look at the case presentation. help me study everything from basic to advanced level about 6th nerve palsy, what are its differentials and final diagnosis? recent advances and any clinical trials associated?
Reading File
Reading File
Running Command
Finding Sources
Searching PubMed
"sixth nerve palsy" OR "abducens palsy" AND etiology diagnosis
Running Command
Finding Sources
Searching PubMed
"abducens nerve palsy" treatment management clinical trial
Running Command
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"abducens nerve" palsy botulinum toxin prism treatment
Reading File
Reading File
Finding Sources
Searching PubMed
"sixth nerve palsy" stroke brainstem infarction young adults
Reading Article
Finding Sources
Searching the Web
6th nerve palsy pontomedullary junction infarction young adult management 2024 2025
Here is a complete breakdown of everything you need to study for this case - from basic to advanced.
Quick Case Recap
27F, sudden-onset binocular horizontal diplopia + headache x 7 days. Left eye restricted abduction. No ptosis, no papilledema, pupils normal. MRI: pontomedullary junction infarction.
Final Diagnosis: Left CN VI (Abducens) Palsy secondary to Pontomedullary Junction Infarction
What I covered in the study guide above:
Part 1 - Basic Anatomy: The abducens nucleus (floor of 4th ventricle), its two neuron types (motor + interneurons via MLF), and why a nuclear lesion causes gaze palsy vs. a nerve lesion causing only lateral rectus weakness.
Part 2 - Topographic Localization: The full course of CN VI (longest intracranial course of any CN), each segment's vulnerabilities, and the classic brainstem syndromes - Millard-Gubler, Foville, Raymond.
Part 3 - Etiology: Complete causes organized by adults vs. children, with the 2023 epidemiological data showing microvascular ischemia remains #1 (36.7% of 807 patients).
Part 4 - Clinical Features: Two actual clinical photographs from Wills Eye Manual showing isolated CN VI palsy, plus the face turn sign and why forced duction testing is key.
Part 5 - Differentials Analyzed: All 5 differentials from the presentation plus 7 more exam-critical mimickers (thyroid eye disease, MG, Duane syndrome, convergence spasm, etc.) with distinguishing features.
Part 6 - Workup: Step-by-step protocol for adults and children, indications for MRI (especially important here - young patient, no vascular risk factors).
Part 7 - Management: Patch/prism → botulinum toxin → surgery pathway, with the 2024 meta-analysis (79% success with BoNT in acute palsy, OR 2.67 vs expectant management).
Part 8 - Advanced Brainstem Syndromes: One-and-a-half syndrome, eight-and-a-half syndrome table.
Part 9 - Recent Advances: 6 key papers from 2023-2025 including BoNT meta-analysis (PMID: 38112391), the 807-patient etiological study, stroke-risk-after-CN-palsy study, and COVID-19 association.
Part 10 - Why This Case Is Unusual: A 27-year-old woman with a brainstem infarct should trigger a hypercoagulable workup, PFO screening, and OCP history - not just traditional vascular risk factor modification.
what are the viva questions that can be asked?
Here are the viva questions you are most likely to face, organized from basic to advanced, with expected answer depth at each level.
🔴 LEVEL 1 — Basic Anatomy & Physiology
Q1. Where is the abducens nucleus located?
Floor of the 4th ventricle, in the dorsal pons, beneath the facial colliculus (facial nerve fibers loop around it - forming the "facial colliculus" on the floor of the 4th ventricle).
Q2. What does the abducens nerve supply?
The ipsilateral lateral rectus muscle - responsible for abduction of the eye.
Q3. What are the two types of neurons in the abducens nucleus?
(1) Motor neurons - whose axons form CN VI and innervate the ipsilateral lateral rectus. (2) Interneurons - whose axons cross the midline, ascend in the contralateral MLF, and synapse on the contralateral medial rectus subnucleus of CN III - coordinating conjugate horizontal gaze.
Q4. Why does a nuclear lesion cause a gaze palsy while a nerve lesion causes only lateral rectus weakness?
Because the nucleus contains both the motor neurons (for LR) AND the interneurons that travel via the contralateral MLF to drive the medial rectus. A nuclear lesion destroys both, producing a complete ipsilateral conjugate horizontal gaze palsy. A fascicular/nerve lesion only affects the motor axons to LR.
Q5. What action does the lateral rectus perform?
Pure abduction (outward movement) of the eye in the horizontal plane. It is the primary abductor; the only muscle innervated by CN VI.
