i am doing 6 year general medicine and right now i am in 5 year 1st semester and my subject is allergology and topic is anaphylaxis can you please explain what is anaphylaxis and all about it
Reading File
search_medical_text
anaphylaxis definition pathophysiology mechanisms IgE mast cells
search_medical_text
anaphylaxis clinical features diagnosis treatment epinephrine management
search_medical_image
anaphylaxis pathophysiology mechanism diagram
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive breakdown of Anaphylaxis tailored for a 5th-year general medicine student in allergology:
Anaphylaxis — Complete Overview
1. Definition
Anaphylaxis is a severe, life-threatening, generalized or systemic hypersensitivity reaction that is rapid in onset and involves multiple organ systems simultaneously. It represents the most extreme end of the allergic reaction spectrum.
According to Harrison's Principles of Internal Medicine (21st Ed.), anaphylaxis results from the interaction of an allergen with IgE antibodies bound to mast cells and basophils, triggering massive release of inflammatory mediators.
2. Etiology — Common Triggers
| Category | Examples |
|---|---|
| Foods | Peanuts, tree nuts, shellfish, fish, milk, eggs, wheat |
| Drugs/Medications | Penicillin/antibiotics, NSAIDs, aspirin, contrast media, opioids |
| Insect venom | Bee sting, wasp, yellow jacket, fire ants |
| Latex | Surgical gloves, catheters |
| Exercise-induced | Exercise alone or food + exercise |
| Idiopathic | No identifiable trigger (~30% of cases) |
| Blood products | Transfusions, IV immunoglobulin |
3. Pathophysiology
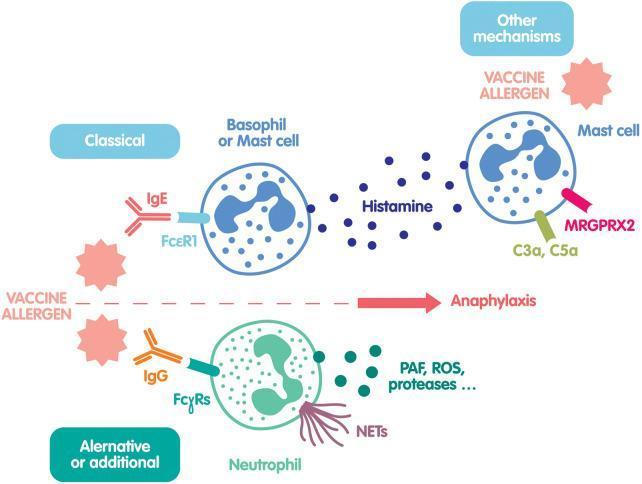
3.1 IgE-Mediated (Classical / Type I Hypersensitivity) — Most Common
This is a two-step process:
Step 1 — Sensitization (first exposure):
- Allergen enters the body → processed by antigen-presenting cells (APCs)
- Th2 helper T cells are activated → secrete IL-4, IL-5, IL-6, IL-10, IL-13
- B cells are driven to produce allergen-specific IgE antibodies
- IgE antibodies bind to high-affinity FcεRI receptors on mast cells (tissue) and basophils (blood) → the cell is now "armed"
- No symptoms occur at this stage
Step 2 — Re-exposure (elicitation):
- Allergen re-enters → cross-links two or more IgE molecules bound to FcεRI
- This cross-linking triggers mast cell and basophil degranulation
- Massive release of inflammatory mediators within minutes
(Harrison's, p. 9830)
3.2 Non-IgE Mediated Mechanisms
| Mechanism | Details |
|---|---|
| Complement activation | C3a and C5a ("anaphylatoxins") directly activate mast cells via C3a/C5a receptors |
| Direct mast cell activation | Via MRGPRX2 receptor — triggered by drugs like opioids, vancomycin, fluoroquinolones, muscle relaxants |
| IgG-mediated (neutrophil pathway) | Allergen + IgG → FcγRs on neutrophils → release PAF, ROS, proteases |
3.3 Mediators Released
| Type | Mediator | Effect |
|---|---|---|
| Preformed (granules) | Histamine | Vasodilation, increased vascular permeability, bronchoconstriction, pruritus |
| Tryptase | Marker of mast cell activation | |
| Heparin | Anticoagulation | |
| Newly synthesized (lipid) | Prostaglandin D2 | Bronchoconstriction, vasodilation |
| Leukotrienes (LTC4, LTD4) | Potent bronchoconstriction, mucus secretion | |
| Platelet-activating factor (PAF) | Severe bronchoconstriction, hypotension | |
