PTA audiogram everything on it to learn understand memorize
Reading File
Finding Sources
Finding Sources
Searching the Web
PTA pure tone audiogram complete guide symbols interpretation hearing loss types
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading Web Page
https://geekymedics.com/audiogram-interpretation
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have everything needed for a complete, thorough guide. Let me compile the full answer.
The Pure Tone Audiogram (PTA) - Complete Master Guide
1. WHAT IS A PTA AUDIOGRAM?
A Pure Tone Audiogram is a graph that maps a patient's hearing thresholds - the softest sound level they can detect at each frequency - tested individually for each ear. It is the cornerstone of audiological assessment.
- It tells you how much hearing loss is present (degree)
- It tells you what type of hearing loss (conductive, sensorineural, mixed)
- Certain disease patterns produce characteristic audiogram "shapes"
2. THE GRAPH ITSELF
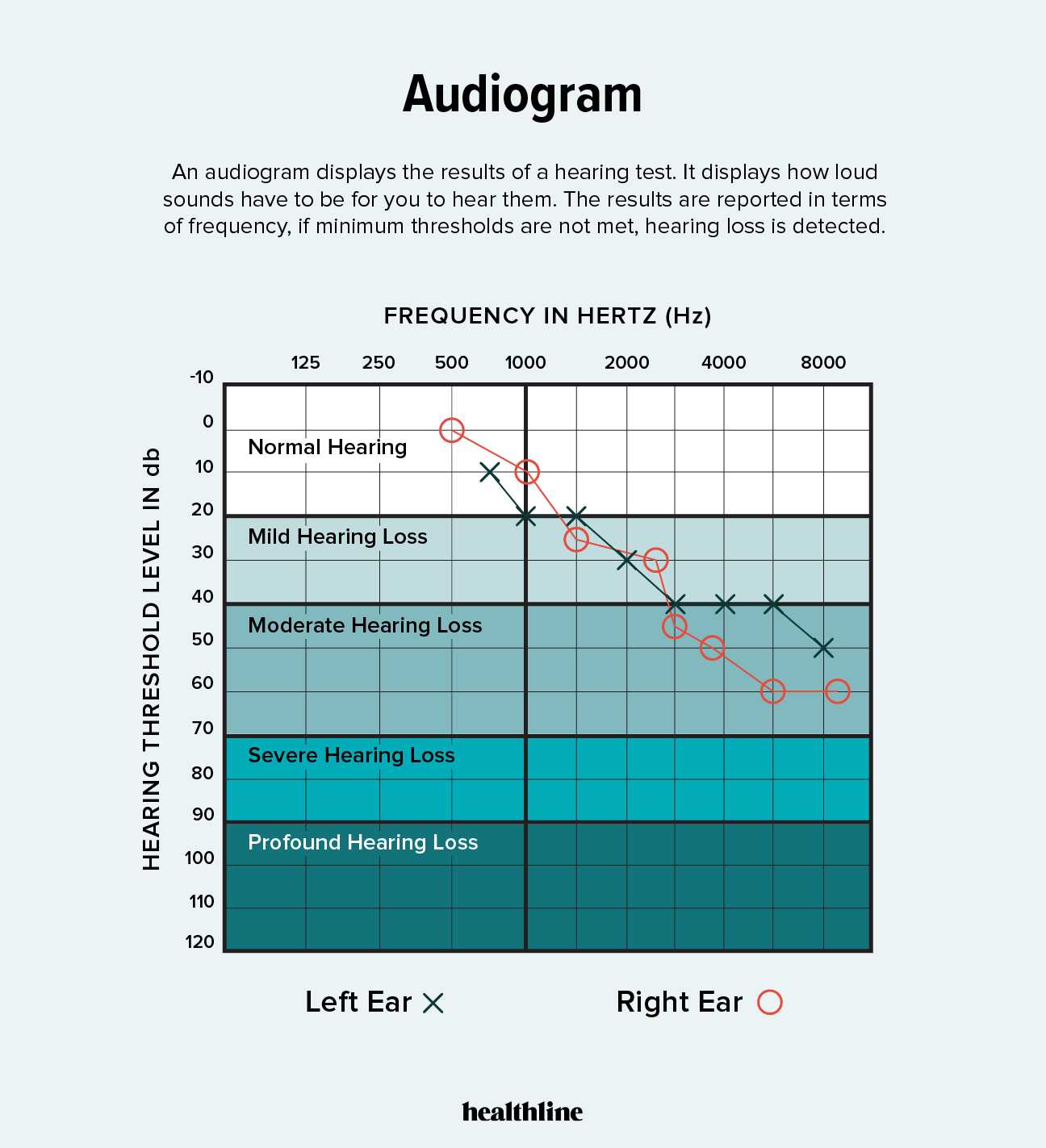
X-axis: FREQUENCY (Hz) - Pitch
- Runs left to right: low pitch to high pitch
- Logarithmic scale (each octave takes equal space)
- Standard frequencies tested: 250, 500, 1000, 2000, 4000, 8000 Hz
- Inter-octave frequencies (750, 1500, 3000, 6000 Hz) added when:
- Threshold difference of ≥25 dB between adjacent octaves
- Ototoxicity monitoring
- Hearing aid fitting
- Speech frequencies: 500-4000 Hz (this is the clinically critical zone)
- 250 Hz ≈ middle C on a piano
Y-axis: HEARING LEVEL (dB HL) - Loudness
- Runs top to bottom (0 at top, 120 at bottom) - this is the opposite of a normal graph
- 0 dB HL = average threshold of a normal young adult (not silence)
- Negative numbers (-10 dB) mean hearing is better than average
- The lower the threshold mark, the worse the hearing (more loss = lower on the graph)
- Units are dB HL (hearing level) - already corrected for the ear's frequency sensitivity. Different from dB SPL.
Memory trick: Think of it as a cliff - the more the line falls down the graph, the more hearing has "fallen"
3. AUDIOGRAM SYMBOLS (ASHA Standard)
This is the ASHA official symbol key:
Full Symbol Table
| Symbol | Ear | Modality | Masking? |
|---|---|---|---|
| O | Right | Air conduction (earphones) | Unmasked |
| △ | Right | Air conduction (earphones) | Masked |
| X | Left | Air conduction (earphones) | Unmasked |
| □ | Left | Air conduction (earphones) | Masked |
| < | Right | Bone conduction (mastoid) | Unmasked |
| [ | Right | Bone conduction (mastoid) | Masked |
| > | Left | Bone conduction (mastoid) | Unmasked |
| ] | Left | Bone conduction (mastoid) | Masked |
| ↓ | Forehead | Bone conduction (forehead) | Unmasked |
| S | Either | Sound field (speakers) | - |
| NR | - | No response | - |
Colour convention
- Red = Right ear
- Blue = Left ear
Line convention
- AC thresholds joined by solid lines
- BC thresholds joined by dashed lines
Memory trick for O and X: "O" is a circle, like a zero = Right (right = zero is the default). "X" for left ("cross" = left).
Memory trick for BC arrows: The arrow points toward the test ear.
< points toward right, > points toward left.4. WHAT IS MEASURED: AIR vs BONE CONDUCTION
Air Conduction (AC)
Sound travels: ear canal → tympanic membrane → ossicles → cochlea → auditory nerve → brain
Tests the entire hearing pathway. Uses earphones (supra-aural or insert).
Bone Conduction (BC)
A bone oscillator is placed on the mastoid process (or forehead). Sound bypasses the outer and middle ear and vibrates the skull directly → cochlea → nerve.
Tests inner ear function only (bypasses outer and middle ear).
Why this matters clinically
| Finding | AC | BC | Diagnosis |
|---|---|---|---|
| Both normal (≤20 dB HL) | Normal | Normal | Normal hearing |
| AC elevated, BC normal | Abnormal | Normal | Conductive loss |
| Both equally elevated | Abnormal | Abnormal | Sensorineural loss |
| AC elevated, BC elevated but less | Both abnormal | Different | Mixed loss |
5. THE AIR-BONE GAP (ABG)
The ABG is the difference between AC threshold and BC threshold at the same frequency.
- Normal: ABG = 0 (both lines overlap)
- Significant ABG: ≥10 dB (StatPearls says >15 dB HL)
- ABG = sign of conductive pathology (outer or middle ear problem)
Key concept: Bone conduction is a "window" into the cochlea. If BC is normal but AC is poor, the cochlea is fine - the problem is in the transmission apparatus (outer/middle ear).
6. MASKING
What it is: Introducing narrow-band noise into the non-test ear to prevent it from "cross-hearing" the signal meant for the test ear.
Why needed: Sound presented to one ear can cross the skull (via bone) and be detected by the other ear. This is called crossover.
Interaural attenuation (IA): The reduction in sound as it crosses the skull.
