrolyte imbalances |
| Urinalysis + urine culture | Renal tubular acidosis, UTI |
| ESR/CRP | Inflammatory condition |
| Bone age (X-ray wrist) | Differentiates constitutional delay from pathological short stature |
| Thyroid function tests (T4, TSH) | Hypothyroidism |
| Serum lead level | Environmental toxin exposure |
Second-Line (based on clinical suspicion)
| Test | Indication |
|---|---|
| Sweat chloride test | Cystic fibrosis (chronic respiratory symptoms, steatorrhoea) |
| Anti-tTG IgA antibody + total IgA | Celiac disease (chronic diarrhea, bloating) |
| HIV test | Risk factors, recurrent opportunistic infections |
| Echocardiogram | Heart murmur / cyanosis |
| Stool studies (fat, occult blood, ova & parasites) | Malabsorption, diarrhea |
| Chromosomal karyotype | Dysmorphic features, Turner syndrome |
| Serum amino acids, urine organic acids | Inborn error of metabolism |
| Immunoglobulins, complement, lymphocyte subsets | Recurrent infections - immunodeficiency |
| Hepatitis B/C serology | Liver disease workup |
| Skeletal survey | Suspected physical abuse |
Harriet Lane Handbook: "Routine labs and imaging are often low yield and generally not recommended; workup should be guided by clinical suspicion." - The Harriet Lane Handbook, 23rd Edition
Diagnostic Flowchart
The following algorithm guides the approach to a child below the 5th percentile:
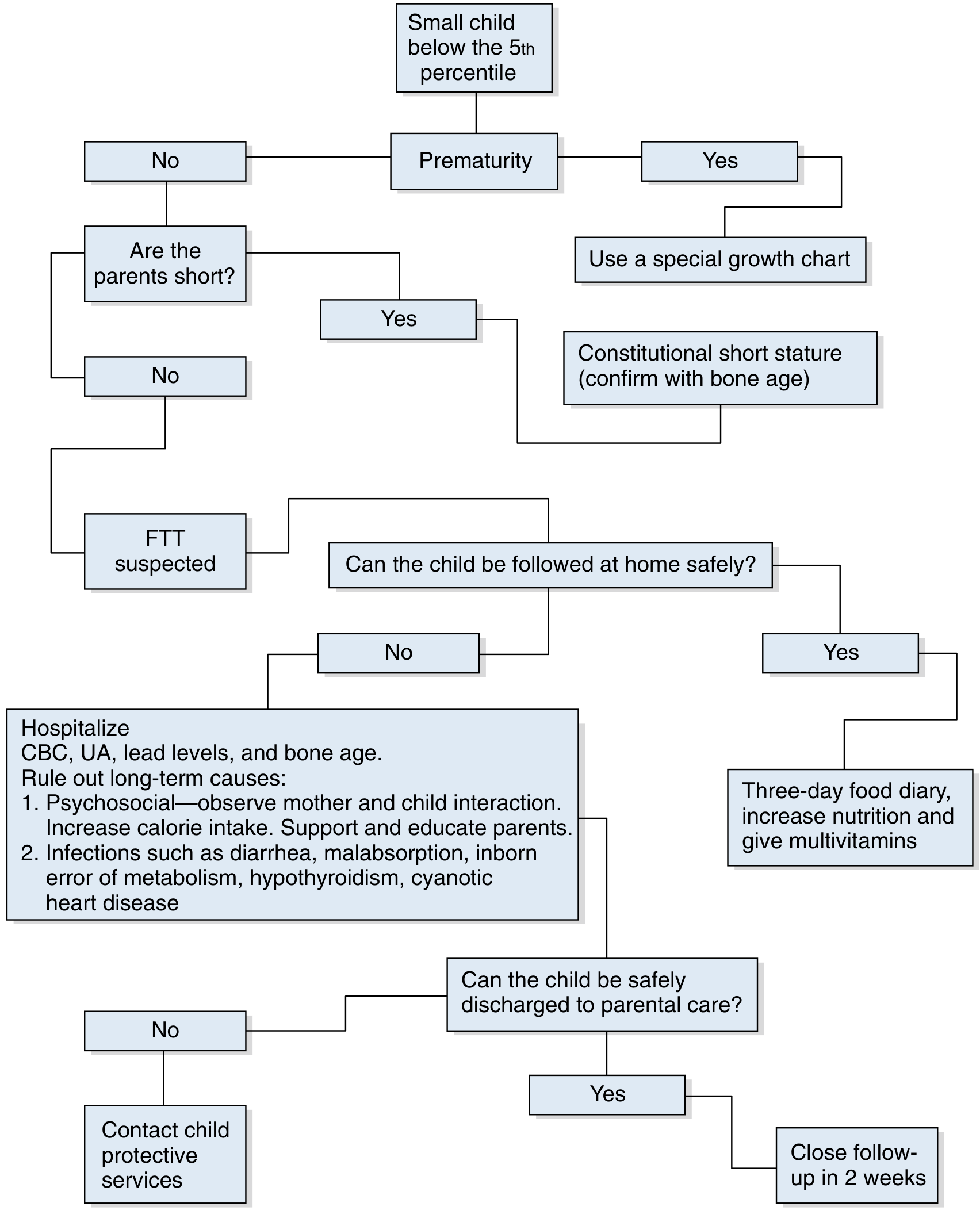
Adapted from Swanson's Family Medicine Review
Management
Inpatient vs. Outpatient
Indications for Hospitalization:
- Severe malnutrition or risk of re-feeding syndrome
- Suspected abuse or neglect where home safety is uncertain
- Social situation prevents safe outpatient follow-up
- Failed outpatient management
- Severe psychological caregiver impairment
- Acute fluid and electrolyte imbalance
- If nonorganic: allows direct observation of mother-child interaction and feeding
Outpatient Management:
- 3-day food diary, calculate actual vs. required caloric intake
- Increase caloric density
- Multivitamin supplementation
- Weekly weight checks initially
Nutritional Rehabilitation
Catch-Up Growth Caloric Requirements (Harriet Lane formula):
RDA calories for age × (Ideal body weight for height / Actual body weight)
Example: 12-month-old boy, weight 7 kg, length 72 cm:
- RDA for age = 98 kcal/kg/day
- Ideal weight for height (50th percentile) = 9 kg
- Catch-up requirement = 98 × (9/7) = 126 kcal/kg/day
Nutritional Strategies
- Breastfed infants: optimize positioning, latch, frequency; consider supplemental nursing system
- Formula-fed infants: ensure correct preparation; consider calorie-dense formula (24-27 kcal/oz)
- Older children: calorie-dense foods (nut butters, avocado, cheese, fortified cereals); limit juice and low-calorie drinks
- Micronutrient supplementation: iron, zinc, vitamin D as indicated
