Explain febrile siezures
Reading File
Finding Sources
Searching PubMed
"febrile seizures"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Febrile Seizures
Definition
A febrile seizure is a convulsion associated with fever (≥38°C / 100.4°F) in the absence of CNS infection, metabolic disturbance, or any other identifiable cause. This definition explicitly excludes seizures in children with meningitis/encephalitis, toxic encephalopathy, or a prior history of afebrile seizures. - Rosen's Emergency Medicine, p. 3158; Textbook of Family Medicine 9e
Epidemiology
-
Affect 2-5% of children in the United States - the most common convulsive disorder of young children
-
Typical age: 6 months to 5 years (some sources extend to 6 years); peak incidence is in the second year of life
-
Boys are affected slightly more often than girls
-
~one-third of children who have a first febrile seizure will have at least one recurrence
-
Rosen's Emergency Medicine, p. 3158; Textbook of Family Medicine 9e
Classification: Simple vs. Complex
| Feature | Simple | Complex |
|---|---|---|
| Duration | < 15 minutes | ≥ 15 minutes (prolonged) |
| Type | Generalized, nonfocal (tonic-clonic) | Focal component OR generalized |
| Recurrence within 24 hrs | Only once | Recurs more than once in 24 hrs |
| Age range | 6 months - 5/6 years | May be outside typical age range |
The vast majority of febrile seizures are simple. Fewer than 8% last longer than 15 minutes. - Textbook of Family Medicine 9e, Rosen's Emergency Medicine
Pathophysiology
The exact mechanism is not fully understood. Key points:
- The rapid rise or defervescence of fever has traditionally been implicated, though research does not clearly confirm this is more important than the absolute fever height
- At the temperature extremes of childhood development, neuronal excitability thresholds appear lower, making the brain more susceptible to seizure activity in the context of fever
- Genetic predisposition plays a clear role (see risk factors)
Risk Factors
For a first febrile seizure:
- Family history of febrile seizures
- Developmental delay
- Very high fever
- Child care attendance (increased infection exposure)
For recurrence:
- Younger age at first seizure (strongest predictor)
- Family history of febrile seizures
- Lower fever at the time of first seizure
- Short duration from fever onset to seizure
- Most recurrences happen within 1 year of the first episode
For developing epilepsy (risk ~1-2% vs. 0.5-1% in general population, an approximately 2-fold increase overall):
-
Pre-existing neurological disorder or developmental delay
-
Family history of epilepsy
-
Complicated/complex febrile seizure (lasted >15 min, was focal, or recurred same day)
-
If all risk factors present, risk of epilepsy rises to approximately 10%
-
Goodman & Gilman's, p. 1266; Textbook of Family Medicine 9e
Clinical Evaluation
History
- Seizure description (type, duration, focal features, post-ictal state)
- Symptoms of infection, current medications, toxic exposures
- Developmental history, birth/prenatal history
- Family history of febrile seizures or epilepsy
Physical Examination
Focus on identifying the source of fever and ruling out meningitis:
- Signs of meningeal irritation: neck stiffness, Kernig's sign, Brudzinski's sign
- Tense or bulging fontanelle (in infants)
- Petechial rash (raises concern for meningococcemia)
- Neurological status: alertness, focal deficits, tone
Lumbar Puncture (LP) - When to Perform
The AAP does not recommend routine LP for simple febrile seizures. Consider LP when:
-
Any signs of meningeal irritation
-
Child < 12 months of age (may lack classic meningeal signs)
-
Age 6-12 months: incomplete immunization against H. influenzae type b or S. pneumoniae, or unknown status
-
Child was pre-treated with antibiotics (partially treated meningitis)
-
Febrile status epilepticus (higher risk - LP should be done)
-
Child does not improve as expected during observation
-
Tintinalli's Emergency Medicine, p. 3472-3474; Rosen's Emergency Medicine, p. 3206-3208
Investigations NOT routinely indicated for simple febrile seizures:
- Blood work (CBC, electrolytes, glucose) - only if clinically indicated for fever source
- EEG
- Neuroimaging (CT/MRI)
- Skull X-ray
Any labs ordered should be aimed at identifying the source of fever, not driven by the seizure itself.