- Supra-aural headphones AC: 40-65 dB IA (crossover risk at ≥40 dB HL)
- Insert earphones AC: 70-90 dB IA (much less crossover risk)
- Bone conduction: 0-10 dB IA (crossover happens almost immediately - always consider masking)
When to mask (two rules):
- AC: Mask the non-test ear when the AC level in the test ear exceeds the BC threshold of the non-test ear by 40 dB (supra-aural) or 55 dB (insert)
- BC: Mask the non-test ear whenever you test bone conduction (because IA for BC ≈ 0-10 dB)
Masked symbols are shown with different symbols (△ for right AC masked; □ for left AC masked; [ and ] for bone conduction masked).
7. DEGREE OF HEARING LOSS
| Degree | dB HL Range | Functional Impact |
|---|---|---|
| Normal | ≤20 dB HL | Hears all speech clearly |
| Mild | 21-40 dB | Difficulty in noisy environments; may miss soft speech |
| Moderate | 41-70 dB | Requires hearing aid for normal conversation; group conversations difficult |
| Severe | 71-95 dB | Loud sounds and shouted speech may be heard; hearing aid usually needed |
| Profound | ≥96 dB | Very little hearing; cochlear implant may be considered |
(BSA 2011 classification, used in Scott-Brown's. ASHA and WHO use slightly different cutoffs - mild starts at 26 dB HL in some systems; normal ≤15 dB HL in children)
8. PURE-TONE AVERAGE (PTA)
Definition: The arithmetic mean of air-conduction thresholds at 500, 1000, and 2000 Hz
Formula: PTA = (threshold at 500 Hz + 1000 Hz + 2000 Hz) ÷ 3
- Summarizes hearing in the key speech frequencies
- Used to classify degree of hearing loss
- Limitation: Does NOT reflect high-frequency hearing loss (e.g., early noise-induced or presbycusis affecting 4000-8000 Hz)
Some clinicians use a 4-frequency average (500, 1000, 2000, 4000 Hz) for more complete assessment.
9. AUDIOGRAM SHAPES (CONFIGURATIONS)
The shape of the audiogram curve gives diagnostic clues:
| Shape | Description | Common Causes |
|---|---|---|
| Flat | Same threshold across all frequencies | Conductive losses, hereditary SNHL |
| Sloping (ski-slope) | Worse in high frequencies | Presbycusis, noise-induced, acoustic neuroma |
| Rising | Worse in low frequencies | Meniere's disease (early) |
| Notch at 4000 Hz | Isolated dip at 4 kHz | Noise-induced hearing loss |
| Cookie bite (U-shape) | Mid-frequency loss | Hereditary hearing loss |
| Carhart's notch | BC dip at 2000 Hz | Otosclerosis |
10. THE THREE TYPES OF HEARING LOSS
A. Conductive Hearing Loss (CHL)
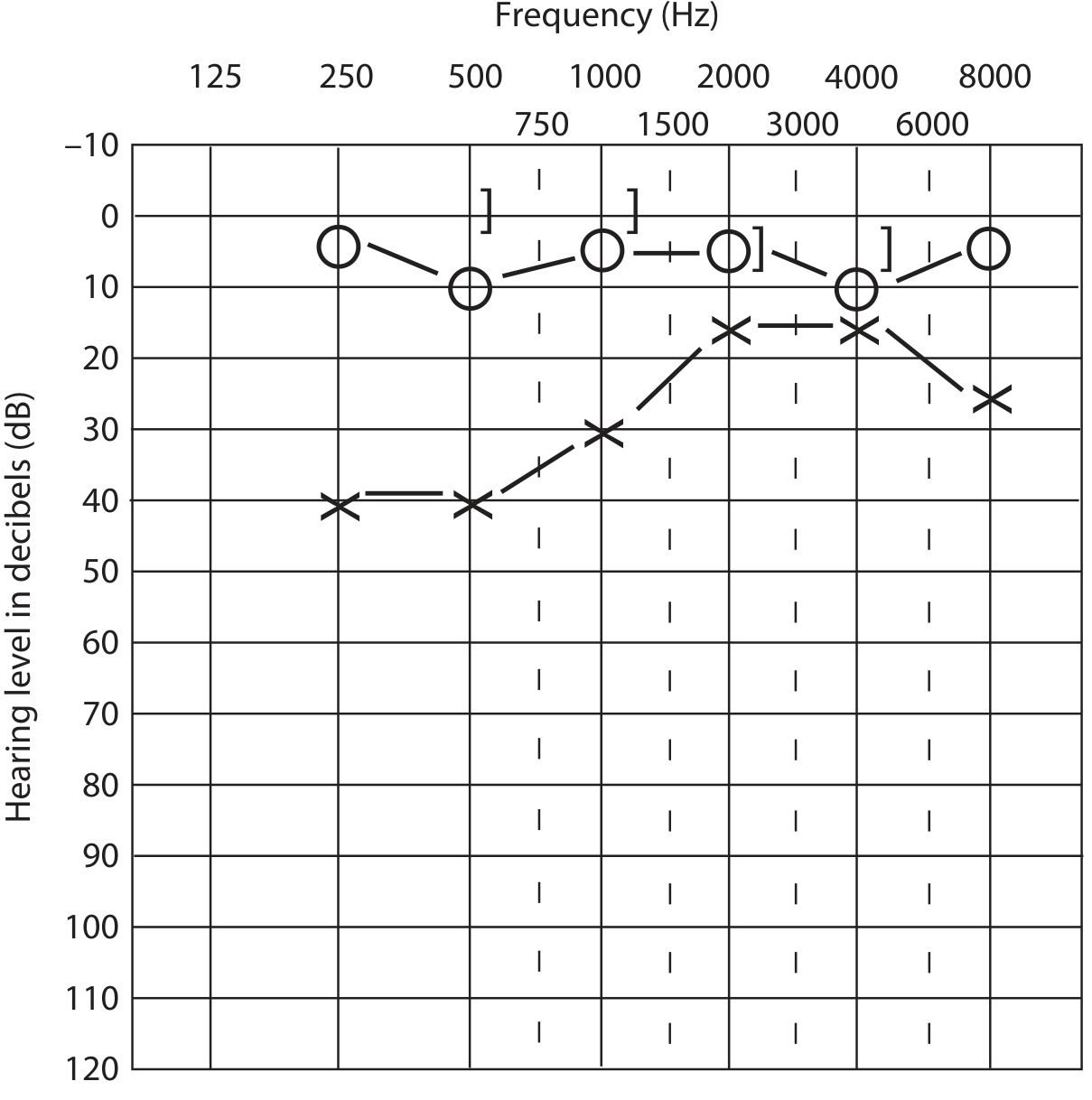
Figure: Left ear conductive loss - X symbols (AC) are significantly lower than the ] symbols (masked BC), which are near 0 dB. Note the large air-bone gap.