🟠 LEVEL 2 — Clinical Presentation
Q6. What type of diplopia does CN VI palsy produce?
Binocular, horizontal diplopia - worse at distance than near, and maximal in the direction of the paretic lateral rectus (ipsilateral gaze). Covering either eye eliminates it (distinguishes from monocular diplopia which is a refractive/corneal issue).
Q7. What is the primary position finding in CN VI palsy?
Esotropia - the affected eye deviates medially because the medial rectus is unopposed with loss of lateral rectus function.
Q8. What is the compensatory head posture adopted and why?
The patient turns the face toward the side of the palsy (ipsilateral face turn). This places the eyes in a position where the paretic lateral rectus is not being demanded, reducing or eliminating diplopia.
Q9. Why is diplopia worse at distance than near?
At distance fixation, both eyes need to maintain slight divergence. The paretic lateral rectus cannot generate sufficient force, so the deviation is more pronounced. At near, convergence demand partially compensates.
Q10. What is the Hirschberg finding in this case?
Left eye 5° esotropia - the light reflex falls nasal to the corneal center of the left eye, indicating that the left eye is deviating medially (esotropia) due to left lateral rectus weakness.
🟡 LEVEL 3 — Localization & Syndromes
Q11. Why is CN VI called a "false localizing sign" in raised ICP?
CN VI has the longest intracranial course of any cranial nerve. In raised ICP, the brainstem is displaced downward (caudally), stretching CN VI over the petroclinoid ligament or compressing it against the clivus. The nerve is damaged at a point distant from the primary lesion - so CN VI palsy does NOT indicate a pontine lesion when raised ICP is present.
Q12. What is Gradenigo syndrome? What causes it?
A triad of: (1) CN VI palsy, (2) retroorbital facial pain (CN V1 trigeminal), (3) ipsilateral deafness (CN VIII). Caused by inflammation/infection at the petrous apex (Dorello canal), classically from complicated otitis media. The canal is a narrow bony tunnel under the petroclinoid ligament where CN VI is most vulnerable.
Q13. Name the brainstem syndromes involving CN VI.
| Syndrome | Structures | Key Features |
|---|---|---|
| Millard-Gubler | CN VI fascicle + CN VII + pyramidal | Ipsilateral CN VI + VII, contralateral hemiplegia |
| Foville | PPRF/CN VI nucleus + CN VII + spinothalamic | Ipsilateral gaze palsy + facial palsy, contralateral hemiplegia/hemisensory loss |
| Raymond | CN VI fascicle + pyramidal tract | Ipsilateral CN VI, contralateral hemiplegia only |
Q14. What is one-and-a-half syndrome? What structure is damaged?
Lesion at the PPRF or CN VI nucleus + ipsilateral MLF. Result: ipsilateral horizontal gaze palsy (one full gaze direction gone) + ipsilateral INO (failure of adduction on the other side). The only remaining horizontal eye movement is abduction of the contralateral eye. Caused by demyelination, stroke, or hemorrhage in the paramedian pontine tegmentum.
Q15. How does a cavernous sinus lesion differ from an isolated CN VI palsy?
A cavernous sinus lesion can cause CN VI palsy BUT typically also involves CN III, CN IV, and CN V1/V2 (pain/sensory loss in forehead and cheek), plus Horner syndrome (sympathetic fibers travel with the ICA through the sinus). Proptosis and chemosis may occur with cavernous sinus thrombosis. An isolated CN VI with no other cranial nerve signs does NOT localize to the cavernous sinus.
🟢 LEVEL 4 — Differentials & Investigation
Q16. What are the differentials for limited abduction of the eye?
- CN VI palsy (neurogenic) - negative forced duction
- Thyroid eye disease - restrictive, positive forced duction, proptosis, lid lag
- Myasthenia gravis - variable/fatigable, positive ice test
- Duane syndrome Type 1 - congenital, globe retraction on adduction
- Orbital blowout fracture with medial rectus entrapment - positive forced duction, history of trauma
- Convergence spasm - miotic pupils, intermittent, ductions full
- Idiopathic orbital inflammatory syndrome - pain, proptosis
Q17. What is forced duction testing and what does it tell you?
A drop of topical anesthetic is instilled, the conjunctiva is grasped with forceps at the limbus, and the eye is mechanically rotated in the direction of limited movement. Positive (resistance felt) = restrictive cause (thyroid eye disease, entrapment, fibrosis). Negative (eye moves freely) = neurogenic or myogenic cause (CN VI palsy, MG).
Q18. How do you differentiate CN VI palsy from myasthenia gravis clinically?
