Mechanical ventilation and modes of ventilation reference cash And cardiopulmonary
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from both textbooks. Let me compile the full detailed response.
Mechanical Ventilation and Modes of Ventilation
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine (CASH), 7th Ed. | Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set
1. Introduction
Mechanical ventilation (MV) is a key resuscitation tool for critically ill patients. The traditional "one-size-fits-all" prescription for MV has been replaced by evidence-based, pulmonary-protective strategies. Increasing hospital overcrowding means emergency and ICU physicians must be fluent in ventilator management, troubleshooting, and liberation strategies.
- Roberts and Hedges' Clinical Procedures in Emergency (CASH), p. 222
2. Basic Physiology
Minute Volume and Alveolar Ventilation
- Minute volume (V̇E) = Tidal Volume (VT) × Respiratory Rate (f)
- Normal V̇E = 7-10 L/min
- VT = Alveolar Volume (VA) + Dead Space Volume (VDS)
- Anatomic dead space ≈ 2.2 mL/kg lean body weight (trachea and large airways)
- Pathologic dead space = ventilated but underperfused alveoli (added in disease states)
- Physiologic dead space = anatomic + pathologic dead space
- Alveolar minute ventilation: V̇A = (VT - VDS) × f
- PaCO2 is determined by V̇A and CO2 production rate
Volume-Pressure Relationship
Compliance (C) describes the relationship between volume and pressure: a stiffer system (decreased compliance) requires more pressure to deliver the same volume. The respiratory system includes ventilator tubing, ETT, trachea, airways, lung parenchyma, chest wall, and diaphragm.
Key Ventilator Parameters
| Parameter | Description |
|---|---|
| FiO2 | Fraction of inspired oxygen (0.21-1.0) |
| Tidal Volume (VT) | Volume delivered per breath (target: 6-8 mL/kg IBW) |
| Respiratory Rate (RR) | Machine-set breath rate |
| PEEP | Positive end-expiratory pressure - prevents alveolar collapse |
| Peak Airway Pressure | Pressure at end of inspiration; reflects resistance + compliance |
| Plateau Pressure | Pressure at zero flow; reflects lung/chest wall compliance (should be ≤30 cm H2O) |
| I:E Ratio | Inspiration:Expiration ratio (normally 1:2 to 1:3) |
| Flow Rate / Waveform | Square (constant) or decelerating waveform |
PEEP Optimization
