Nephritic syndrome
Reading File
search_medical_text
nephritic syndrome etiology pathophysiology classification
search_medical_text
nephritic syndrome clinical features diagnosis management treatment
search_medical_image
nephritic syndrome glomerulonephritis histology pathology
GradeResponse
GradeResponse
GradeResponse
search_medical_text
glomerulonephritis post-streptococcal IgA nephropathy RPGN anti-GBM ANCA
Here is a comprehensive overview of nephritic syndrome:
Nephritic Syndrome
Definition
Nephritic syndrome is a clinical constellation resulting from glomerular inflammation that causes disruption of the capillary wall, leading to hematuria, proteinuria, oliguria, hypertension, and varying degrees of renal impairment.
Core Features (The "Nephritic Pentad")
| Feature | Mechanism |
|---|---|
| Hematuria (macro or microscopic) | Disrupted GBM allows RBC passage |
| Proteinuria (usually < 3.5 g/day) | Inflammatory damage to filtration barrier |
| Oliguria | Reduced GFR from inflammation |
| Hypertension | Salt/water retention; ↑ RAAS |
| Azotemia | Impaired glomerular filtration |
The nephritic urinalysis is hallmark: hematuria, RBC casts, granular casts, WBC casts, and mixed proteinuria. RBC casts are pathognomonic for glomerulonephritis. (Harrison's, p. 8381)
Pathophysiology
Glomerular inflammation involves:
- Immune complex deposition (in situ or circulating) → complement activation → C3a/C5a recruitment of PMNs
- Endocapillary hypercellularity → obliteration of capillary lumens → ↓ GFR
- Crescent formation (in severe disease) → parietal epithelial cell proliferation + macrophage infiltration in Bowman's space → rapidly progressive GN (RPGN)
- Salt/water retention → hypertension and edema (less dramatic than nephrotic)
Causes and Classification
By Pattern of Injury
| Category | Prototype Diseases |
|---|---|
| Diffuse proliferative GN | Post-infectious GN (PSGN), lupus nephritis class III/IV |
| Mesangial proliferative GN | IgA nephropathy (Berger's disease) |
| RPGN / Crescentic GN | Anti-GBM (Goodpasture), ANCA vasculitis, immune complex GN |
| Focal proliferative GN | IgA nephropathy, lupus class III |
By Immunofluorescence Pattern
| IF Pattern | Diagnosis |
|---|---|
| Granular ("starry sky") | PSGN, lupus, IgA nephropathy, MPGN |
| Linear | Anti-GBM disease (Goodpasture syndrome) |
| Pauci-immune (negative/scant) | ANCA-associated vasculitis (GPA, MPA, EGPA) |
Key Individual Conditions
1. Post-Streptococcal GN (PSGN)
- Trigger: Group A β-hemolytic Strep (pharyngitis or impetigo), 1–3 weeks prior
- Age: Children most common; can affect adults
- Labs: ↓ C3, normal C4; ASO/anti-DNase B positive
- Course: Self-limiting in children; adults may have persistent disease
2. IgA Nephropathy (Berger's Disease)
- Most common primary GN worldwide
- Gross hematuria concurrent with URI ("synpharyngitic hematuria")
- Mesangial IgA deposits on IF
- Prognosis variable; ~30% progress to ESRD over 20 years
3. Lupus Nephritis
- WHO/ISN Class III/IV presents as nephritic syndrome
- ↓ C3 and C4; anti-dsDNA, ANA positive
- "Full house" immunofluorescence (IgG, IgA, IgM, C3, C4, C1q)
4. RPGN / Crescentic GN
- Rapid loss of renal function over days–weeks
-
50% crescents on biopsy
- Three types:
- Type I: Anti-GBM (linear IF) — Goodpasture syndrome (pulmonary hemorrhage + nephritis)
- Type II: Immune complex (granular IF)
- Type III: Pauci-immune (ANCA+) — GPA, MPA
5. Membranoproliferative GN (MPGN)
- Can present with mixed nephritic-nephrotic features
- ↓ C3; "tram-track" GBM on EM
- Associated with hepatitis C, cryoglobulinemia, complement disorders
Histology
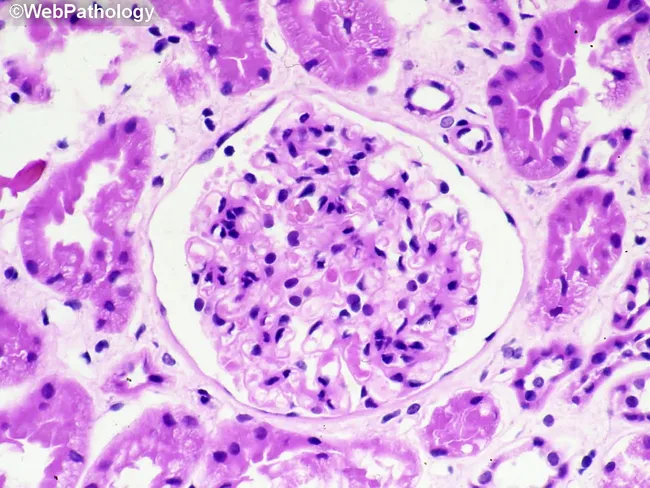
Renal biopsy showing intraglomerular hypercellularity, prominent cellular crescent in Bowman's space compressing the capillary tuft, and surrounding interstitial inflammation — consistent with RPGN/crescentic GN.