MG: symptoms fluctuate during the day (worse in evening), variable ptosis, fatigability on sustained upgaze (Cogan lid twitch), positive ice test (ptosis improves with ice), positive edrophonium test, positive acetylcholine receptor antibodies. CN VI palsy: constant, no ptosis, no fatigability, no diurnal variation.
Q19. In this young patient (27F), what specific investigations would you add beyond routine workup?
Given young age and no classical vascular risk factors:
- MRI/MRA brain and brainstem (done - showed pontomedullary infarction)
- Echocardiography + bubble contrast study (rule out PFO - patent foramen ovale, present in ~25% of young stroke patients)
- Hypercoagulable screen: antiphospholipid antibodies, Factor V Leiden, Protein C/S, antithrombin III
- OCP/hormonal contraceptive history
- ANA, ANCA, vasculitis screen
- Fasting glucose, HbA1c, lipids (baseline)
- ECG + Holter (rule out paroxysmal AF as embolic source)
Q20. When is MRI mandatory in isolated CN VI palsy?
- Young patient without vascular risk factors (as here)
- Any additional neurological sign or symptom
- Bilateral CN VI palsy
- Papilledema on fundus examination
- Palsy not resolving within 3-6 months
- Increasing abduction deficit on follow-up
🔵 LEVEL 5 — Management & Advanced
Q21. What is the management plan for this patient?
- Neurology consult - acute ischemic stroke protocol
- Antiplatelet therapy (aspirin ± clopidogrel depending on stroke workup)
- Risk factor modification
- Investigate underlying cause (PFO, coagulopathy in this young patient)
- Symptomatic - occlusion patch or fogging tape for diplopia
- Prism glasses if angle is stable
- Monitor every 6 weeks
- Botulinum toxin injection (medial rectus) if palsy persists beyond 3-6 weeks
- Strabismus surgery if no recovery at 6 months with stable deviation
Q22. What is the role of botulinum toxin in CN VI palsy? What is the evidence?
BoNT-A is injected into the ipsilateral medial rectus - this prevents medial rectus contracture while the lateral rectus recovers, and also reduces the angle of deviation. Best used in the acute phase (within 3-6 weeks).2024 Meta-Analysis (Khalili et al., 38 studies, 643 patients):
- Success rate in acute palsy: 79%, chronic palsy: 33%
- Symptomatic response: 84%, functional response: 64%
- OR 2.67 vs expectant management in acute palsy
- Diabetic etiology has highest success rate
Q23. When and what surgical procedure is indicated in complete CN VI palsy?
Surgery is indicated when the deviation is stable and there is no recovery at 6 months. For complete palsy: vertical rectus transposition procedures are used since there is no functional lateral rectus to resect:
- Hummelsheim procedure (split superior and inferior rectus transposed laterally + medial rectus recession)
- Jensen procedure (partial tendon transposition)
- Full tendon transposition augmented with BoNT
For partial palsy with some recovery: medial rectus recession ± lateral rectus resection
Q24. What is the prognosis of CN VI palsy?
- Vasculopathic/microvascular causes: ~70-80% recover spontaneously within 3-6 months
- Idiopathic: similar good prognosis
- Trauma, inflammation: generally good
- Neoplasm: poor prognosis without treating the primary
- This patient (brainstem infarct): depends on extent of infarction and stroke management; partial recovery is common with early rehabilitation
Q25. Why is this case unusual - why does a 27-year-old woman get a brainstem infarct?
Young stroke (age <45) has different risk factors from elderly stroke:
- Patent foramen ovale (PFO) - paradoxical embolism
- Oral contraceptive use - prothrombotic
- Antiphospholipid syndrome
- Cervical artery dissection (vertebral artery dissection → posterior circulation stroke)
- Hypercoagulable states
- Vasculitis (SLE, ANCA)
- Cardiac embolism (structural defects, paroxysmal AF)
- Migraine with aura (small increased risk) This mandates a full young stroke workup beyond simply checking glucose and BP.
⚫ BONUS — Examiner Trap Questions
Q26. A patient has an esotropia worse at distance but single vision at near - is this CN VI palsy?
Not necessarily. This is the pattern of divergence insufficiency, which can be benign (primary divergence insufficiency) OR can indicate bilateral subtle CN VI palsy from raised ICP. You must examine for papilledema, obtain full history, and consider MRI.
Q27. If you see CN VI palsy in a patient with otitis media, what must you rule out?