- AC abnormal, BC normal (≤20 dB HL)
- Air-bone gap present (≥10-15 dB)
- Problem in: outer ear or middle ear
Common causes:
- Cerumen impaction
- Otitis media with effusion ("glue ear")
- Tympanic membrane perforation
- Otosclerosis (stapes fixation)
- Ossicular chain disruption
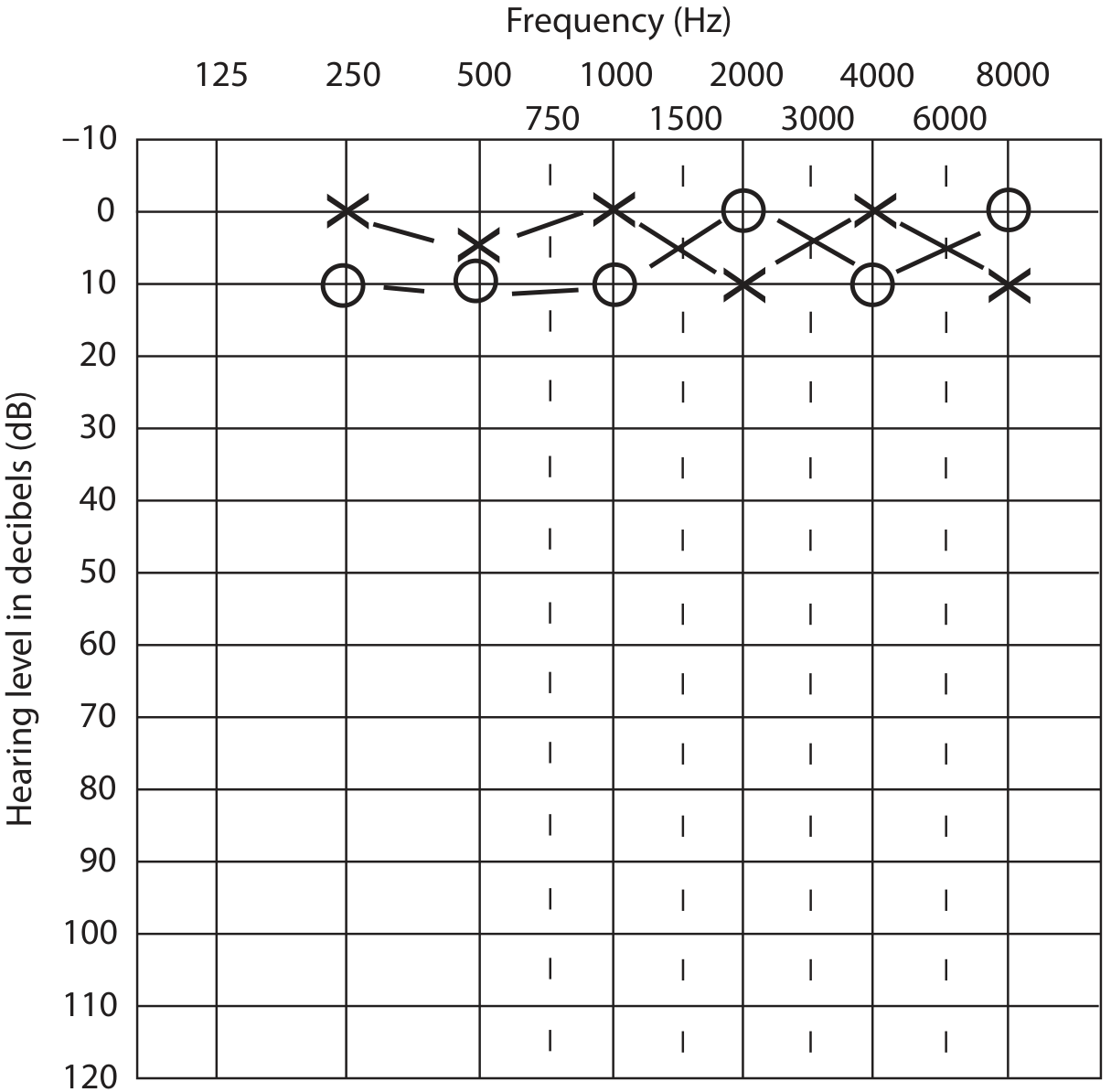
B. Sensorineural Hearing Loss (SNHL)
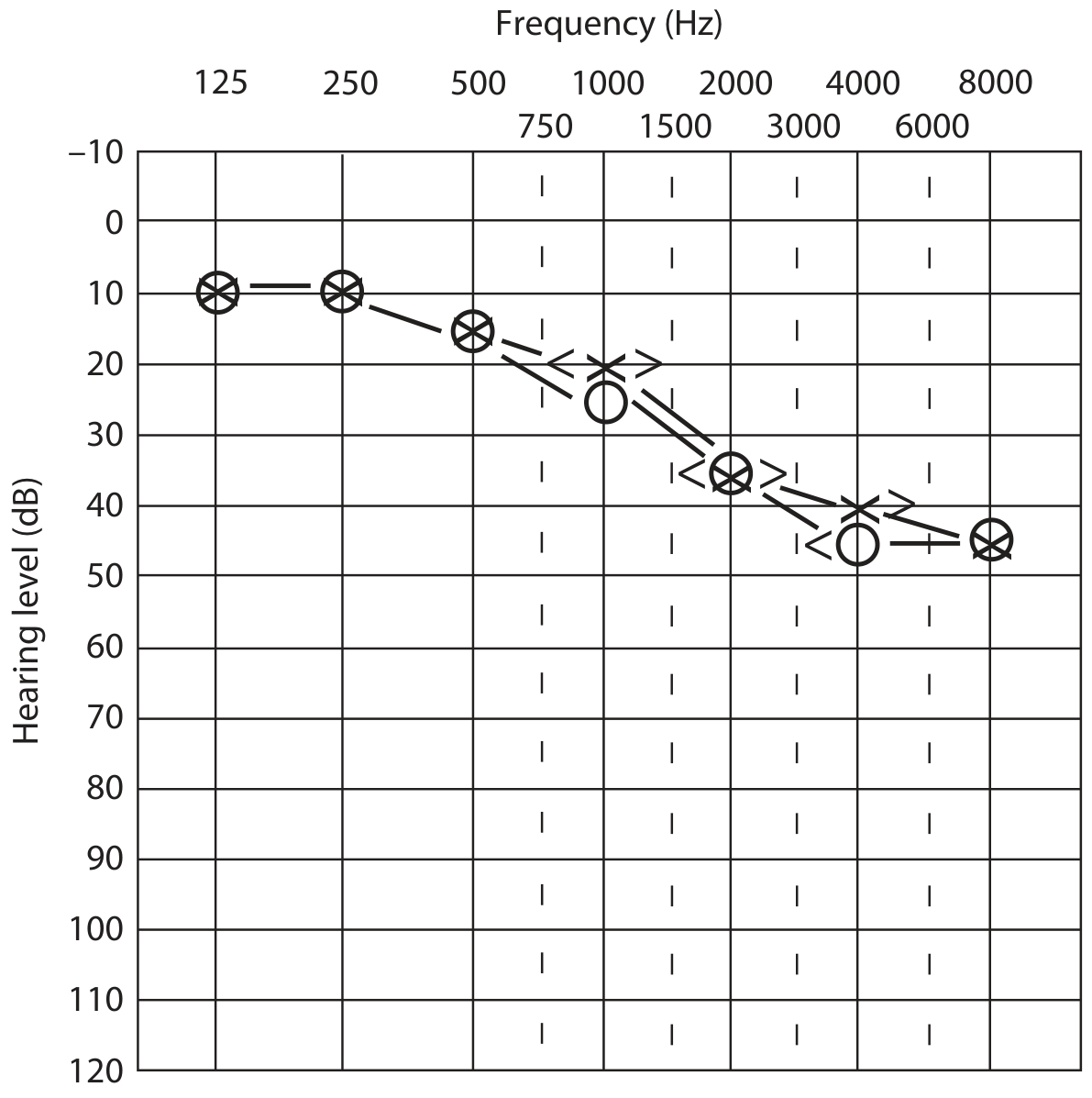
Figure: Bilateral SNHL with sloping configuration - O/X (AC) and </> (BC) lines fall together, no air-bone gap.
- Both AC and BC are equally abnormal
- No air-bone gap (lines overlap or gap <10 dB)
- Problem in: cochlea (sensory) or auditory nerve/CNS (neural)
Common causes:
- Presbycusis (age-related) - bilateral sloping high-frequency loss
- Noise-induced - 4 kHz notch
- Meniere's disease - low-frequency, fluctuating
- Acoustic neuroma (vestibular schwannoma) - unilateral
- Ototoxic drugs (aminoglycosides, cisplatin)
- Viral/genetic causes
C. Mixed Hearing Loss
- Both AC and BC abnormal
- Air-bone gap also present (both are impaired but BC is better than AC)
- Problem in: both outer/middle ear AND cochlea
Common causes: Chronic suppurative otitis media with cochlear damage, advanced otosclerosis, head trauma
11. NORMAL AUDIOGRAM
Normal hearing: All AC thresholds in adults ≤20 dB HL across all frequencies. In children, normal = ≤15 dB HL.