| Cytokines | TNF-α, IL-4, IL-13 | Inflammation, late-phase reaction |
4. Clinical Features — "SASH" Organ Systems
Symptoms appear within seconds to 30 minutes of exposure (rarely up to 1–2 hours)
| System | Signs & Symptoms |
|---|---|
| Skin (most common ~90%) | Urticaria (hives), angioedema, flushing, pruritus |
| Respiratory (~70%) | Bronchospasm (wheeze, dyspnea), stridor (laryngeal edema), rhinorrhea, hoarseness |
| Cardiovascular (~45%) | Hypotension, tachycardia, arrhythmia, cardiovascular collapse, "empty ventricle syndrome" |
| Gastrointestinal (~45%) | Nausea, vomiting, diarrhea, abdominal cramping |
| Neurological | Anxiety, dizziness, confusion, syncope, loss of consciousness |
Key exam point: Skin manifestations are most common, but their absence does not rule out anaphylaxis — in cardiovascular collapse or rapid progression, skin findings may be absent or appear after hypotension.
5. Biphasic Anaphylaxis
- A second wave of anaphylactic symptoms occurs 1–72 hours after the initial reaction (usually 8–12 hours)
- Occurs in ~5–20% of cases
- Mechanism: Late-phase mediators (leukotrienes, cytokines)
- Reason for observation period of at least 4–8 hours after initial treatment
6. Diagnosis
Anaphylaxis is a clinical diagnosis. There is no single confirmatory test.
Diagnostic Criteria (WAO/NIAID-FAAN Guidelines)
Anaphylaxis is highly likely when ANY ONE of the following 3 criteria is met:
Criterion 1: Acute onset of illness with involvement of skin/mucosa + at least one of:
- Respiratory compromise
- Reduced BP or end-organ dysfunction
Criterion 2: Two or more of the following occurring rapidly after exposure to a likely allergen:
- Skin/mucosal symptoms
- Respiratory compromise
- Reduced BP or end-organ symptoms
- Persistent GI symptoms
Criterion 3: Reduced BP after exposure to a known allergen for that patient
Supportive Labs (not required for diagnosis but useful)
| Test | Significance |
|---|---|
| Serum Tryptase | Elevated >11.4 ng/mL; best drawn 1–3 hrs after reaction; confirms mast cell activation |
| Plasma/urine histamine | Elevated early (peaks at 5–10 min, normalizes in 30–60 min) |
| ABG | Hypoxia in severe respiratory compromise |
| ECG | Tachyarrhythmias, ischemia |
7. Treatment
Step-by-Step Emergency Management
"Early recognition + epinephrine = survival" (Harrison's, p. 9927)
Step 1 — Immediate (First 60 seconds)
- Call for help / activate emergency response
- Remove the trigger if possible (e.g., stop IV drug infusion)
- Position the patient: Supine with legs elevated (improves venous return)
- If unconscious / vomiting: recovery position
- If respiratory distress: semi-recumbent
- ⚠️ Avoid upright posture — risks "empty ventricle syndrome" from sudden hypotension + epinephrine's chronotropic effect
Step 2 — Epinephrine (Drug of FIRST CHOICE)
| Route | Dose | Details |
|---|---|---|
| IM (preferred) | 0.3–0.5 mL of 1:1000 (1 mg/mL) = 0.3–0.5 mg | Anterolateral thigh (vastus lateralis); may repeat every 5–20 min |
| IV | 0.1 mg (1:10,000 solution) diluted, slow push | Only in cardiac arrest or refractory cases — risk of arrhythmia |
| Auto-injector (EpiPen) | 0.3 mg adult; 0.15 mg child | For pre-hospital use / self-administration |
⚠️ Failure to give epinephrine within the first 20 minutes of symptoms is a significant risk factor for fatal outcomes (Harrison's, p. 9927)
Why epinephrine?