Management
Immediate (Actively Seizing Child)
- Airway - ensure patency; nasopharyngeal airway if needed
- Oxygenation - oxygen via cannula or face mask
- Circulation - IV/IO access
- Treat metabolic causes if identified:
- Hypoglycemia: 10% dextrose 5 mL/kg IV
- Hyponatremia: 3% saline 3 mL/kg IV over 30 min
- Hypocalcemia: calcium gluconate 100 mg/kg IV over 5-10 min (on cardiac monitor)
- Benzodiazepines are the first-line anticonvulsant if seizure is ongoing (standard seizure protocol)
Post-Seizure (Simple Febrile Seizure)
- Identify and treat the source of fever
- No antiseizure prophylaxis is recommended after a single simple febrile seizure
- No routine neuroimaging or EEG
- Observe in the ED for several hours
- Discharge home if: alert, fever evaluated and treated, close outpatient follow-up available
Chronic Prophylaxis - NOT recommended
Chronic phenobarbital (or other antiseizure drugs) prophylaxis is not indicated. Uncertainties about its efficacy in preventing epilepsy, combined with significant side effects (cognitive effects with phenobarbital), argue strongly against it. For high-risk children with recurrent febrile seizures, rectally administered diazepam at the time of fever may prevent recurrence while avoiding chronic side effects. - Goodman & Gilman's, p. 1266-1268
Prognosis and Parental Counseling
Parents need reassurance about the following:
-
Only 50% of children < 12 months and 30% of children > 12 months will have another simple febrile seizure
-
Fewer than 5% of children who have a febrile seizure develop epilepsy - the absolute risk increase is small
-
Simple febrile seizures do not cause brain damage or intellectual impairment
-
Children should not bathe or swim unsupervised; bathroom doors should not be locked
-
Parents should be told what to do if a seizure recurs (keep child safe, time the seizure, call emergency services if prolonged)
-
Tintinalli's Emergency Medicine, p. 2638; Harriet Lane Handbook 23e, p. 739
Post-vaccination Febrile Seizures
A special note: febrile seizures can be triggered by vaccine-associated fever. If one occurs, it is most likely:
- Within 48 hours of DTaP vaccination
- Within 10 days of MMR vaccination
These are managed the same as any febrile seizure. - Textbook of Family Medicine 9e
Key Teaching Points Summary
| Point | Key Fact |
|---|---|
| Incidence | 2-5% of children |
| Age range | 6 months - 5 years |
| Simple seizure duration | < 15 minutes, generalized, no recurrence in 24 hrs |
| LP indication | Signs of meningitis, age < 12 months, incomplete immunization, prior antibiotics |
| Routine EEG/imaging | NOT indicated |
| Antiseizure prophylaxis | NOT recommended |
| Risk of epilepsy | ~1-2% (slightly above general population) |
| Recurrence risk | ~33% overall |
Sources: Rosen's Emergency Medicine (Concepts and Clinical Practice); Tintinalli's Emergency Medicine: A Comprehensive Study; Harriet Lane Handbook (23rd ed., Johns Hopkins); Textbook of Family Medicine (9e); Goodman & Gilman's Pharmacological Basis of Therapeutics
Cerebral palsy theory and typical case presentation
Finding Sources
Searching PubMed
"cerebral palsy"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have thorough, comprehensive material from multiple authoritative sources. Let me compile the full answer.
Cerebral Palsy (CP)
Definition
Cerebral palsy is a group of nonprogressive motor impairments caused by a disturbance to the developing fetal or infant brain. The International Committee on Cerebral Palsy Classification (2005) defines it as:
"A group of developmental disorders of movement and posture, which cause activity limitations that are attributed to nonprogressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of CP are often accompanied by disturbances of sensation, cognition, communication, perception, and/or behavior, and/or by a seizure disorder."
Key elements of the definition:
-
Non-progressive brain insult (the underlying lesion does not worsen, though clinical manifestations may evolve)
-
Affects movement and posture
-
Occurs in the developing brain (prenatal, perinatal, or postnatal up to ~2 years of age)
-
Creasy & Resnik's Maternal-Fetal Medicine; Bradley & Daroff's Neurology in Clinical Practice
Epidemiology
- Prevalence: 1.5 to 3.5 per 1,000 live births - has remained relatively unchanged over the past 50 years despite improvements in perinatal care
- Congenital CP (injury before or during birth): 85-90% of cases
- Acquired CP (injury after 1 month of life): 10-15% of cases
- ~50% of patients have cognitive impairment, sometimes severe
Aetiology and Risk Factors
Timing of Injury
| Timing | Proportion |
|---|---|
| Prenatal (in utero) | 75-80% |
| Intrapartum (birth asphyxia) | ~10% |
| Postnatal (e.g., infection, trauma) | ~10% |
Prenatal Risk Factors
- Prematurity - the strongest and most important identifiable risk factor
- Very preterm (<32 weeks): incidence of CP ~8.7%
- Late preterm (34-37 weeks): ~0.6%
- Very low birth weight (<1,500 g)
- Periventricular/intraventricular hemorrhage (especially severe grades)
- Intrauterine infection (chorioamnionitis)
- Intrauterine growth restriction (IUGR)
- Multiple gestation (mediated largely through prematurity)
- Placental pathology
- Structural brain abnormalities
- Genetic syndromes (~20% of "idiopathic" cases have de novo copy number variants)
- Kernicterus (bilirubin toxicity to the globus pallidus)
Perinatal Risk Factors
- Hypoxic-ischemic encephalopathy (HIE) - the classic perinatal cause
- Perinatal stroke (ischemic, hemorrhagic, or thromboembolic) - the most common cause of acquired CP
Postnatal Risk Factors (acquired CP)
-
Meningitis or encephalitis in infancy (2nd most common cause of acquired CP)
-
Head trauma (abusive head trauma, motor vehicle accident)
-
Bradley & Daroff's Neurology; Creasy & Resnik's Maternal-Fetal Medicine; Goldman-Cecil Medicine
Classification
CP is classified by two axes: topography (which limbs are affected) and motor type (nature of the movement disorder).