12. DISEASE-SPECIFIC AUDIOGRAM PATTERNS (HIGH-YIELD)
| Disease | Pattern to Know |
|---|---|
| Presbycusis | Bilateral, symmetrical, high-frequency sloping SNHL (worse at 4-8 kHz) |
| Noise-induced | 4 kHz notch (dip) in both ears; high-frequency SNHL; often with recovery at 8 kHz |
| Meniere's disease | Low-frequency SNHL (250-500 Hz); unilateral; fluctuating; "rising" configuration |
| Otosclerosis | CHL (flat/rising) + Carhart's notch: BC dip at 2000 Hz (mechanical resonance artifact) |
| Acoustic neuroma | Unilateral, asymmetric high-frequency SNHL |
| Sudden SNHL | Unilateral SNHL developing within 72h; urgent evaluation |
| Glue ear (OME) | Flat mild CHL ~25-40 dB, air-bone gap, BC normal |
| Ototoxicity | High-frequency bilateral SNHL progressing inward (starts 8 kHz, moves to 4, 2 kHz) |
13. THE AUDIOGRAM OF FAMILIAR SOUNDS ("Speech Banana")
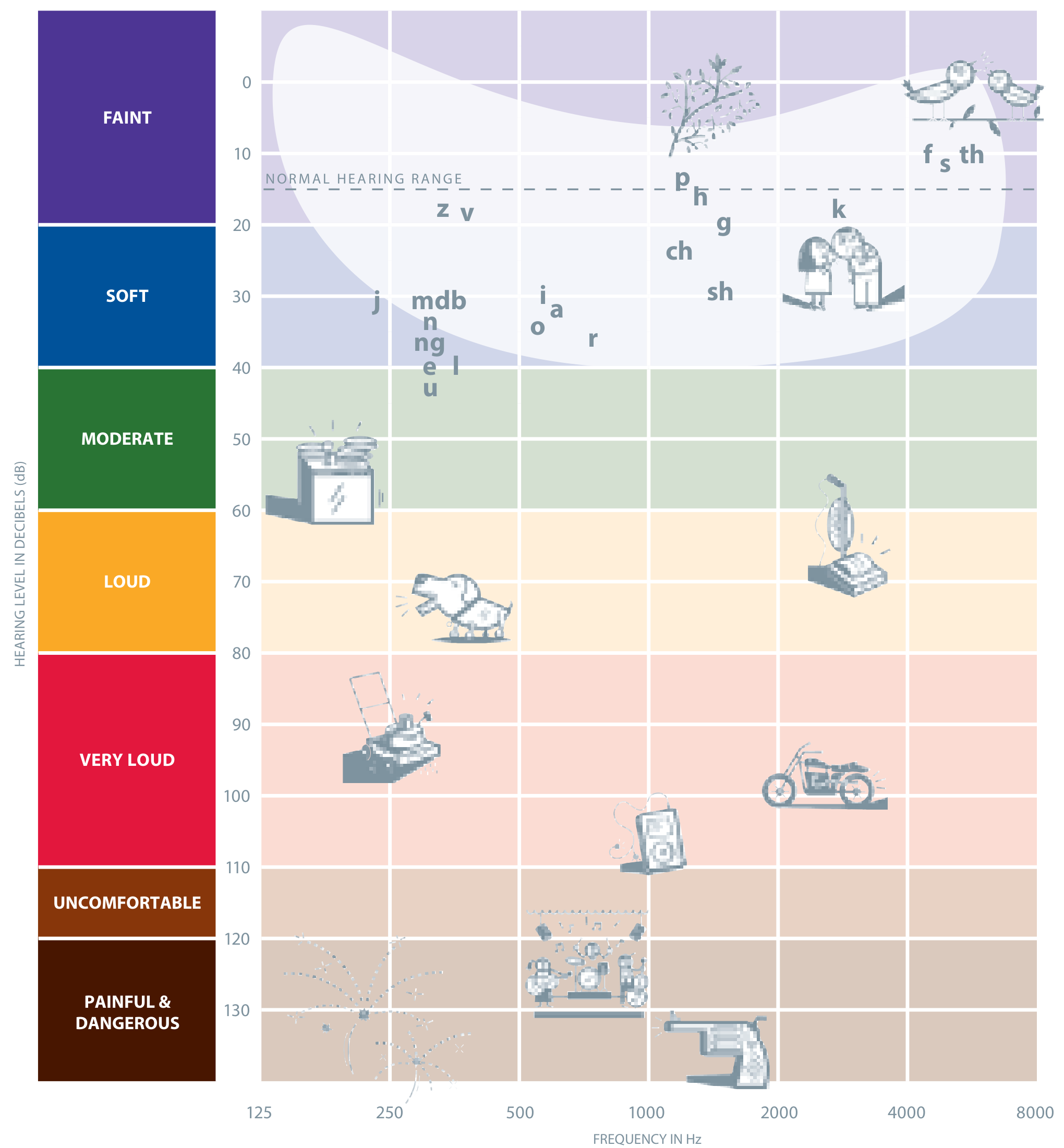
This chart overlays everyday sounds onto the audiogram grid:
- Vowels (a, e, o, u) fall in low frequencies (250-1000 Hz), moderate intensity (40-60 dB)
- Consonants (f, s, th) fall in high frequencies (2000-8000 Hz), low intensity (10-20 dB)
- The cluster of speech sounds forms a banana shape from lower-left to upper-right
- If a patient's thresholds fall below the speech banana, those sounds are inaudible to them
- This explains why high-frequency SNHL causes difficulty understanding consonants even when they can "hear" speech
14. WHAT THE AUDIOGRAM DOES NOT SHOW
An audiogram measures threshold sensitivity only. It does not directly assess:
- Speech discrimination/intelligibility in noise (needs speech audiometry)
- Central auditory processing
- Cochlear mechanics (needs OAEs - otoacoustic emissions)
- Neural synchrony (needs ABR - auditory brainstem response)
- Middle ear function (needs tympanometry)
- Uncomfortable loudness levels (needs loudness testing)
15. THE TEST PROCEDURE (How PTA is Performed)
- Patient sits in a sound-treated booth to eliminate ambient noise
- Otoscopic inspection first (check for cerumen, perforation, etc.)
- Earphones placed (supra-aural or insert)
- Tones presented using the Hughson-Westlake method:
- Start at 1000 Hz at a comfortable level
- Patient responds (button/hand raise) every time they hear a tone
- Decrease in 10 dB steps, increase in 5 dB steps
- Threshold = lowest level with ≥50% correct responses
- Order: typically 1000 → 2000 → 4000 → 8000 → 500 → 250 Hz; retest 1000 Hz for reliability
- Better ear tested first
- Bone conduction if AC ≥15 dB HL
- Masking applied as needed
16. QUICK INTERPRETATION PROTOCOL (Step-by-Step)
When you see an audiogram:
Step 1: Look at the AC thresholds - are they normal (≤20 dB HL)?
Step 2: Calculate the PTA (500 + 1000 + 2000 Hz ÷ 3) for each ear
Step 3: Compare AC to BC at each frequency - is there an air-bone gap (≥10 dB)?
Step 4: Classify:
- Normal BC + abnormal AC + ABG → Conductive
- Abnormal BC + abnormal AC + no ABG → Sensorineural
- Both abnormal + ABG present → Mixed
Step 5: Look at the shape - does it suggest a specific disease pattern?
Step 6: Check for symmetry - asymmetric SNHL requires further investigation (MRI for acoustic neuroma)
17. KEY NUMBERS TO MEMORIZE
| Number | Meaning |
|---|---|
| 0 dB HL | Average normal threshold |
| 20 dB HL | Upper limit of normal hearing (adults) |
| 15 dB HL | Upper limit of normal (children) |
| ≥10 dB | Significant air-bone gap |
| 40 dB | Crossover threshold for AC with supra-aural phones |
| 0-10 dB | Interaural attenuation for BC |
| 500-4000 Hz | Primary speech frequencies |
| 4000 Hz | Noise-induced hearing loss notch |
| 2000 Hz | Carhart's notch (otosclerosis) |
| PTA = 500+1000+2000 ÷ 3 | Pure-tone average formula |
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2 (Ch. 51); K.J. Lee's Essential Otolaryngology (Ch. 14); StatPearls - Audiogram Interpretation; Geeky Medics - Audiogram Interpretation; ASHA audiogram symbol guidelines (1990)
Tympanometry and stapedial reflex
Finding Sources
Finding Sources
Searching the Web
tympanometry types tympanogram interpretation stapedial reflex complete guide
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed. Let me compile the complete guide.
Tympanometry and the Stapedial (Acoustic) Reflex - Complete Master Guide
PART 1: TYMPANOMETRY
1. WHAT IS TYMPANOMETRY?
Tympanometry is an objective test that measures the mobility (compliance/admittance) of the tympanic membrane and middle ear system as a function of systematically varied air pressure in the sealed external ear canal.
- It does not test hearing - it tests middle ear mechanics
- It measures acoustic immittance (admittance = how easily sound energy enters the middle ear; impedance = opposition to sound flow - they are reciprocals)
- Results are displayed as a tympanogram - a graph of compliance vs pressure
- Performed with a tympanometer (probe inserted into the ear canal with an airtight seal)
Key concept: Maximum compliance occurs when the pressure in the ear canal equals the pressure in the middle ear space - this is the peak of the tympanogram.
2. THE TYMPANOGRAM GRAPH
X-axis: Air pressure in the ear canal - daPa (decapascals), swept from +200 to -400 daPa
Y-axis: Compliance (admittance) of the tympanic membrane - in mL (equivalent air volume) or millimho (mmho)
- Normal static compliance: 0.3-1.6 mL (adults)
- Normal peak pressure: -100 to +50 daPa (adults)
Additional measurements recorded:
- Peak compensated static admittance (height of the peak)
- Tympanometric peak pressure (TPP) - pressure at which peak occurs
- Tympanometric width (TW) / Gradient - width of the curve at half the peak height (normal ~60-150 daPa; widened in OME)
- Equivalent ear canal volume (ECV) - volume of air in front of the probe (normal 0.6-1.5 mL adults; 0.3-0.9 mL children)
Probe tone: Standard = 226 Hz. For infants <6 months: 1000 Hz probe tone (because the external canal is too compliant at 226 Hz in neonates, giving falsely normal results).