Optimal PEEP is identified by the plateau pressure method:
- As PEEP increases, plateau pressure initially rises proportionally
- At optimal PEEP, plateau pressure plateaus (no further rise) - lung is optimally recruited
- Beyond optimal PEEP, overdistension causes plateau pressure to rise again
Dynamic Pressure-Volume (PV) Loop - normal open lung:
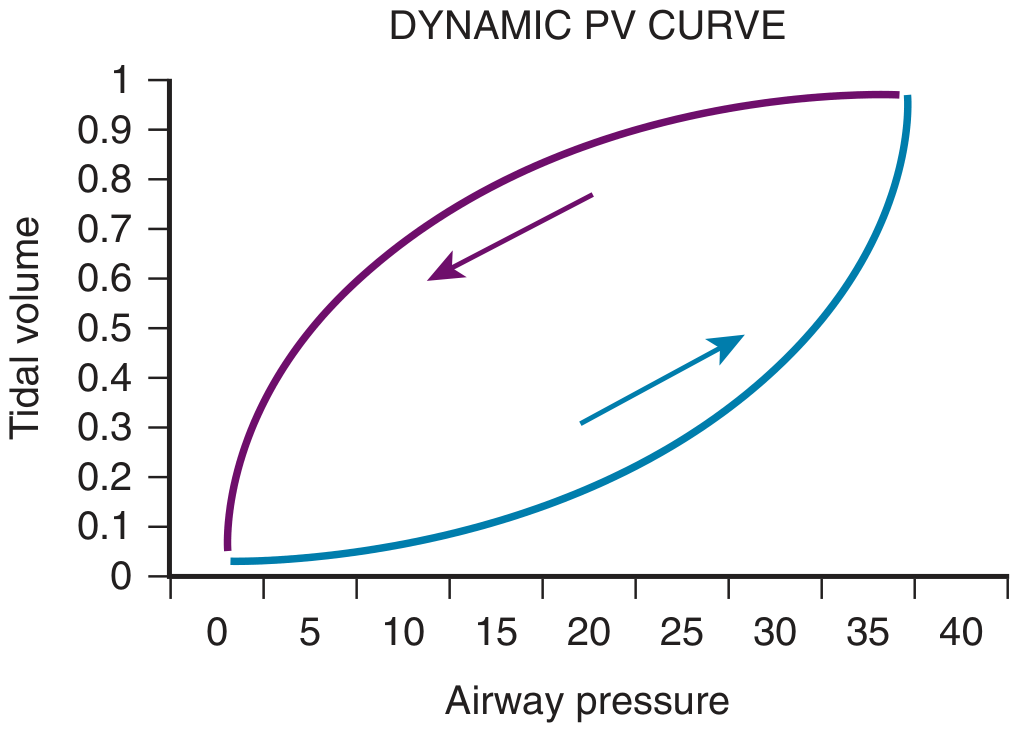
A normal PV loop (adequate PEEP): pressure rise is immediately matched by tidal volume increase. The lower limb rises steeply from the origin - airways are already open.
3. Modes of Ventilation
Ventilators target one of three strategies: spontaneous breathing support, volume-targeted, or pressure-targeted ventilation (or dual/combined modes).
A. Pressure Support Ventilation (PSV)
"PSV is the most widely used mode of mechanical ventilation." - Murray & Nadel, p. 3175
- All breaths are patient-triggered
- Ventilator delivers flow to meet a set inspiratory pressure
- Cycles off when inspiratory flow falls to a threshold (operator-set, typically 10-35% of peak inspiratory flow)
- VT is determined by pressure support level, patient effort, and respiratory system compliance
- FiO2 and PEEP set by clinician; patient controls respiratory rate and flow
- No set RR (most modern ventilators have a backup apnea rate)
- Best for: spontaneous breathing patients being weaned; good patient-ventilator synchrony
- Cycling adjustments: if the ventilator cycles prematurely (under-assistance) or late (delayed cycling/over-assistance), the flow threshold can be adjusted
B. Volume-Cycled Ventilation (VCV)
Also called: volume-limited, volume-control, volume-assist, or volume-targeted ventilation.
- Volume (VT) is the target - ventilator generates whatever pressure is needed to reach the set VT
- Clinician sets: VT, RR, FiO2, PEEP, flow rate, flow waveform (decelerating or square), I:E ratio, trigger sensitivity
- Most familiar and commonly used mode in adults
- Advantage: guarantees reliable tidal volume
- Disadvantage: does not account for dynamic changes in lung compliance; high airway pressures if compliance decreases
- Typical initial settings (VCV-AC): RR 10-14, VT 7-8 mL/kg IBW, PEEP 5 cm H2O, FiO2 100%, flow rate 60 L/min, decelerating waveform
C. Pressure-Cycled Ventilation (PCV)
Also called: pressure-control, pressure-targeted, pressure-limited ventilation.