By Topography
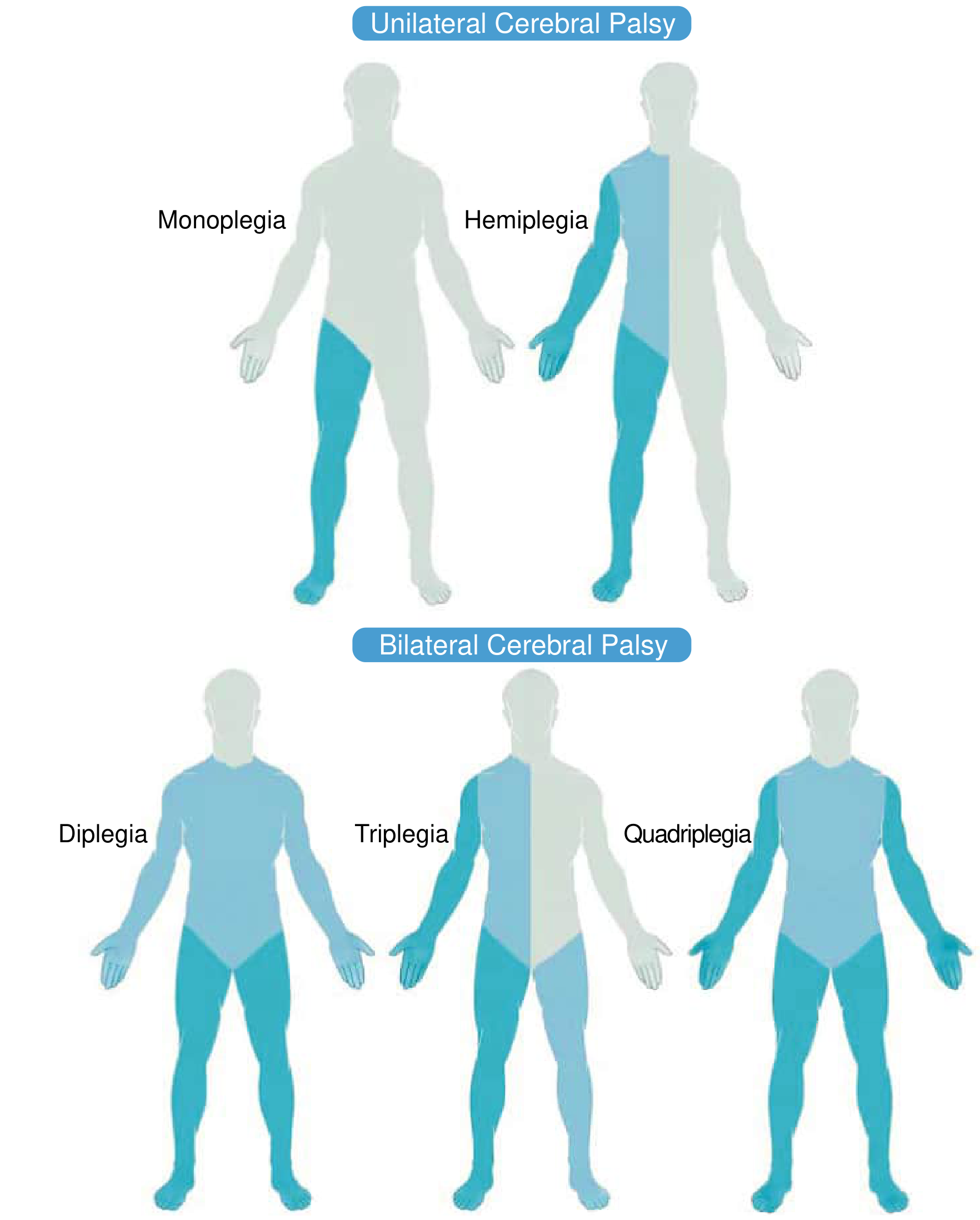
| Type | Distribution |
|---|---|
| Monoplegia | One limb only (rare) |
| Hemiplegia | One side (arm + leg); arm usually more affected than leg |
| Diplegia | Both lower limbs predominantly; arms mildly involved |
| Triplegia | Both lower extremities + one arm |
| Quadriplegia | All four limbs + trunk + face |
By Motor Type (Tone/Movement Disorder)
| Type | Features | Pathology | % of CP |
|---|---|---|---|
| Spastic | Velocity-dependent increased tone, brisk reflexes, UMN signs | Pyramidal tract damage | 70-80% |
| Dyskinetic - Dystonic | Increased tone but reduced activity, stiff movements | Extrapyramidal (basal ganglia) | ~15% |
| Dyskinetic - Choreoathetoid | Low tone but increased activity, uncoordinated jerky/writhing movements | Extrapyramidal | included above |
| Ataxic | Generalised low tone, loss of coordination, wide-based gait | Cerebellar damage | ~5% |
| Mixed | Combination (spasticity + dystonia is most common mix) | Multiple areas | variable |
| Hypotonic | Generalised floppiness - often a phase before spasticity develops | - | - |
- Bailey & Love's Surgery 28th ed.; Bradley & Daroff's Neurology; Campbell's Operative Orthopaedics 15th ed.
Pathophysiology
Spastic CP (most common)
- Injury to the pyramidal tracts (corticospinal/corticobulbar)
- Mechanism: chronic reduction in presynaptic inhibition + hyperexcitability of motor neurons through alterations in motor neuron membrane and synaptic input
- Results in velocity-dependent increase in tonic stretch reflexes (spasticity) and hyperreflexia
Dyskinetic CP
- Injury to the basal ganglia/extrapyramidal system
- Up to 70% have imaging involvement of the thalamus and basal ganglia (lenticular nucleus most common)
- Kernicterus preferentially damages the globus pallidus
- Hypoxic-ischemic events in term/near-term infants preferentially affect basal ganglia due to their high metabolic rate
Ataxic CP
- Cerebellar damage
- Results in truncal hypotonia, dysmetria, and gait ataxia
Key Neuropathological Lesion: Periventricular Leukomalacia (PVL)
- White matter necrosis in the periventricular zone - classic in premature infants
- Descending corticospinal fibers regulating lower limbs run near the ventricles, explaining why spastic diplegia (legs > arms) is the hallmark of premature birth-associated CP
- Identifiable on MRI as periventricular white matter loss/gliosis
Clinical Features
Motor Features (hallmark)
- Delayed motor milestones - often the presenting complaint