Gradenigo syndrome - petrous apicitis. The triad is CN VI palsy + retroorbital pain + ipsilateral deafness. Requires urgent imaging (CT temporal bone + MRI brain) and IV antibiotics; may need surgical drainage.
Q28. Can raised ICP cause bilateral CN VI palsy?
Yes - and this is an important sign. Bilateral CN VI palsy without any other explanation is a raised ICP sign until proven otherwise. Get urgent fundoscopy (papilledema?), CT/MRI, and investigate for intracranial hypertension (pseudotumor cerebri, mass lesion, CSF drainage obstruction).
Q29. What is Dorello's canal?
A fibro-osseous canal at the petrous apex of the temporal bone, through which CN VI passes along with the inferior petrosal sinus. The canal is bounded above by the petroclinoid ligament (Gruber's ligament). CN VI is particularly vulnerable here because it makes a sharp angle as it enters the canal, making it susceptible to compression in raised ICP, petrous apicitis, and trauma.
Q30. A patient recovers from CN VI palsy in 2 months. Six months later, it recurs. What do you think?
Recurrent CN VI palsy is a RED FLAG. This is NOT vasculopathic behavior (those are single episodes that resolve). Differentials include:
- Neurovascular compression (vascular loop at root entry zone - emerging cause)
- Recurrent demyelination (MS)
- Nasopharyngeal carcinoma / skull base tumor (most dreaded)
- Meningeal carcinomatosis
- Recurrent post-viral (in children, COVID-19 reported) Requires urgent repeat MRI with contrast and ENT evaluation.
These 30 questions cover every level an examiner is likely to probe - from "where is the nucleus" to "recurrent palsy red flags." The case's unusual feature (young woman, pontine infarct) gives the examiner an easy opening to push toward the young stroke workup - make sure that part is solid.
explain the diplopia charting. how do we do it? explain from very beginning
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
I now have everything needed. Let me write the complete, clear explanation.
Diplopia Charting - Complete Explanation from the Very Beginning
Part 1 - The Fundamental Concept: Why Does Diplopia Happen?
Before understanding charting, you need to understand why two images form.
Normal Situation
Both foveae (the point of highest resolution in each retina) are aimed at the same object. The brain fuses the two images into one. This is called bifoveal fixation.
When a Muscle is Weak (e.g., Left Lateral Rectus Palsy)
The left eye cannot abduct properly. When the patient looks left:
- The right eye moves fully left - its image falls on the fovea (true image, correctly localized)
- The left eye lags behind - the object's image falls on a point nasal to the fovea (extrafoveal, incorrectly localized)
The brain projects each image according to where on the retina it falls:
- A nasal retinal image is projected temporally (outward)
- So the left eye's image is projected too far to the left - this becomes the false/peripheral image
The result: the patient sees two images side by side - one real, one displaced.
The Two Golden Rules of Diplopia Analysis
(Adams & Victor's Neurology, 12e)
- The direction in which the images are most widely separated = the direction of action of the paretic muscle
- The more peripheral (outer/further displaced) image belongs to the eye with the paretic muscle
Part 2 - Crossed vs. Uncrossed Diplopia
This is a concept students get confused about. Here is the simple way to understand it:
Uncrossed (Homonymous) Diplopia
- Occurs in esotropia (eye turns IN - e.g., CN VI palsy)
- The deviated eye's image is on the same side as the deviated eye
- Example: Left CN VI palsy → left eye turns in → left eye's false image appears on the LEFT side
- The images do NOT cross over
Crossed (Heteronymous) Diplopia
- Occurs in exotropia (eye turns OUT - e.g., CN III palsy, medial rectus palsy)
- The deviated eye's image is on the opposite side from the deviated eye
- The images cross over each other
Memory trick: In esotropia (eye turns IN) = UNcrossed. In exotropia (eye turns OUT) = CROSSED.
Part 3 - Methods of Diplopia Charting
There are several methods, from simple bedside tests to formal charting. They all use the same underlying principle - dissociate the two eyes and map where each image lands.
Method 1: Simple Torch Test (Bedside - No Equipment)
How to do it:
- Sit the patient 1 meter in front of you
- Hold a small torch/penlight at eye level
- Ask the patient to look at the light
- Move the light through the 9 positions of gaze (see below)
- Ask: "Where do you see two lights? Where are they farthest apart?"
9 Positions of Gaze:
Up-Left | Up | Up-Right
Left | Primary | Right
Down-Left | Down | Down-Right
What to ask in each position:
- "Do you see one light or two?"
- "Are they side by side (horizontal) or one above the other (vertical)?"