- Appetite stimulants (cyproheptadine, megestrol): considered in children with significant underlying disease (CF, cancer) - not routine
Re-feeding Syndrome (Critical Complication)
Watch for in severe malnutrition when refeeding is initiated:
- Electrolyte shifts (especially hypophosphatemia, hypokalemia, hypomagnesemia)
- Cardiac arrhythmias, respiratory failure, seizures
- Management: daily cardiorespiratory monitoring, strict I/O and calorie count, daily electrolytes (especially phosphate), correct deficiencies before and during refeeding
Treating Underlying Cause
- Address specific organic cause (CF enzyme replacement, celiac - gluten-free diet, hypothyroidism - levothyroxine, CHD - surgical correction)
Psychosocial Intervention (Nonorganic FTT)
- Non-judgmental parent education about feeding practices
- Observe and address dysfunctional parent-child feeding interaction
- Social work referral for poverty, food insecurity
- Mental health referral for maternal depression
- If child abuse or neglect suspected: mandatory reporting to child protective services
- Home visits by public health nurse are highly effective
Follow-Up
- Weekly weight checks initially after discharge
- Some home visits should occur in the child's home environment (especially for nonorganic FTT)
- Target "catch-up growth" over 3-6 months
Prognosis
- Most infants identified early and treated do not progress to severe malnutrition, growth delay, or long-term developmental problems
- Later onset feeding disorders have worse outcomes
- Nonorganic FTT: prognosis depends heavily on the degree of family dysfunction and response to intervention
- Children with untreated severe FTT may suffer cognitive impairment and long-term psychosocial difficulties
- Psychosocial dwarfism: endocrine abnormalities and growth often normalize once the child is removed from the dysfunctional environment
Key Exam Points (Long Case Summary)
| Feature | Key Point |
|---|---|
| Most common type | Nonorganic (~75%) |
| Most common cause | Inadequate caloric intake / psychosocial deprivation |
| First growth parameter affected | Weight (then height, then head circumference) |
| Most important investigation | 3-day dietary record |
| Most common organic cause | GI/malabsorption (CF, celiac, GERD) |
| Catch-up growth formula | RDA × (ideal weight / actual weight) |
| Mandatory action if neglect suspected | Report to child protective services |
| Best follow-up setting (nonorganic) | In the home by public health nurse |
| Complication of rapid refeeding | Refeeding syndrome (hypophosphatemia) |
| Psychosocial dwarfism | Reversible GH deficiency; normalizes on removal from dysfunctional environment |
Sources: Swanson's Family Medicine Review; The Harriet Lane Handbook, 23rd Edition; Tintinalli's Emergency Medicine; Kaplan & Sadock's Synopsis of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.