- Abnormal muscle tone - spasticity (most common), rigidity, hypotonia, or mixed
- Exaggerated deep tendon reflexes and pathological reflexes (e.g., persistent Babinski)
- Persistence of primitive reflexes (e.g., Moro, asymmetric tonic neck reflex) beyond the normal age of disappearance
- Scissor gait - classic in spastic diplegia (hip adduction and internal rotation, knees crossing)
- Hemiplegic gait (circumduction of the affected leg) in spastic hemiplegia
- Weakness - there is always a generalised, relative muscle weakness regardless of tone type
- Contractures - develop over time due to muscle imbalance and spasticity; can lead to fixed joint deformities
Associated Non-Motor Features (~50% of patients)
| Feature | Details |
|---|---|
| Cognitive impairment / intellectual disability | Present in ~50%; ranges from mild to severe |
| Epilepsy / seizures | Common, especially in quadriplegia and hemiplegia |
| Speech and language disorders | Dysarthria, oromotor dysfunction |
| Feeding difficulties | Dysphagia, risk of aspiration |
| Visual problems | Strabismus, cortical visual impairment |
| Hearing impairment | Especially in kernicterus (sensorineural) |
| Behavioural/psychiatric disorders | ADHD, anxiety, autism spectrum features |
| Sleep disturbances | Dysautonomia, pain-related |
| Bladder/bowel dysfunction | Especially in severe forms |
| Hip subluxation/dislocation | Critical concern in total body involvement (TBI/quadriplegia) |
| Scoliosis | Particularly in non-ambulant patients |
Typical Case Presentation
Scenario 1: Spastic Diplegia (Classic Premature Infant)
A 2-year-old boy, born at 28 weeks gestation, is brought by his parents because he is not yet walking. He stood briefly at 18 months. His parents note his legs "go stiff" when they try to dress him and he "walks on his tiptoes" when supported. He has been in physiotherapy since 6 months.On examination: Alert and socially engaging, speech slightly delayed. Lower limb tone markedly increased bilaterally (spasticity, velocity-dependent). Brisk knee and ankle jerks bilaterally. Sustained ankle clonus. Persistent bilateral Babinski reflex. Scissor posture of the legs when held upright. Mild hip adductor tightness. Upper limbs have mild increased tone but near-normal fine motor function. No focal cranial nerve findings.MRI brain: Periventricular leukomalacia - thinning of the posterior periventricular white matter with ex-vacuo dilation of the posterior horns of the lateral ventricles.Diagnosis: Spastic diplegia - CP secondary to PVL from prematurity.