- "Which position makes them farthest apart?"
Limitation: You cannot tell which eye sees which image without dissociating the eyes. That is why we use colored glasses.
Method 2: Red Glass Test (Bedside - Essential to Know)
This is the most important bedside diplopia charting method.
Equipment needed: A red glass/filter (placed over one eye - by convention, always the RIGHT eye)
How to do it:
- Dim the room lights slightly
- Place the red glass over the right eye
- Hold a penlight 1 meter away from the patient
- Move through all 9 positions of gaze
- Patient reports: position of the red image vs. white image
Why it works: Now you know which eye sees which image:
- Red image = Right eye
- White image = Left eye
Interpretation (the key rule):
The image that is farther away from the center (more peripheral) belongs to the paretic eye
Plotting the chart:
- Draw a 3x3 grid representing the 9 gaze positions
- In each position, mark two dots: one red (RE image), one white (LE image), as the patient reports them
- The position where the dots are farthest apart = direction of the paretic muscle
Applying Red Glass to This Case (Left CN VI Palsy)
| Gaze Position | What Patient Sees |
|---|---|
| Primary position | Slight separation - white image (LE) slightly to the left of red |
| Left gaze | Maximum separation - white image far to the left |
| Right gaze | Images overlap or minimal separation |
| Up/Down | Minimal or no separation |
Interpretation:
- Maximum separation in left gaze → paretic muscle acts in left gaze
- The white image (left eye) is the peripheral one → left eye is paretic
- Left eye's paretic muscle acting in left gaze = Left Lateral Rectus
- Diagnosis confirmed: Left CN VI palsy
The image below shows the diplopia fields for each individual muscle paralysis using the Maddox rod (same principle):
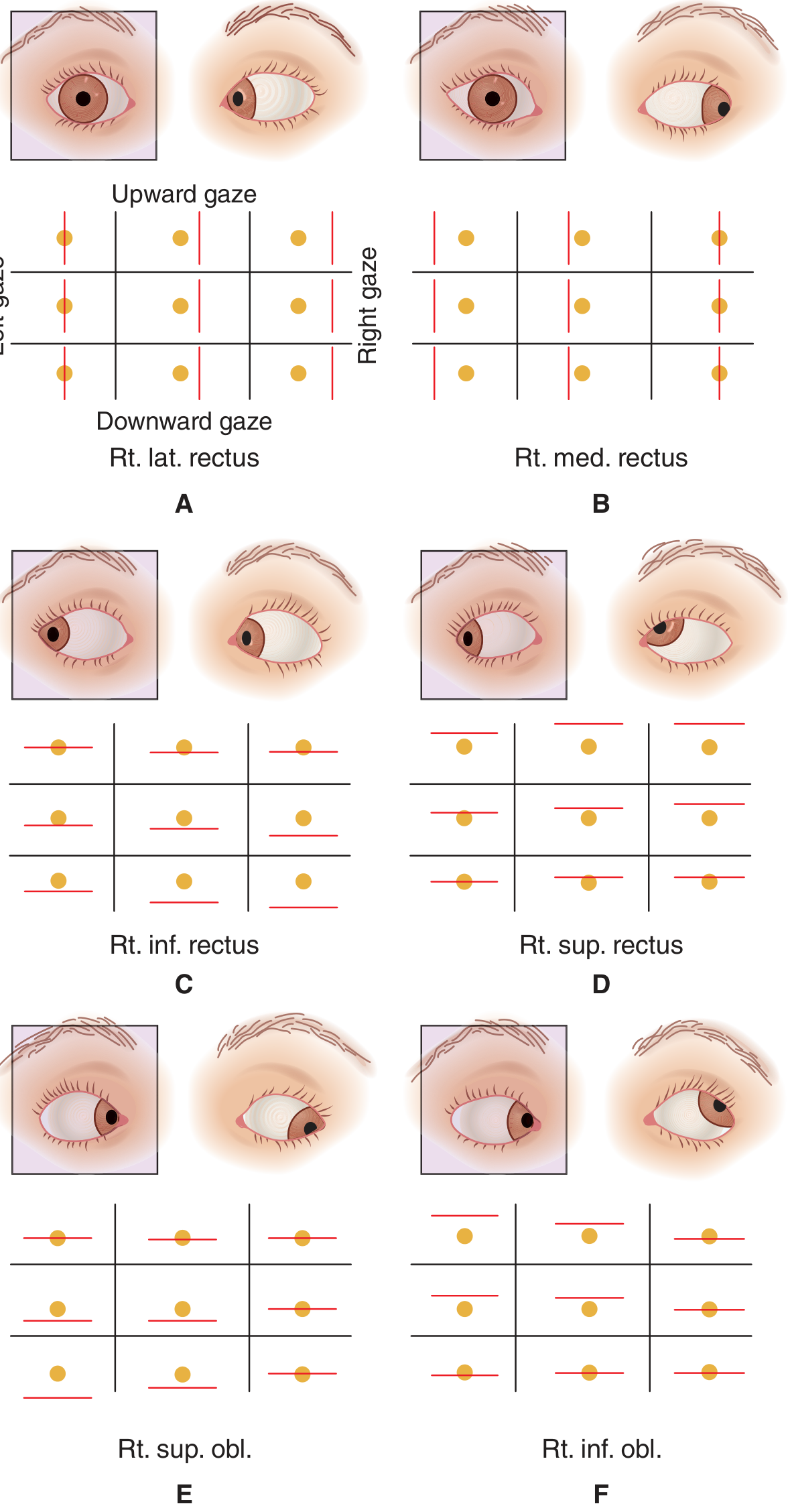
Panel A = Right lateral rectus palsy: vertical red line displaced to the RIGHT, separation increases on right gaze. In left CN VI palsy, the same pattern occurs but mirrored - maximum separation on left gaze.