- α1 effect: Vasoconstriction → reverses hypotension and angioedema
- β1 effect: Increases heart rate and cardiac contractility
- β2 effect: Bronchodilation → reverses bronchospasm
- Inhibits further mediator release from mast cells
Step 3 — Airway, Breathing, Circulation (ABC)
- Supplemental O₂ (high flow, 8–10 L/min via face mask)
- IV access — large bore cannula × 2
- IV fluids — Normal saline 1–2 L rapidly for hypotension
- Prepare for intubation or surgical airway if laryngeal edema progresses
Step 4 — Adjunctive Therapy (Secondary agents — NOT first-line)
| Drug | Dose | Role |
|---|---|---|
| H1 antihistamine (diphenhydramine) | 25–50 mg IV/IM | Relieves urticaria, pruritus — does NOT treat hypotension or bronchospasm |
| H2 antihistamine (ranitidine/famotidine) | 50 mg IV | Adjunct for skin symptoms |
| Corticosteroids (hydrocortisone / methylprednisolone) | 100–200 mg IV | Prevent/reduce biphasic reaction (onset delayed 4–6 hrs; NOT for acute management) |
| Bronchodilator (salbutamol/albuterol) | 2.5 mg nebulized | For persistent bronchospasm |
| Glucagon | 1–2 mg IV bolus | For patients on beta-blockers (reverses epinephrine resistance) |
8. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Vasovagal syncope | Bradycardia (not tachycardia), pallor, no urticaria/angioedema, resolves with supine position |
| Angioedema (hereditary/HAE) | No urticaria, no IgE mechanism, C1 esterase inhibitor deficiency, family history |
| Panic attack | Normal BP, no urticaria/angioedema, tachycardia from anxiety |
| Carcinoid syndrome | Flushing, diarrhea — no urticaria, elevated 5-HIAA |
| Asthma exacerbation | Respiratory only, no skin or cardiovascular features |
| Septic shock | Slower onset, fever, source of infection |
9. Special Populations & Considerations
| Scenario | Key Point |
|---|---|
| Beta-blocker patients | Epinephrine is less effective → use glucagon 1–2 mg IV |
| Pregnant women | Epinephrine still first-line (risk of anaphylaxis > risk to fetus); position in left lateral decubitus |
| Children | IM epinephrine 0.01 mg/kg (max 0.3 mg); EpiPen Jr. for <25 kg |
| Exercise-induced anaphylaxis | Avoid trigger food 4–6 hrs before exercise; carry epinephrine auto-injector |
10. Prevention & Long-term Management
- Allergen identification: Skin prick test, specific IgE (RAST), oral food challenge (controlled setting)
- Avoidance: Educate patient on strict allergen avoidance
- Prescription of epinephrine auto-injector (EpiPen): Every patient with a history of anaphylaxis should carry two
- MedicAlert bracelet
- Allergen immunotherapy (desensitization): Available for venom (bee/wasp) and some foods — reduces severity of future reactions
- Anti-IgE therapy (Omalizumab): Used in refractory/idiopathic cases
11. Grading of Anaphylaxis Severity (Ring & Messmer Scale)
| Grade | Features |
|---|---|
| I | Skin/mucosal only — urticaria, flushing, angioedema |
| II | Systemic mild — skin + hypotension/tachycardia + mild bronchospasm/GI |
| III | Systemic severe — life-threatening bronchospasm or cardiovascular collapse |
| IV | Cardiac arrest, respiratory arrest |
12. Key Exam Points to Remember
- Epinephrine IM is ALWAYS first-line — antihistamines and steroids are adjuncts, never first-line
- IM route preferred over IV (safer, faster absorption from vastus lateralis)
- Tryptase is the best lab marker to confirm anaphylaxis retrospectively
- Skin symptoms absent does not rule out anaphylaxis
- Biphasic reaction occurs in 5–20% — always observe for ≥4–8 hours
- Beta-blocker patients need glucagon
- Upright posture is dangerous in hypotensive anaphylaxis ("empty ventricle syndrome")
- Omalizumab (anti-IgE) is used in chronic spontaneous urticaria and idiopathic anaphylaxis
This covers anaphylaxis from first principles to clinical management at the level expected of a 5th-year medical student in allergology. Good luck with your studies!
now write on ' surgical disease '
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.