This presentation is so classic that it is described in the literature as: "spastic diplegia associated with relative preservation of intellectual function" in premature infants. - Bailey & Love's Surgery
Scenario 2: Spastic Hemiplegia (Perinatal Stroke)
An 18-month-old girl is brought in because she only uses her right hand - she has been "hand dominant" since very early and seems to drag her right leg when crawling. Born at term with no complications.On examination: Right arm held in flexion at the elbow and wrist, with fisting. Right leg slightly shorter. Right-sided hyperreflexia and Babinski. Mild facial asymmetry. Normal cognition and speech for age.MRI brain: Focal encephalomalacia in the left MCA territory consistent with perinatal stroke.Diagnosis: Left spastic hemiplegia. Arm more affected than leg (typical pattern).
Scenario 3: Dyskinetic CP (HIE at Term)
A 3-year-old boy with a history of birth asphyxia (required resuscitation at birth, Apgar 2 at 5 minutes) presents with inability to walk, constant involuntary writhing movements of his arms, and difficulty speaking or swallowing.On examination: Fluctuating tone (sometimes hypertonic, sometimes hypotonic). Athetoid movements of all four limbs. Drooling, dysarthria. Hearing impaired (sensorineural). Intelligence appears intact - the child communicates with eye gaze.MRI brain: T2 signal abnormality in the basal ganglia and thalamus bilaterally.Diagnosis: Dyskinetic (choreoathetoid) CP following HIE. (If kernicterus: preferential globus pallidus signal on MRI.)
Investigations
| Investigation | Purpose |
|---|---|
| MRI brain (preferred) | Identify lesion type, location, severity; correlates with clinical subtype; identifies PVL, stroke, malformations |
| Head ultrasound | Useful in neonates/premature infants (periventricular hemorrhage, PVL) |
| EEG | If seizures are suspected |
| Metabolic/genetic workup | If no clear acquired cause on history/imaging - genetic causes (copy number variants, neurometabolic disorders) must be considered |
| Ophthalmology assessment | Screen for cortical visual impairment, strabismus |
| Audiology | Hearing assessment (especially if kernicterus history) |
| Gait analysis | In ambulant children, used to plan surgical/orthotic management |
| Hip X-rays (surveillance) | In non-ambulant/TBI patients - monitor for hip subluxation |
Note: Imaging is normal in up to 13% of patients with dyskinetic CP. A normal MRI without a clear risk factor history should prompt genetic investigation. - Bradley & Daroff's Neurology
Management
Multidisciplinary Team
Paediatrician, physiotherapist, occupational therapist, speech-language pathologist, orthopaedic surgeon, neurologist, psychologist, orthotist.