Method 3: Maddox Rod Test
What it is: A refinement of the red glass test. Instead of just a red filter, the Maddox rod is a series of parallel red cylinders placed in front of (by convention) the right eye.
How it works: A point of light seen through the rod is transformed into a red line perpendicular to the cylinders. This completely dissociates the two images (a dot vs. a line), making fusion impossible. This allows detection of even very small deviations (heterophorias) that the red glass misses.
Maddox rod orientations:
- Cylinders horizontal → patient sees a vertical red line (tests horizontal deviation)
- Cylinders vertical → patient sees a horizontal red line (tests vertical deviation)
- Cylinders oblique → tests for torsional diplopia (cyclotorsion)
Reading the result (horizontal test - cylinders horizontal → vertical red line):
- Red line to the RIGHT of the white dot → uncrossed → the right eye (with rod) is deviating IN = right esotropia = right CN VI palsy
- Red line to the LEFT of the white dot → crossed → exotropia
Advantage over red glass: Can detect cyclotorsion by asking if the red line is tilted. A tilted line indicates torsional diplopia (suggests CN IV palsy or skew deviation).
Method 4: Hess Chart (Formal Charting)
This is the gold standard formal diplopia charting method used in ophthalmology departments. It gives you a permanent visual record that can be compared over time.
(Kanski's Clinical Ophthalmology 10e, section on Hess Chart and Lees Screen)
Equipment: Hess screen apparatus (a tangent screen with a dark background, red LED lights at the 9 cardinal positions in inner (15°) and outer (30°) fields), red-green goggles, green pointer.
The Principle:
The key is dissociating the two eyes using red-green glasses:
- Red lens over the fixating eye - it can only see red lights
- Green lens over the non-fixating eye - it can only see the green pointer
- Since each eye sees only its assigned color, the eyes cannot fuse - they are dissociated
How to do it (step-by-step):
- Patient sits 50 cm from the Hess screen
- Red-green goggles placed on the patient (red lens over the right eye first)
- Red lights on the screen are illuminated one at a time at each of the 9 positions (inner and outer fields)
- Patient holds a green pointer and is asked to superimpose the green light (from the pointer) over each red light on the screen
- The examiner marks on the Hess chart grid where the patient places the green pointer
- This is done for all 9 positions → plots the right eye chart (right eye is fixating through the red lens)
- Goggles are reversed (green lens now over right eye, red over left)
- The entire procedure is repeated → plots the left eye chart
Normal result: Both charts are the same size and shape, matching the template grid.
What the charts mean:
The smaller chart = the eye with the paretic muscle The larger chart = the eye with the overacting yoke muscle
(Kanski's Clinical Ophthalmology 10e)
This is based on Hering's Law of equal innervation: when you try to move a paretic muscle, you send extra innervation to it - and by Hering's law, that same extra innervation goes equally to its yoke muscle in the other eye, causing it to overact.