Diagnosis
Workup Algorithm
- Urinalysis + microscopy — RBC casts confirm glomerulonephritis
- CBC, BMP, LFTs — assess renal function, anemia
- 24-hour urine protein or spot PCR — quantify proteinuria
- Complement (C3, C4, CH50)
- Serologies:
- ANA, anti-dsDNA (lupus)
- ANCA (p-ANCA/MPO, c-ANCA/PR3)
- Anti-GBM antibodies
- ASO, anti-DNase B (PSGN)
- HBsAg, anti-HCV, cryoglobulins
- Serum protein electrophoresis
- Renal biopsy — required for definitive diagnosis in most cases (except classic PSGN)
Complement Levels as a Diagnostic Aid
| Condition | C3 | C4 |
|---|---|---|
| PSGN | ↓ | Normal |
| Lupus nephritis | ↓ | ↓ |
| MPGN | ↓ | ↓ or normal |
| Anti-GBM, ANCA | Normal | Normal |
| IgA nephropathy | Normal | Normal |
Management
General Principles
- Treat underlying cause (specific therapy below)
- BP control: ACE inhibitors/ARBs (also reduce proteinuria)
- Salt/fluid restriction: manage hypertension and edema
- Loop diuretics: for volume overload
- Dialysis: if severe AKI or uremia
Disease-Specific Treatment
| Disease | Treatment |
|---|---|
| PSGN | Supportive (antibiotics if active infection; steroids not routinely indicated) |
| IgA nephropathy | ACE/ARB; fish oil; steroids if proteinuria >1g/day; sparsentan (newer agent) |
| Lupus nephritis III/IV | Hydroxychloroquine + MMF or cyclophosphamide + steroids; belimumab, voclosporin (newer) |
| Anti-GBM disease | Urgent plasmapheresis + cyclophosphamide + steroids |
| ANCA vasculitis | Rituximab or cyclophosphamide + steroids; rituximab preferred for GPA/MPA |
| MPGN | Treat underlying cause (HCV: antivirals; complement: eculizumab) |
Nephritic vs. Nephrotic Syndrome (Quick Comparison)
| Feature | Nephritic | Nephrotic |
|---|---|---|
| Proteinuria | < 3.5 g/day | > 3.5 g/day |
| Hematuria | Prominent | Minimal |
| RBC casts | Yes | No |
| Edema | Mild–moderate | Severe ("pitting") |
| Hypertension | Common | Variable |
| Mechanism | Inflammation | Podocyte injury |
Prognosis
- PSGN in children: >95% full recovery
- IgA nephropathy: 20–40% ESRD over 20 years; Oxford MEST-C score guides prognosis
- Lupus nephritis class IV: renal survival ~80% at 10 years with treatment
- Anti-GBM disease: poor if dialysis-dependent at presentation; aggressive early treatment critical
- RPGN (ANCA): good renal recovery if treated promptly; relapse common
This is a shared conversation. Sign in to Orris to start your own chat.