Spasticity Management (Stepwise)
1. Oral medications (widespread spasticity):
- Baclofen (GABA-B agonist) - first line
- Tizanidine, dantrolene, benzodiazepines (alternatives)
- Clonidine or gabapentin - dual benefit for tone + sleep/pain
2. Focal/segmental spasticity:
- Botulinum toxin A (BoNT-A) injections - chemodenervation, repeat every 4-6 months; combined with rehabilitation therapy to improve function and delay surgery
- Phenol / ethyl alcohol injections
3. Intrathecal Baclofen (ITB) pump:
- For spasticity not controlled by oral agents, or where side effects (sedation, weakness) are limiting
- Baclofen delivered directly into CSF at 1/100th the oral dose
- Reversible (unlike SDR)
- Pump requires replacement every 5-7 years; complication rates higher in children
4. Surgical - Neurological:
- Selective Dorsal Rhizotomy (SDR): Reduces spasticity by selectively cutting sensory nerve rootlets in the lumbar cord; effective for spastic diplegia; not useful for dystonia
5. Surgical - Orthopaedic:
- Muscle-tendon lengthening (restore joint range)
- Tendon transfers (rebalance muscle forces)
- Joint release / bony osteotomy (correct fixed deformity)
- Hip relocation (for subluxation in TBI)
- Spinal fusion (for scoliosis)
- Leg equalisation procedures
Other
-
Deep brain stimulation (DBS) - emerging for dystonic CP
-
Physiotherapy - cornerstone of functional rehabilitation; early intervention more effective
-
Speech therapy - language, communication, feeding
-
Orthoses (AFOs, splints) - prevent contractures, improve gait
-
Aquatic therapy, hippotherapy - emerging evidence for motor function improvement
-
Anticonvulsants - for epilepsy
-
Manage cognitive, visual, hearing, and behavioural co-morbidities
-
Goldman-Cecil Medicine; Bailey & Love's Surgery; Bradley & Daroff's Neurology
Prognosis
- CP is a lifelong condition - the brain lesion is static but functional capacity can improve with rehabilitation
- Ambulatory prognosis depends on type and severity: most children with hemiplegia and diplegia become ambulatory; many with quadriplegia do not
- The brain lesion does not progress, but secondary musculoskeletal complications (contractures, scoliosis, hip dislocation) worsen over time without management
- Intelligence may be normal, especially in spastic diplegia from prematurity
Sources: Bradley & Daroff's Neurology in Clinical Practice; Creasy & Resnik's Maternal-Fetal Medicine; Goldman-Cecil Medicine; Bailey & Love's Short Practice of Surgery (28th ed.); Campbell's Operative Orthopaedics (15th ed. 2026)
Cerebral palsy theory and typical case presentation
This is the same question you just asked! Here's the full answer again:
Cerebral Palsy (CP)
Definition
Cerebral palsy is a group of nonprogressive motor impairments caused by a disturbance to the developing fetal or infant brain. The International Committee on Cerebral Palsy Classification (2005) defines it as:
"A group of developmental disorders of movement and posture, which cause activity limitations that are attributed to nonprogressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of CP are often accompanied by disturbances of sensation, cognition, communication, perception, and/or behavior, and/or by a seizure disorder."
Key elements:
- Non-progressive brain insult (lesion does not worsen, though clinical manifestations may evolve with growth)
- Affects movement and posture
- Injury occurs in the developing brain (prenatal, perinatal, or postnatal up to ~2 years)
Epidemiology
- Prevalence: 1.5 to 3.5 per 1,000 live births - unchanged over the past 50 years despite improved perinatal care
- Congenital CP (before/during birth): 85-90% of cases
- Acquired CP (after 1 month of age): 10-15%
- ~50% have cognitive impairment (sometimes severe)
- Boys affected slightly more than girls
Aetiology and Risk Factors
Timing of Injury
| Timing | Proportion |
|---|---|
| Prenatal (in utero) | 75-80% |
| Intrapartum (birth asphyxia) | ~10% |
| Postnatal (infection, trauma) | ~10% |
Key Risk Factors
Prenatal:
- Prematurity - strongest identifiable risk factor
- Very preterm (<32 wks): CP incidence ~8.7%
- Late preterm (34-37 wks): ~0.6%
- Very low birth weight (<1,500 g)
- Periventricular/intraventricular hemorrhage
- Intrauterine infection (chorioamnionitis)
- Multiple gestation (risk largely mediated by prematurity)
- Placental pathology, IUGR
- Structural brain anomalies
- Genetic - ~20% of "idiopathic" cases have de novo copy number variants
- Kernicterus (bilirubin toxicity - targets globus pallidus)
Perinatal:
- Hypoxic-ischemic encephalopathy (HIE)
- Perinatal stroke (most common cause of acquired CP)
Postnatal:
- Meningitis/encephalitis in infancy (2nd most common acquired cause)
- Head trauma (abusive head trauma, MVA)
Classification
CP is classified on two axes: topography (which limbs) and motor type (movement disorder).