Why the paretic eye's chart is SMALLER:
- When the right eye (paretic) fixates and tries to point the green pointer at a red dot, it cannot move far enough in the direction of the paretic muscle
- So the green pointer lands short → the plotted chart is contracted (smaller) in the direction of the palsy
Why the yoke eye's chart is LARGER:
- When the left eye fixates, extra innervation drives the yoke muscle to overact
- The green pointer overshoots → the chart is expanded in the direction of the yoke muscle
Here is what a normal Hess chart looks like (template to compare against):
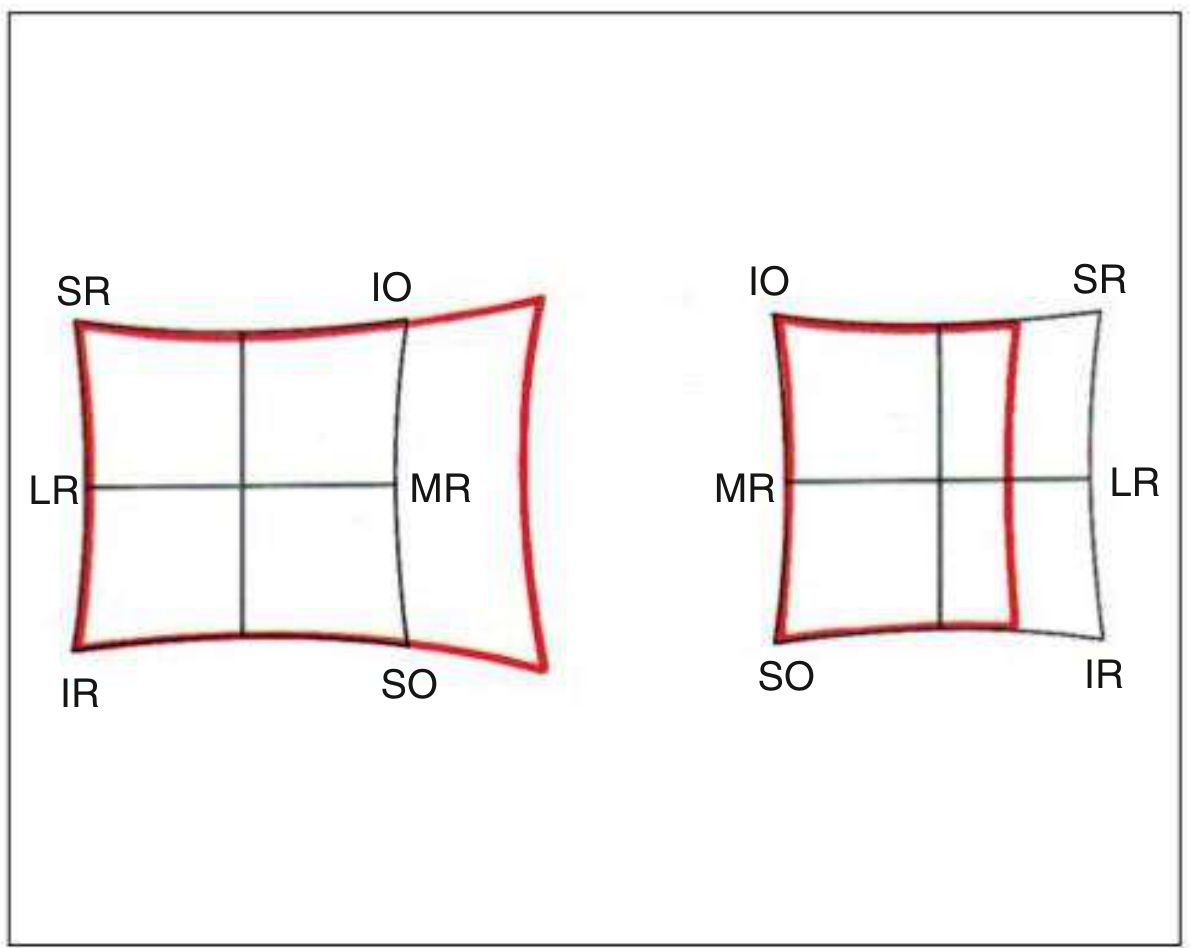
Left chart = right eye (RE). Right chart = left eye (LE). Each corner is labeled with the muscle that primarily acts in that direction. The red outline should match the black grid template in a normal patient.