3. TYMPANOGRAM TYPES (JERGER CLASSIFICATION)
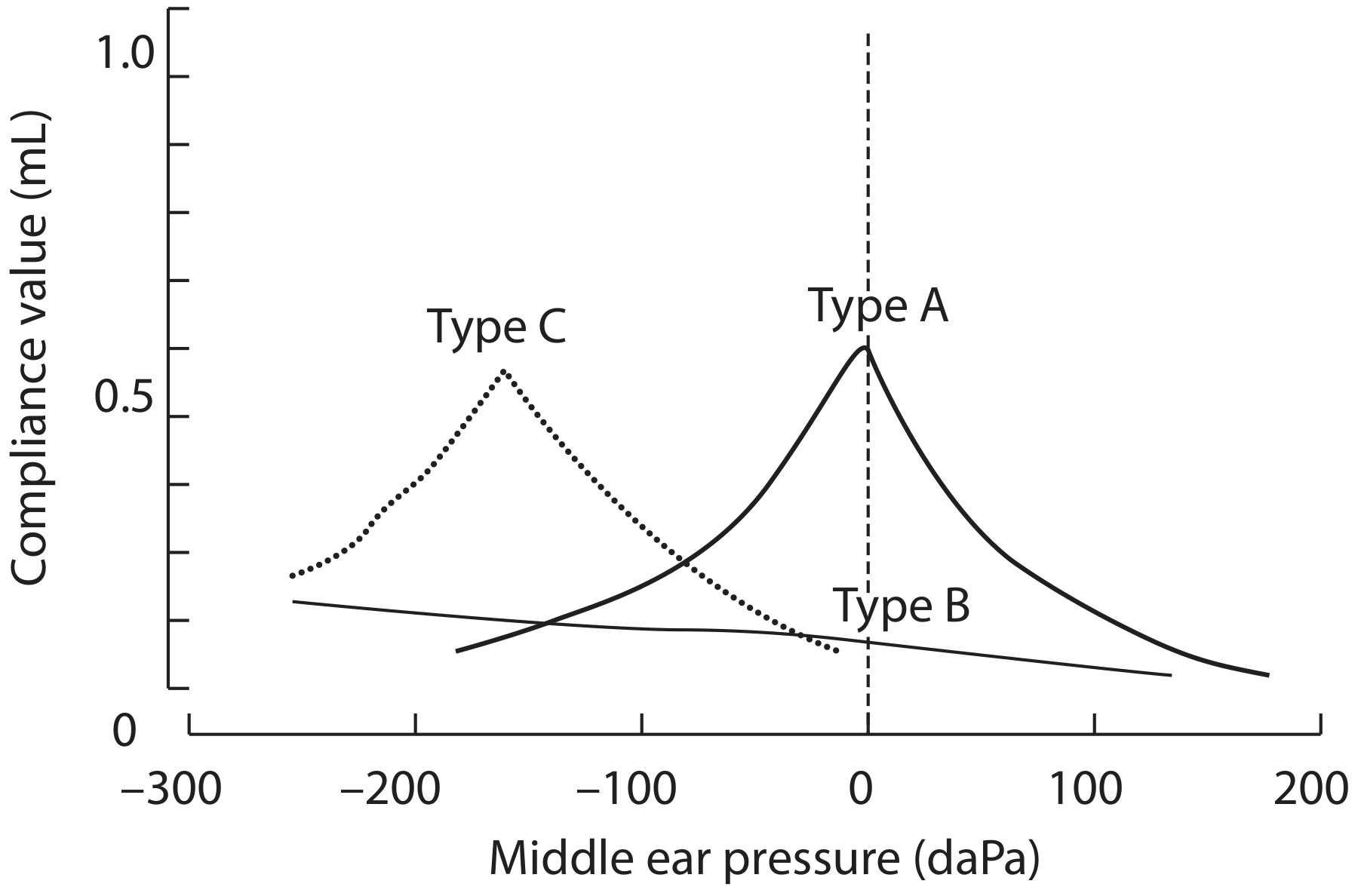
Type A: normal peak at ~0 daPa. Type B: flat line. Type C: peak shifted into negative pressure.
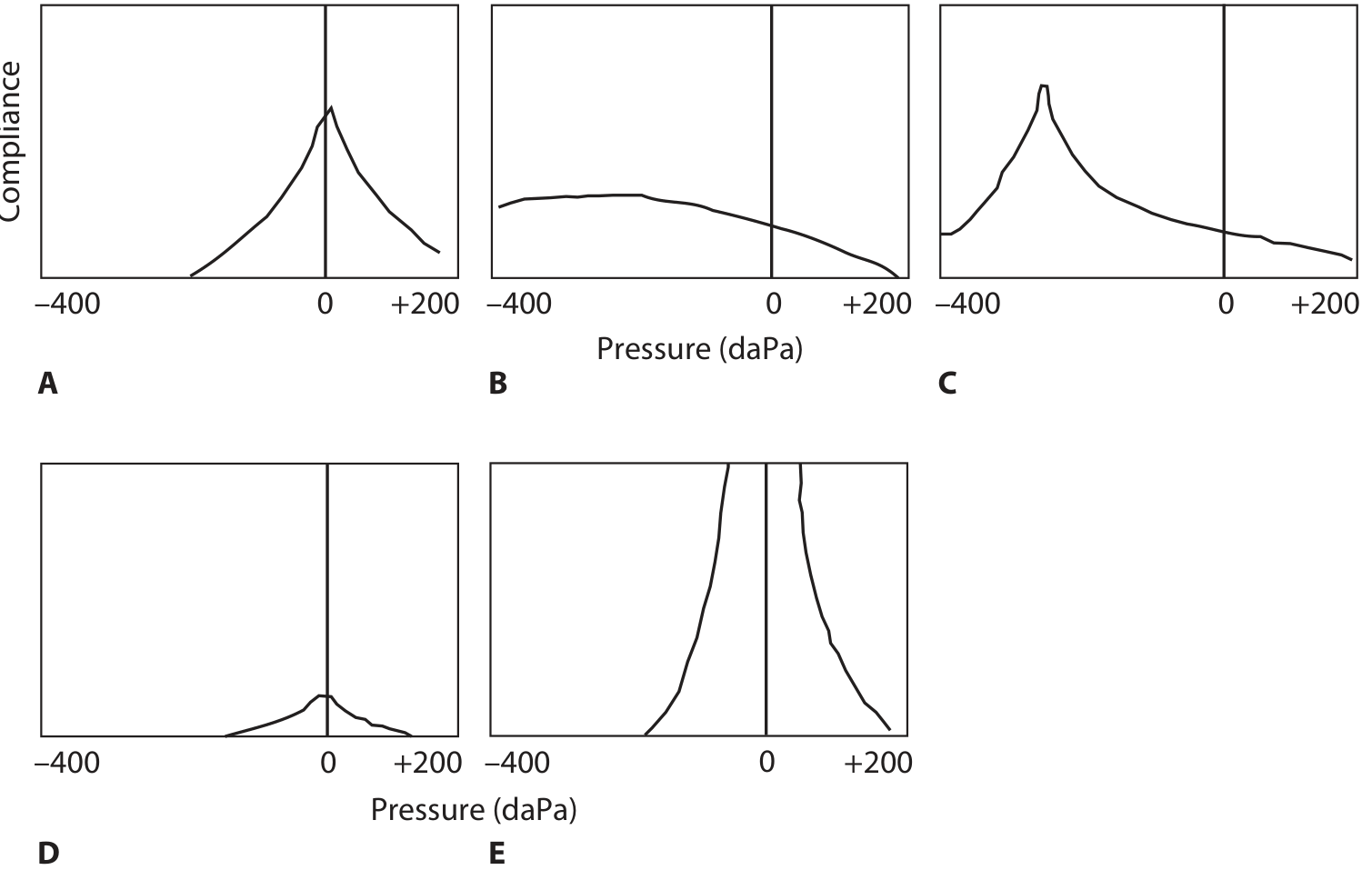
A = normal; B = flat; C = negative pressure; D (As) = shallow peak; E (Ad) = very high peak.