Topographic Classification
| Type | Affected Areas |
|---|---|
| Monoplegia | One limb (rare) |
| Hemiplegia | One side; arm > leg affected |
| Diplegia | Both lower limbs predominantly; arms mildly involved |
| Triplegia | Both lower limbs + one arm |
| Quadriplegia | All four limbs + trunk + face |
Motor Type Classification
| Type | Tone | Features | Pathology | Frequency |
|---|---|---|---|---|
| Spastic | High (velocity-dependent) | Brisk reflexes, UMN signs, scissor gait | Pyramidal tract damage | 70-80% |
| Dyskinetic - Dystonic | Variable (high with reduced movement) | Stiff, sustained abnormal postures | Basal ganglia (extrapyramidal) | ~15% |
| Dyskinetic - Choreoathetoid | Low with excessive movement | Writhing, jerky, uncoordinated | Basal ganglia | included above |
| Ataxic | Low (generalised) | Poor coordination, wide-based gait | Cerebellum | ~5% |
| Mixed | Variable | Combination; spasticity + dystonia most common | Multiple areas | variable |
| Hypotonic | Low | Often a transitional phase before spasticity appears | - | - |
Pathophysiology
Spastic CP
- Pyramidal tract (corticospinal) damage
- Chronic reduction in presynaptic inhibition + hyperexcitability of motor neurons
- Produces velocity-dependent increased tone, clonus, hyperreflexia, Babinski sign
Dyskinetic CP
- Basal ganglia / extrapyramidal system injury
- Up to 70% show MRI involvement of thalamus and basal ganglia (lenticular nucleus most common)
- Term/near-term HIE preferentially damages basal ganglia (high metabolic rate)
- Kernicterus selectively damages the globus pallidus
Ataxic CP
- Cerebellar damage → truncal hypotonia, dysmetria, intention tremor, gait ataxia
Key Neuropathological Lesion: Periventricular Leukomalacia (PVL)
- White matter necrosis in the periventricular zone - hallmark of premature infant brain injury
- Descending corticospinal fibres for the lower limbs run close to the ventricles - explains why prematurity causes spastic diplegia (legs worse than arms) with relative preservation of cognition
- Seen on MRI as periventricular white matter loss + ex-vacuo dilation of posterior horns
Clinical Features
Motor (Core)
- Delayed motor milestones - most common presenting complaint
- Abnormal muscle tone (spasticity, rigidity, hypotonia, fluctuating)
- Exaggerated deep tendon reflexes + pathological reflexes (persistent Babinski)
- Persistence of primitive reflexes beyond normal age (Moro, ATNR)
- Scissor gait - hip adduction/internal rotation, knees crossing (spastic diplegia)
- Hemiplegic gait - circumduction of affected leg, arm held flexed (spastic hemiplegia)
- Relative muscle weakness - present in all types regardless of tone
- Joint contractures - develop over time from muscle imbalance and spasticity
Associated (Non-Motor) Features
| Feature | Notes |
|---|---|
| Intellectual disability | ~50% of patients; severity varies |
| Epilepsy | Common, especially in hemiplegia and quadriplegia |
| Speech / dysarthria | Oromotor dysfunction |
| Feeding difficulties / dysphagia | Aspiration risk |
| Strabismus / cortical visual impairment | Vision assessment mandatory |
| Sensorineural hearing loss | Especially with kernicterus |
| Behavioural disorders | ADHD, anxiety, autistic features |
| Sleep disturbance / dysautonomia | |
| Bladder and bowel dysfunction | Especially in severe CP |
| Hip subluxation / dislocation | Primary concern in quadriplegia/TBI |
| Scoliosis | Especially in non-ambulant patients |
Typical Case Presentations
Case 1 - Spastic Diplegia (Classic Premature Infant)
A 2-year-old boy born at 28 weeks gestation is brought by his parents because he is not yet walking. He briefly stood at 18 months. Parents report his legs "go stiff" when dressing him and he "walks on his tiptoes" when supported. He has been attending physiotherapy since 6 months of age.Examination: Alert and socially engaging; speech slightly delayed. Markedly increased lower limb tone bilaterally (velocity-dependent spasticity). Brisk bilateral knee and ankle jerks. Sustained ankle clonus. Bilateral Babinski signs. Scissor posture on vertical suspension. Hip adductor tightness. Upper limbs have mildly increased tone with near-normal fine motor function. Head circumference normal.MRI brain: Periventricular leukomalacia - thinning of posterior periventricular white matter, ex-vacuo dilation of posterior horns of lateral ventricles.Diagnosis: Spastic diplegia secondary to PVL from prematurity.
This is the prototypical presentation: lower limbs far worse than upper limbs, intellectual function relatively preserved. - Bailey & Love's Surgery 28th ed.
Case 2 - Spastic Hemiplegia (Perinatal Stroke)
An 18-month-old girl born at full term with an uncomplicated delivery is referred because she only uses her left hand - she has been "left-handed" since very early, which her parents thought was unusual. She drags her right leg when crawling.Examination: Right arm held in flexed posture at elbow and wrist, fisting. Right lower limb slightly shorter, equinus posture of the foot. Right-sided hyperreflexia. Right Babinski positive. Mild right facial asymmetry. Cognition and receptive language appear normal.MRI brain: Focal encephalomalacia in the left MCA territory consistent with a remote perinatal arterial ischaemic stroke.Diagnosis: Left spastic hemiplegia. Arm more affected than leg (typical pattern).