Part 4 - Reading the Hess Chart in CN VI Palsy
In Right CN VI Palsy (Right Lateral Rectus Palsy):
(Kanski's Clinical Ophthalmology 10e, describing Fig. 18.41)
-
Right chart (paretic eye) - SMALLER:
- Marked underaction of the lateral rectus corner (right side of chart is pulled inward)
- Slight overaction of the medial rectus (opposite corner bulges slightly)
- Fixation spot deviated nasally (esotropia in primary position)
-
Left chart (yoke eye) - LARGER:
- Marked overaction of the medial rectus (left medial rectus is the yoke of the right lateral rectus by Hering's Law)
- The left medial rectus corner of the chart expands outward
-
Primary angle (deviation when the RIGHT paretic eye fixes): ~15°
-
Secondary angle (deviation when the LEFT normal eye fixes): ~20°
-
Secondary angle > Primary angle = confirms the paretic eye is the one that is fixing
In this case (LEFT CN VI palsy): Mirror image of the above. Left chart is smaller with underaction at the lateral rectus corner. Right chart is larger with overaction of the right medial rectus (yoke of left LR).
Part 5 - Yoke Muscles (Hering's Law) - Critical for Reading Hess Chart
This table tells you which muscle overacts on the other eye when a muscle is paretic:
| Paretic Muscle | Yoke Muscle (overacts) |
|---|---|
| Right Lateral Rectus | Left Medial Rectus |
| Left Lateral Rectus | Right Medial Rectus |
| Right Medial Rectus | Left Lateral Rectus |
| Right Superior Rectus | Left Inferior Oblique |
| Right Inferior Rectus | Left Superior Oblique |
| Right Superior Oblique | Left Inferior Rectus |
| Right Inferior Oblique | Left Superior Rectus |
Part 6 - Changes in Hess Chart Over Time
(Kanski's Clinical Ophthalmology 10e - "Changes with time")
This is important clinically and in exams:
Stage 1 - Early (acute palsy):
- Paretic eye chart: small, with underaction in direction of paretic muscle
- Yoke eye chart: large, with overaction of yoke muscle
- Charts are very unequal - easy to diagnose
Stage 2 - Intermediate:
- Secondary contracture develops in the ipsilateral antagonist of the paretic muscle (e.g., in right LR palsy, the right medial rectus contracts/shortens)
- This shows up as apparent overaction of the right MR on the right chart
- This causes inhibitional palsy of the antagonist of the yoke (left LR appears to underact)
- Now you might wrongly suspect the left LR is primarily paretic!
Stage 3 - Late (concomitant spread):
- Both charts become progressively more concomitant (equal)
- The incomitance disappears
- It becomes impossible to tell which muscle was the original culprit from the chart alone
- This is why serial Hess charts from the beginning are valuable
Clinical pearl: If a patient presents late with a comitant deviation and you have no early Hess chart, you cannot determine the primary paretic muscle from the Hess chart alone. This is why early charting matters.
Part 7 - Lees Screen (Alternative to Hess Screen)
The Lees screen uses the same Hering's Law principle but dissociates the eyes differently - using a two-sided mirror between two perpendicular screens. One eye sees one screen, the other eye sees the other. No colored glasses are needed. It is more accurate but less widely available.
Part 8 - Summary: Which Test to Use When
| Test | Setting | What It Detects | Advantage |
|---|---|---|---|
| Torch test | Bedside, no equipment | Gross diplopia, direction | Quick, no equipment |
| Red glass test | Bedside | Identifies paretic eye and muscle | Simple, ubiquitous |
| Maddox rod | Bedside/clinic | Horizontal + vertical + torsion | Detects cyclotorsion (CN IV) |
| Hess chart | Clinic/hospital | Quantifies each muscle, monitors change | Serial comparison, documents recovery |
| Lees screen | Specialist centre | Same as Hess | More accurate, no colored glasses |
Part 9 - Applying to This Case (Left CN VI Palsy)
What the diplopia chart shows in this case:
| Position | Finding |
|---|---|
| Primary position | Left esotropia (left eye in) |
| Left gaze | Maximum separation of images - white (LE) image far left |
| Right gaze | Images nearly superimposed - no diplopia |
| Up/Down gaze | Minimal separation |
Hess chart expected findings:
- Left chart: SMALLER - restricted at the lateral gaze corner (LR direction), fixation spot deviated nasally
- Right chart: LARGER - overaction of right medial rectus corner (yoke of left LR)
- Confirms: Left lateral rectus underaction = Left CN VI palsy
This matches perfectly with the restricted levoversion and restricted abduction of the left eye found on EOM testing.
Sources: Kanski's Clinical Ophthalmology 10e (Hess chart and Lees screen); Adams & Victor's Neurology 12e (Analysis of Diplopia); Bradley & Daroff's Neurology in Clinical Practice (Red glass, Maddox rod)
This is a shared conversation. Sign in to Orris to start your own chat.