TYPE A - NORMAL
- Peak at 0 daPa (or close: -100 to +50 daPa in adults)
- Normal compliance height
- Indicates: Normal middle ear pressure and normal TM mobility
- Seen in: Normal hearing OR sensorineural hearing loss (inner ear problem, but middle ear is fine)
Memory: "A for Adequate"
TYPE As (A-shallow / A-stiff)
- Peak is at normal pressure but compliance is abnormally LOW (shallow peak)
- "s" = shallow/stiffened
- Indicates: Increased stiffness of the middle ear system
- Seen in:
- Otosclerosis (fixation of stapes footplate)
- Tympanosclerosis
- Scarred/thickened tympanic membrane
- Malleus fixation
Memory: "As = A-stiff"
TYPE Ad (A-deep / A-discontinuous)
- Peak is at normal pressure but compliance is abnormally HIGH (very tall, sharp peak)
- "d" = deep/discontinuous
- Indicates: Hypercompliant / flaccid middle ear
- Seen in:
- Ossicular chain discontinuity (e.g., traumatic disruption of incus)
- Flaccid/atrophic tympanic membrane (monomeric)
- Healed large perforation
- Note: In discontinuity there is often a severe conductive hearing loss, worse at high frequencies (unlike most CHL)
Memory: "Ad = A-dislocated (ossicular chain)"
TYPE B - FLAT
- No identifiable peak across the pressure sweep
- The curve is flat or gently rounded
- Now look at the ear canal volume (ECV) - this is the key discriminator:
| ECV | Interpretation |
|---|---|
| Normal (0.6-1.5 mL) | Middle ear effusion (OME / glue ear) - fluid dampens TM movement |
| Large (>2 mL) | TM perforation or patent tympanostomy (PE) tube - probe is measuring the middle ear + canal together |
| Very small (<0.3 mL) | Probe blocked (cerumen, against canal wall) - artefact |
Type B with normal ECV = OME until proven otherwise
Sensitivity of Type B for OME vs myringotomy: 56-73%, specificity 50-98% (Scott-Brown's)
Memory: "B for Blocked (by fluid)"
TYPE C - NEGATIVE PRESSURE
- Peak present but shifted to negative pressure (more negative than -100 daPa adults, -150 daPa children)
- Subtypes:
- C1: -100 to -199 daPa
- C2: -200 to -399 daPa (more significant)
- Indicates: Negative middle ear pressure - Eustachian tube dysfunction
- Seen in: Eustachian tube obstruction, early OME, after URI, retracted TM
- C2 + Type B combined has sensitivity 73-99% for OME
Memory: "C for Congested Eustachian tube"
SUMMARY TABLE
| Type | Peak | Compliance | ECV | Diagnosis |
|---|---|---|---|---|
| A | 0 daPa | Normal | Normal | Normal middle ear |
| As | 0 daPa | Low | Normal | Otosclerosis, TM scarring |
| Ad | 0 daPa | Very high | Normal | Ossicular discontinuity, flaccid TM |
| B | Absent | Flat | Normal | OME (glue ear) |
| B | Absent | Flat | Large | TM perforation / PE tube |
| B | Absent | Flat | Small | Probe blocked |
| C | Negative | Normal-low | Normal | ET dysfunction |
4. CLINICAL APPLICATIONS OF TYMPANOMETRY
- Diagnosing OME (otitis media with effusion) - key test alongside otoscopy
- Detecting TM perforation (large ECV)
- Checking PE tube patency (large ECV if patent)
- Screening for middle ear pathology in children
- Confirming conductive hearing loss cause
- Combined with otoscopy: When both agree (Type B + otoscopy = OME), sensitivity 98%; specificity 98%
5. LIMITATIONS
- Does NOT test hearing directly
- Unreliable in infants <7 months with standard 226 Hz probe (use 1000 Hz)
- Cannot be performed with TM perforation for standard immittance testing
- Does not distinguish all causes of Type B (need ECV to help)
PART 2: THE STAPEDIAL (ACOUSTIC) REFLEX
6. WHAT IS THE STAPEDIAL REFLEX?
When a loud sound (typically 70-100 dB above threshold) is heard, the stapedius muscle (in the middle ear, attached to the stapes) contracts bilaterally, stiffening the ossicular chain to protect the cochlea from damage.
This contraction decreases the compliance of the middle ear and this change can be detected by the tympanometer probe. This is the acoustic reflex (also called stapedial reflex or acoustic stapedial reflex).
What it tests: Integrity of the entire arc from cochlea → auditory nerve → brainstem → facial nerve → stapedius muscle
7. THE REFLEX ARC
The reflex occurs bilaterally no matter which ear is stimulated:
Ipsilateral Pathway (stimulus and recording in SAME ear)
- Cochlea (hair cells)
- CN VIII (auditory nerve)
- Ipsilateral ventral cochlear nucleus (VCN)
- Trapezoid body
- Ipsilateral facial motor nucleus (or medial superior olive)
- Ipsilateral CN VII (facial nerve)
- Ipsilateral stapedius muscle contracts
Contralateral Pathway (stimulus in ONE ear, recording in OTHER ear)
- Cochlea (hair cells)
- CN VIII (auditory nerve)
- Ipsilateral VCN
- Crosses to contralateral medial superior olive
- Contralateral facial motor nucleus
- Contralateral CN VII (facial nerve)
- Contralateral stapedius muscle contracts
Key teaching point: A sound in the RIGHT ear → reflexes in BOTH stapedius muscles. The reflex is always bilateral.
8. HOW IT IS TESTED
- Tympanometer set to hold TM at point of maximum compliance
- Pure tones or broadband noise presented at increasing intensities
- The reflex threshold = lowest level that produces a change in compliance
- Tested ipsilaterally (probe = recording ear also gets the sound) and contralaterally (probe records in one ear; sound in the other)
- Normal reflex threshold: 70-100 dB HL for pure tones
9. RECORDING ARRANGEMENT - UNDERSTANDING THE 4 COMBINATIONS
For each stimulus ear (Right or Left) and each recording ear (Right or Left):
| Stimulus Ear | Recording Ear | Pathway Type |
|---|---|---|
| Right | Right | Ipsilateral |
| Right | Left | Contralateral |
| Left | Left | Ipsilateral |
| Left | Right | Contralateral |
A full test battery = 4 reflex measurements.
10. CAUSES OF ABSENT OR ELEVATED ACOUSTIC REFLEX
The reflex is absent when any part of the arc is disrupted:
| Cause | Why |
|---|---|
| Conductive loss ≥10 dB in recording ear | Probe ear cannot detect the compliance change |
| Conductive loss ≥40 dB in stimulus ear | Sound not loud enough to reach threshold even at max output |
| SNHL >70 dB HL in stimulus ear | Cochlea cannot detect the loud tone |
| CN VIII (acoustic neuroma/vestibular schwannoma) | Neural lesion; reflex absent or decays |
| CN VII lesion proximal to stapedius branch | Facial nerve cannot activate stapedius |
| Brainstem lesion | Arc interrupted centrally |
| Multiple sclerosis | Demyelination of reflex arc |
| Ramsay Hunt syndrome | CN VII involvement |
11. PATTERNS OF REFLEX FINDINGS (LESION LOCALISATION)
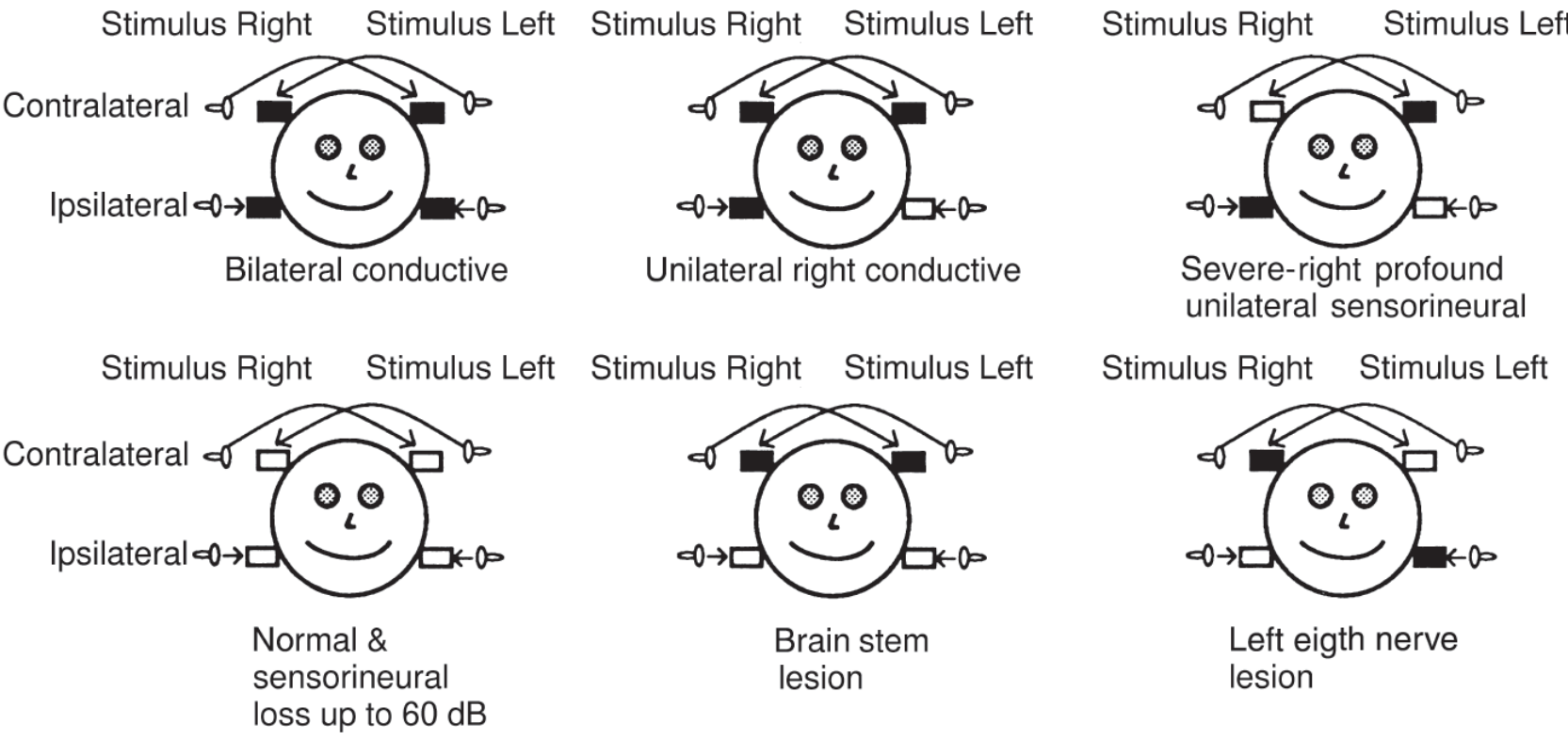
Key: Filled box = reflex present; Open box = reflex absent
| Pattern | Ipsi Right | Contra Right | Ipsi Left | Contra Left | Likely Lesion |
|---|---|---|---|---|---|
| Normal | ✓ | ✓ | ✓ | ✓ | Normal / SNHL ≤60 dB |
| Right CHL (probe side) | Absent | Absent | ✓ | Absent | Right middle ear - probe can't detect |
| Right CHL (stim side >40dB) | Absent | Absent | ✓ | ✓ | Right conductive (mild) |
| Right CN VIII | Absent | Absent | ✓ | ✓ | Right auditory nerve (no stimulus crosses) |
| Brainstem | ✓ | Absent | ✓ | Absent | Contralateral pathway interrupted bilaterally |
| Bilateral CHL | Absent | Absent | Absent | Absent | Both ears conductive |
Key distinction - Otosclerosis:
- Tympanogram: Type As (stiffened)
- Reflex: Absent (stapes is fixed, cannot move)
- Useful to contrast with "third window" lesions (superior semicircular canal dehiscence): Type A tympanogram, reflex present, cochlear conductive hearing loss pattern
12. ACOUSTIC REFLEX DECAY TEST
What it is: The stimulus is presented at 10 dB above reflex threshold for 10 seconds. Normally the reflex is sustained (no significant decay).