Case 3 - Dyskinetic CP (Term HIE)
A 3-year-old boy with a history of severe birth asphyxia (Apgar 1 at 1 min, 4 at 5 min; required full resuscitation) presents with inability to walk, constant writhing movements of all four limbs, and great difficulty speaking or swallowing. Parents note he drools constantly and cannot feed himself.Examination: Fluctuating tone - intermittently hypertonic and hypotonic. Athetoid/choreoathetoid movements of all limbs, worse with intention. Facial grimacing. Severe dysarthria. Sensorineural hearing loss on audiology. When assessed with eye gaze/picture communication, the child demonstrates near-normal intelligence.MRI brain: Bilateral T2 signal abnormality in the basal ganglia and thalami.Diagnosis: Dyskinetic (choreoathetoid) CP following perinatal HIE. Cognition preserved despite severe motor disability - an important distinguishing feature of dyskinetic CP.
Investigations
| Investigation | Purpose |
|---|---|
| MRI brain (gold standard) | Lesion type, location, etiology; correlates with clinical subtype; identifies PVL, stroke, malformations |
| Head ultrasound | Useful in neonates/premature infants (IVH, PVL) |
| EEG | If seizures suspected |
| Metabolic / genetic workup | If no clear acquired cause - genetic causes must be excluded; up to 13% of dyskinetic CP have normal MRI |
| Ophthalmology | Strabismus, cortical visual impairment |
| Audiology | Hearing assessment; mandatory in kernicterus history |
| Gait analysis | In ambulant children; used to plan orthopaedic and orthotic management |
| Hip X-ray surveillance | In non-ambulant/quadriplegic patients - monitor for subluxation |
Management
Multidisciplinary Team
Paediatrician, physiotherapist, occupational therapist, speech-language pathologist, orthopaedic surgeon, neurologist, psychologist, orthotist, and social worker.
Spasticity Management (Stepwise)
Step 1 - Oral medications (widespread spasticity):
- Baclofen (GABA-B agonist) - first line
- Tizanidine, dantrolene, benzodiazepines (alternatives)
- Gabapentin or clonidine - dual benefit for tone, sleep, and pain
Step 2 - Focal chemodenervation (segmental spasticity):
- Botulinum toxin A (BoNT-A) injections - every 4-6 months; combined with rehabilitation therapy to improve function and delay surgery
- Phenol / ethyl alcohol injections
Step 3 - Intrathecal Baclofen (ITB) pump:
- For inadequate response to oral agents or limiting side effects (sedation, weakness)
- Delivers baclofen directly to CSF at a fraction of oral dose - bypasses blood-brain barrier
- Reversible; pump requires surgical replacement every 5-7 years
- Catheter-related complications more common in children
Step 4 - Neurosurgical:
- Selective Dorsal Rhizotomy (SDR): Cuts selected dorsal sensory rootlets in lumbar region; effective for spastic diplegia; not useful for dystonia
- Deep brain stimulation (DBS): Emerging option for dystonic CP
Step 5 - Orthopaedic surgery:
| Procedure | Goal |
|---|---|
| Muscle-tendon lengthening | Restore joint range (reduces spasticity-driven contracture) |
| Tendon transfer | Rebalance muscle forces |
| Joint release / bony osteotomy | Correct fixed deformity |
| Hip relocation | For subluxation in quadriplegia |
| Spinal fusion | For scoliosis |
| Leg equalisation | Correct limb length discrepancy |
Rehabilitation
- Physiotherapy - cornerstone from early infancy; prevents contractures, improves strength and function
- Occupational therapy - upper limb function, activities of daily living, adaptive equipment
- Speech therapy - communication, augmentative devices, feeding
- Orthoses (AFOs, splints) - prevent contractures, improve gait mechanics
- Aquatic therapy / hippotherapy - evidence supports motor function benefits
Other
- Anticonvulsants for epilepsy
- Manage cognitive, visual, hearing, and behavioural comorbidities with appropriate specialists
- Nutritional support (PEG feeding in severe dysphagia)
Prognosis
- CP is a lifelong condition; the brain lesion is static but functional ability can improve substantially with therapy
- Secondary musculoskeletal complications (contractures, scoliosis, hip dislocation) worsen over time without active management
- Ambulatory prognosis:
- Spastic diplegia: majority become ambulatory
- Spastic hemiplegia: almost all walk
- Spastic quadriplegia / TBI: many do not achieve independent ambulation
- Cognitive prognosis: Intelligence may be fully normal, especially in spastic diplegia from prematurity and in dyskinetic CP
Sources: Bradley & Daroff's Neurology in Clinical Practice; Creasy & Resnik's Maternal-Fetal Medicine; Goldman-Cecil Medicine; Bailey & Love's Short Practice of Surgery (28th ed.); Campbell's Operative Orthopaedics (15th ed. 2026)
This is a shared conversation. Sign in to Orris to start your own chat.