-
Pressure is the target - ventilator delivers to a set pressure level; VT varies with compliance and resistance
-
Clinician sets: pressure high, PEEP, RR, FiO2, inspiratory time (Ti)
-
VT not guaranteed - improves (rises) as compliance improves, decreases if compliance worsens
-
Advantage: limits peak airway pressure, potentially safer for injured lungs
-
Disadvantage: VT is not fixed; requires close monitoring of VT and minute ventilation alarms
-
Typical initial settings (PCV-AC): RR 12-16, pressure high 20 cm H2O, PEEP 5, FiO2 100%; monitor VT to target 7-8 mL/kg IBW
-
CASH, p. 227
D. Assist-Control (AC) Ventilation
- Ventilator delivers machine (control) breaths at a preset rate
- Every breath - whether patient-initiated or machine-initiated - is fully supported to the set target (VT in VCV, or pressure in PCV)
- If patient breathes faster than the set rate, additional assist breaths are triggered
- Advantage: guarantees minimum minute ventilation, reduces work of breathing completely
- Disadvantage: risk of hyperventilation (respiratory alkalosis); risk of auto-PEEP (breath stacking) in patients with high intrinsic RR, particularly in asthma where auto-PEEP can reduce cardiac output and cause cardiovascular collapse
- In VCV-AC: every breath (control + assist) receives the same set VT
- In PCV-AC: every breath receives the same set pressure
"Caution should be exercised to avoid auto-PEEP (also known as breath stacking) when using volume-targeted AC modes." - CASH, p. 228
E. Synchronized Intermittent Mandatory Ventilation (SIMV)
- Delivers a preset number of machine breaths (as VCV or PCV)
- Patient can trigger additional spontaneous breaths between the mandatory breaths - these are NOT fully supported
- Spontaneous breaths above the preset rate receive only patient-generated VT (high work of breathing)
- Typically combined with PSV to support spontaneous breaths and overcome circuit resistance
- SIMV has fallen out of favor - studies show it increases ventilator days and delays liberation compared to PSV or AC weaning protocols
- Murray & Nadel, p. 3175
F. Pressure-Regulated Volume Control (PRVC) / Volume Support (VS)
These are dual-control modes that combine volume targeting with pressure delivery:
-