Abnormal decay (positive test): Compliance returns to baseline by >50% within 10 seconds
Significance: Positive decay strongly suggests retrocochlear pathology (CN VIII lesion - acoustic neuroma/vestibular schwannoma)
- Cochlear SNHL: Normal reflex thresholds (or slightly elevated) - no decay
- Neural SNHL (acoustic neuroma): Reflex may be elevated, absent, or present with rapid decay
As Harrison's puts it: "In neural hearing loss, such as with vestibular schwannoma, the reflex adapts or decays with time."
13. REFLEX THRESHOLD AND TYPE OF HEARING LOSS
| Hearing Loss Type | Reflex Threshold | Notes |
|---|---|---|
| Normal hearing | 70-100 dB HL | Present, normal level |
| Cochlear SNHL (mild-moderate) | Normal or mildly elevated | Loudness recruitment raises effective level |
| Cochlear SNHL (severe, >70 dB) | Often absent | Cannot reach threshold |
| Conductive (probe ear) | Absent (any degree) | Stiffened probe ear misses change |
| Conductive (stim ear, >40 dB) | Absent | Sound cannot reach threshold |
| CN VIII lesion | Absent or elevated with decay | Retrocochlear pattern |
| CN VII lesion (proximal) | Absent ipsilaterally | Facial nerve cannot drive stapedius |
| Brainstem | Absent contralaterally | Crossed pathway disrupted |
14. COMBINING TYMPANOMETRY + REFLEX: THE IMMITTANCE BATTERY
The immittance test battery = tympanogram + acoustic reflex + ear canal volume. Together they give a diagnostic profile:
| Tympanogram | Reflex | Interpretation |
|---|---|---|
| Type A | Present | Normal OR SNHL |
| Type As | Absent | Otosclerosis |
| Type Ad | Present or Absent | Ossicular discontinuity (CHL, reflex variable) |
| Type B (normal ECV) | Absent | OME (fluid in middle ear) |
| Type B (large ECV) | Absent | TM perforation / PE tube |
| Type C | Present or Absent | ET dysfunction ± early effusion |
| Type A | Absent with decay | Acoustic neuroma (CN VIII) |
| Type A | Absent, no decay | Brainstem or CN VII lesion |
15. KEY NUMBERS TO MEMORISE
| Value | What it means |
|---|---|
| -100 to +50 daPa | Normal peak pressure (adults) |
| -150 daPa | Lower limit for children |
| < -200 daPa | Type C2 (significant ET dysfunction) |
| 0.3-1.6 mL | Normal static compliance |
| 0.6-1.5 mL | Normal ECV (adults) |
| 0.3-0.9 mL | Normal ECV (children) |
| 226 Hz | Standard probe tone |
| 1000 Hz | Probe tone for infants <6 months |
| 70-100 dB HL | Normal reflex threshold range |
| ≥50% decay in 10s | Abnormal reflex decay (retrocochlear) |
| ≥10 dB CHL (probe ear) | Reflex absent in recording ear |
| ≥40 dB CHL (stimulus ear) | Reflex absent due to stimulus ear problem |
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2 (Ch. 13, 51); K.J. Lee's Essential Otolaryngology (Ch. 14); Cummings Otolaryngology (Ch. 199); Harrison's Principles of Internal Medicine 22e (Ch. 36); AAFP - Tympanometry
OAE ECOG BERA decay test speech audiometry ENT
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
OAE BERA ABR ECOG speech audiometry ENT clinical interpretation complete guide
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Finding Sources
I now have comprehensive material from multiple textbooks. Let me compile the complete master guide.
OAE, ECoG, BERA/ABR, Decay Test & Speech Audiometry - Complete Master Guide
PART 1: OTOACOUSTIC EMISSIONS (OAE)
1. WHAT ARE OAEs?
OAEs are low-level sounds generated by the outer hair cells (OHCs) of the cochlea. The active motility of OHCs serves as a mechanical amplifier of the basilar membrane; OAEs are acoustic by-products of this OHC motility - detectable with a sensitive microphone in the sealed ear canal.
- OAEs are absent if OHCs are damaged (≥35-40 dB HL of cochlear hearing loss typically abolishes them)
- They test OHC integrity only - not inner hair cells, not auditory nerve, not brainstem
- They are objective - patient does not need to respond; unaffected by sedation, anesthesia, sleep, arousal, cognitive status, language
- They cannot be recorded if middle ear is abnormal (fluid, perforation → check tympanogram first)
Key rule: OAE tests the cochlea (OHC side). ABR tests the nerve and brainstem. Together they localise lesions.