PRVC (pressure-regulated volume control): A type of pressure-control (PACV) mode using VT as feedback to continuously adjust the pressure target
- If respiratory mechanics improve → applied pressure decreases
- If respiratory mechanics worsen → applied pressure increases
- Guarantees volume while limiting pressure
-
Volume Support (VS): Patient-triggered, pressure-targeted, flow-cycled PSV where pressure is auto-adjusted to achieve a target volume
- Increasing patient effort → lower applied pressure (automatic unloading)
- Decreasing patient effort → higher applied pressure
-
Murray & Nadel, p. 3175
G. Adaptive Support Ventilation (ASV)
- Assist-control, pressure-targeted, time-cycled mode
- Clinician sets only: desired minute ventilation and patient height (for dead space estimation)
- Ventilator uses respiratory system mechanics to automatically select VT-frequency pattern
- Murray & Nadel, p. 3175
H. Airway Pressure Release Ventilation (APRV) / Bi-Level Ventilation
An open-lung mode that differs fundamentally from cyclic ventilation.
Settings:
| Parameter | Typical Range |
|---|---|
| Pressure High (P-high) | 20-40 cm H2O or higher |
| Pressure Low (P-low) | Near 0 cm H2O |
| Time High (T-high) | 4-6 seconds (majority of cycle) |
| Time Low (T-low) | 0.2-0.8 sec (restrictive) / 0.8-1.5 sec (obstructive) |
How it works:
- Patient spends most time at P-high → establishes oxygenation via sustained recruitment
- Brief release to P-low → clears CO2 (elastic recoil drives large-volume gas flow)
- Patient can spontaneously breathe in ALL phases of the cycle (unique "floating valve" system)
- No traditional set respiratory rate; T-high + T-low = one "phase cycle"
Key differences from IRV (inverse ratio ventilation):
- IRV requires paralysis/heavy sedation; APRV/Bi-Level does not
- Patient can exhale 50-200 mL during P-high phase (excess gas release)
- More comfortable; reduces sedation requirements
Indications: Severe ARDS, refractory hypoxemia, neonatal/pediatric/adult respiratory failure
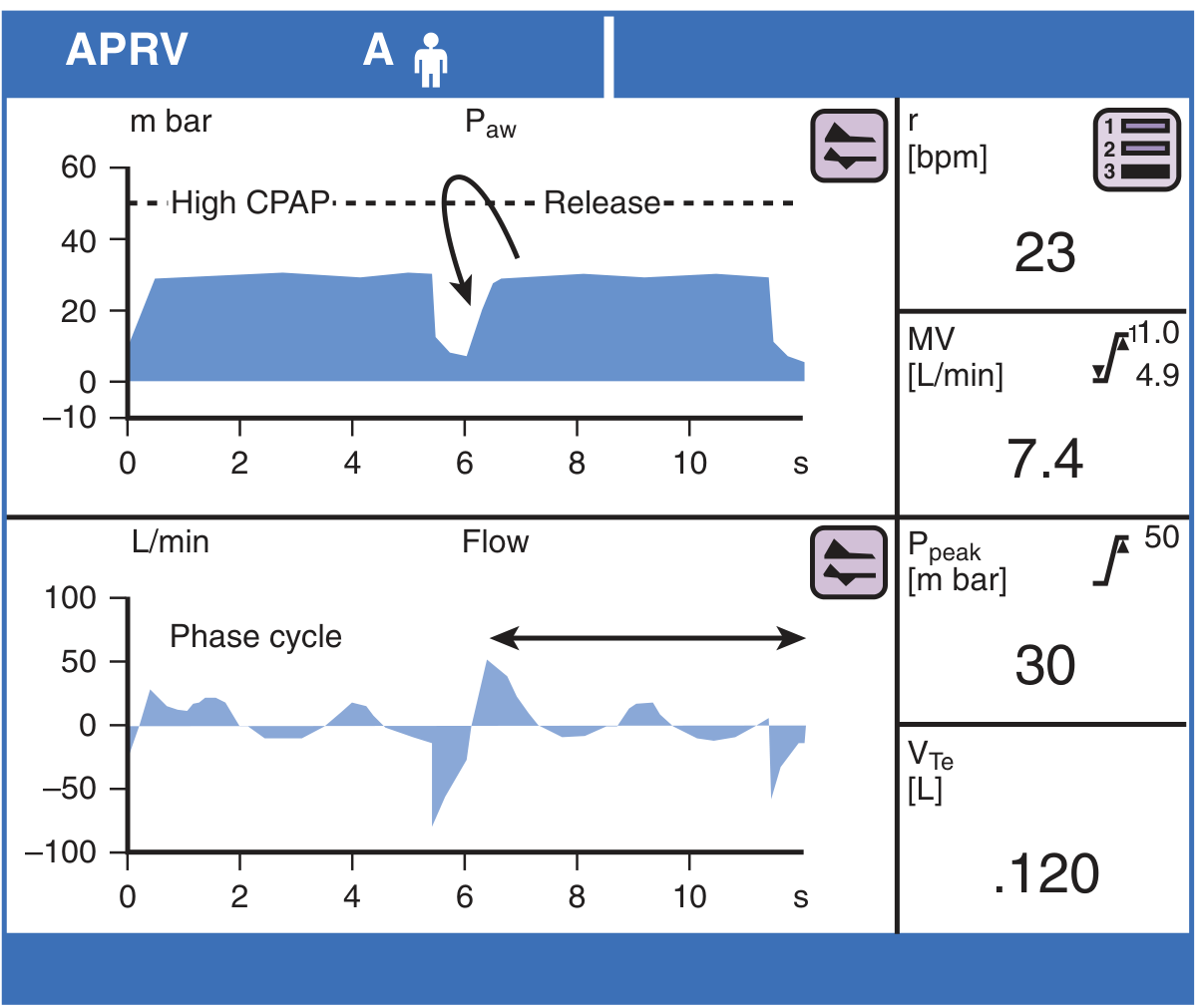
APRV traces: P-high maintained for ~4-5 seconds (oxygenation phase), followed by brief release (CO2 clearance). Flow trace shows spontaneous breathing activity throughout P-high, and large negative flow during release consistent with alveolar recruitment.
- CASH, p. 229
I. Advanced Modes: PAV+ and NAVA
These modes address a key deficiency of all traditional modes - none delivers pressure in proportion to patient effort:
-
Proportional Assist Ventilation with load-adjustable gain factors (PAV+):
- Uses transient end-inspiratory occlusions to measure elastance and resistance
- Delivers a fixed proportion of the total inflation pressure needed
- As patient effort increases → ventilator pressure increases proportionally (true unloading)
-
Neurally Adjusted Ventilatory Assist (NAVA):
- Delivers pressure proportional to diaphragmatic electrical activity (Edi signal)
- Edi acquired from EMG electrodes on an esophageal catheter detecting diaphragmatic crura activation
- Highest synchrony mode available
-
Murray & Nadel, p. 3176
4. Modes Commonly Used in the ED (CASH Summary)
"Assist/control (AC) and SIMV are the ventilation modes most commonly used in the ED. Both are acceptable, and no data have demonstrated a better outcome with either mode." - CASH, p. 228
Initial Ventilator Settings Quick Reference (from CASH)
| Mode | RR | VT / Pressure | PEEP | FiO2 | Notes |
|---|---|---|---|---|---|
| VCV-AC | 10-14 | 7-8 mL/kg IBW | 5 cm H2O | 100% | Flow 60 L/min, decelerating waveform |
| PCV-AC | 12-16 | Pressure 20 cm H2O | 5 cm H2O | 100% | Monitor VT, target 7-8 mL/kg IBW |
| SIMV | As above | VCV or PCV settings + add PSV | 5 | 100% | Add PSV to support spontaneous breaths |
Adjustments:
- FiO2: titrate based on SpO2 or PaO2
- PEEP: increase for persistent hypoxia
- Minute ventilation: adjust based on blood pH (note: on AC, decreasing RR does NOT change minute ventilation if patient breathes above set rate)
5. Ventilator Components and Circuit Considerations (Murray & Nadel)
- Gas blenders: Mix air + O2 to produce FiO2 0.21-1.0; newer systems also blend heliox, nitric oxide, anesthetic agents
- PEEP valve: Maintains positive airway pressure throughout expiration to keep alveoli patent and improve V/Q matching
- Humidification: Required because upper airway is bypassed
- Active humidifiers: external water source, heat to ≥35°C, water content ≥40 mg/L
- Passive (HME) humidifiers: capture heat/moisture from expired gas; adequate for short-term MV (≥30-33°C, ≥28-32 mg/L)
- Aerosol delivery: Bronchodilators, steroids, vasodilators, antibiotics via in-line nebulizers or MDI adapters; optimal position is inspiratory limb, several cm proximal to Y-connector
- Circuit compliance: Flexible tubing has compliance of 2-4 mL/cm H2O - applied pressure may distend circuit rather than reach lungs when airway opening pressure is high
Summary Table: Modes at a Glance
| Mode | Trigger | Target | Cycle | Patient Controls |
|---|---|---|---|---|
| PSV | Patient | Pressure | Flow ↓ to threshold | Rate, VT |
| VCV-AC | Patient or machine | Volume | Volume reached | Nothing (fully supported) |
| PCV-AC | Patient or machine | Pressure | Time | Nothing (fully supported) |
| SIMV | Machine (mandatory) + Patient (spontaneous) | Volume or Pressure | Volume/Time | Spontaneous VT above set RR |
| PRVC | Patient or machine | Volume (pressure adjusts) | Time | Nothing |
| ASV | Machine | Mechanics-calculated | Time | Nothing |
| APRV/Bi-Level | Phase cycle (no traditional trigger) | Pressure High/Low | Time | Breathe in any phase |
| PAV+ | Patient effort | Proportional pressure | Flow | Rate, depth |
| NAVA | Edi (diaphragm EMG) | Proportional pressure | Edi ↓ | Rate, depth |
Key Clinical Pearls:
- Plateau pressure must stay ≤30 cm H2O to avoid ventilator-induced lung injury (VILI)
- Auto-PEEP in asthma on AC-VCV can cause cardiovascular collapse - monitor flow-time curves for incomplete exhalation
- SIMV delays liberation from MV - most guidelines now favor AC + spontaneous breathing trials
- Lung-protective strategy: VT 6 mL/kg IBW, Pplat ≤30, adequate PEEP
- On AC mode, decreasing RR will NOT reduce minute ventilation in a patient who is breathing above the set rate
This is a shared conversation. Sign in to Orris to start your own chat.