2. TYPES OF OAE
A. Spontaneous OAEs (SOAEs)
- Occur without any external stimulus
- Found in ~50-60% of normal-hearing ears
- Not used clinically (inconsistent)
B. Evoked OAEs (clinical use):
1. Transient Evoked OAEs (TEOAEs / click-evoked)
- Stimulus: Brief click or tone burst
- The cochlea produces a delayed "echo" after the click
- Response spans 0.4-6 kHz; latency 5-20 ms
- Used for: Newborn hearing screening, general OHC function assessment
- Readout: Waveform reproducibility (>70% acceptable) + amplitude (signal vs noise)
- Advantages: Fast, broadband frequency coverage
2. Distortion Product OAEs (DPOAEs)
- Stimulus: Two simultaneous pure tones (f1 and f2) at 55-85 dB SPL
- The nonlinear OHCs generate a distortion product at frequency: 2f₁ - f₂ (e.g., f₁ = 2000 Hz, f₂ = 2500 Hz → DPOAE at 1500 Hz)
- Ratio f₂/f₁ = 1.22 is optimal; f₂ level 10-15 dB lower than f₁
- The DPOAE amplitude is ~60 dB below the primary tone levels
- Used for: Frequency-specific OHC mapping, monitoring ototoxicity, monitoring noise exposure
- Displayed as a DP-gram (DPOAE amplitude vs frequency)
- Advantages: Frequency-specific - can track changes at specific cochlear regions
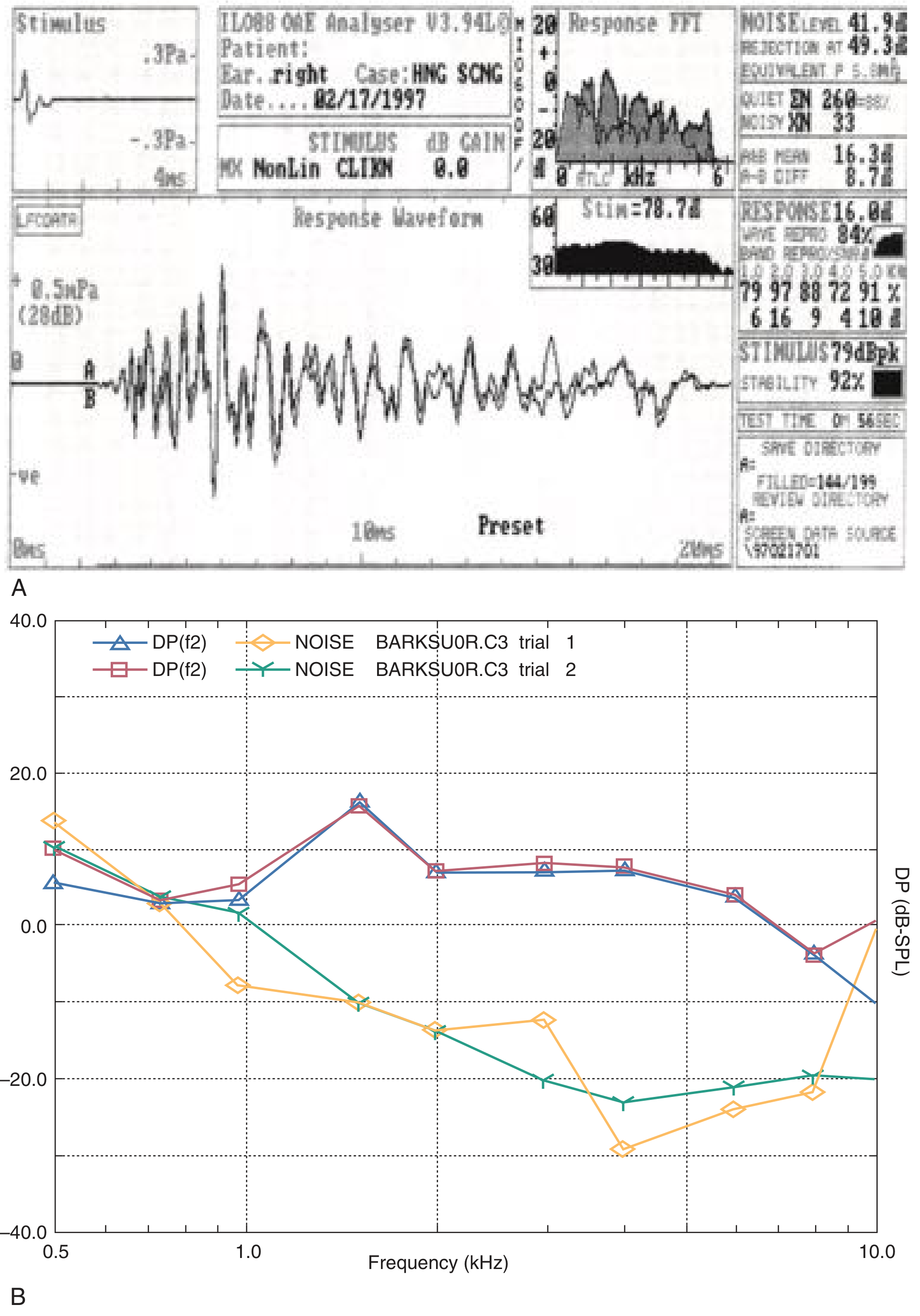
Figure: (A) TEOAE - click-evoked waveform with spectral analysis. (B) DPOAE gram - amplitude vs frequency for two trials, showing responses above the noise floor.
3. INTERPRETING OAEs
| Result | Meaning |
|---|---|
| OAEs present | OHCs functioning - hearing likely normal OR loss is retrocochlear |
| OAEs absent | OHC damage (SNHL ≥35-40 dB) OR middle ear problem |
| OAEs present + ABR absent | Auditory Neuropathy Spectrum Disorder (ANSD) - OHCs OK, nerve/inner hair cell damage |
Warning: Always pair with tympanometry. Middle ear effusion, perforation, or cerumen will suppress OAEs and give a false-negative result.
4. CLINICAL APPLICATIONS OF OAEs
| Application | Type Used | Why |
|---|---|---|
| Newborn hearing screening | TEOAE (or ABR) | Fast, objective, no patient cooperation needed |
| Ototoxicity monitoring | DPOAE | Frequency-specific early detection before PTA changes |
| Noise-induced hearing loss monitoring | DPOAE | Tracks 4 kHz region |
| Differential: cochlear vs retrocochlear | TEOAE/DPOAE | Present OAEs with poor ABR = nerve problem |
| Malingering / non-organic hearing loss | TEOAE | Objective; if OAEs present, hearing is at least 35-40 dB HL |
| Acoustic neuroma | TEOAE | Presence of OAEs with poor ABR - cochlea preserved |
| ANSD diagnosis | TEOAE + ECoG | OAEs present, cochlear microphonic present, ABR absent |
5. FACTORS THAT AFFECT OAEs
Do NOT affect OAEs (important for exams):
- Sleep/arousal state
- Sedation or anesthesia
- Body position
- Motivation / cognitive status
- Language barriers
Do affect OAEs:
- Middle ear pathology (must have normal tympanogram)
- Degree of hearing loss (absent if >35-40 dB HL cochlear loss)
- Probe fit / cerumen
- Ambient noise in test room
PART 2: ELECTROCOCHLEOGRAPHY (ECoG / ECochG)
6. WHAT IS ECoG?
ECoG records neuroelectric events generated by the cochlea and auditory nerve in response to sound. It measures the earliest electrical responses - at the cochlear level.
Three components recorded:
| Component | Generator | What it reflects |
|---|---|---|
| CM (Cochlear Microphonic) | Outer hair cells | Mirrors the stimulus waveform; "follows" the sound like a microphone |
| SP (Summating Potential) | Inner hair cells + basilar membrane | DC shift; reflects basilar membrane displacement |
| AP (Action Potential) | Auditory nerve (CN VIII) | Same as Wave I of ABR; whole-nerve compound action potential |
7. ELECTRODES USED
| Electrode type | Placement | Signal Quality | Invasiveness |
|---|---|---|---|
| Transtympanic | Needle through TM onto promontory | Best (highest amplitude) | Invasive (needs LA) |
| TIPtrode | Gold foil in ear canal | Moderate | Non-invasive |
| Tymptrode | On surface of TM | Good | Minimal |
| Extratympanic | Ear canal wall | Least good | Non-invasive |
8. THE SP/AP RATIO - DIAGNOSTIC KEY
The main measurement in ECoG is the SP/AP ratio (or SP/AP amplitude percentage).
- Normal: SP is a small shoulder/deflection before the AP; ratio is low
- Endolymphatic hydrops (Meniere's disease): Basilar membrane is distorted → SP amplitude increases relative to AP → elevated SP/AP ratio
Abnormal thresholds (SP/AP ratio):
| Electrode | Abnormal Threshold |
|---|---|
| TIPtrode (ear canal) | >50% |
| Tymptrode (on TM) | >35% |
| Transtympanic | >30% |
Sensitivity for Meniere's: ~65-70%; false positive rate ~5%.
9. CLINICAL APPLICATIONS OF ECoG
- Meniere's disease / endolymphatic hydrops - elevated SP/AP ratio (primary use)
- Auditory Neuropathy Spectrum Disorder (ANSD) - CM present (OHCs intact) but AP/ABR absent (nerve dysfunction)
- Intraoperative monitoring of cochlear function
- Threshold estimation (largely replaced by ABR now)
- Enhancing Wave I of ABR when it is absent or difficult to identify (helps interpeak latency measurements)
- Acoustic neuroma detection (largely replaced by ABR + MRI)
PART 3: AUDITORY BRAINSTEM RESPONSE (ABR / BERA)
(BERA = Brainstem Evoked Response Audiometry - same test, different name used in UK/India)
10. WHAT IS ABR/BERA?
The ABR is a surface-recorded electrophysiological response representing the synchronized electrical activity of the auditory nerve and brainstem nuclei in response to sound.
- Objective test - requires no patient response
- NOT affected by: sedation, sleep, most anesthetics, drugs, arousal state
- IS affected by: body temperature (latencies change), sex (females have slightly shorter latencies), age, degree of hearing loss
- Stimulus: Click (100 µs rectangular pulse, broad spectrum, activates basal cochlea = 2000-4000 Hz region) or tone bursts for frequency-specific threshold testing
- Recording: Surface electrodes on forehead/vertex (non-inverting), earlobe/mastoid (inverting), forehead centre (ground)
- 1000-3000 sweeps are averaged to reduce noise
11. THE ABR WAVEFORM - WAVES I TO V
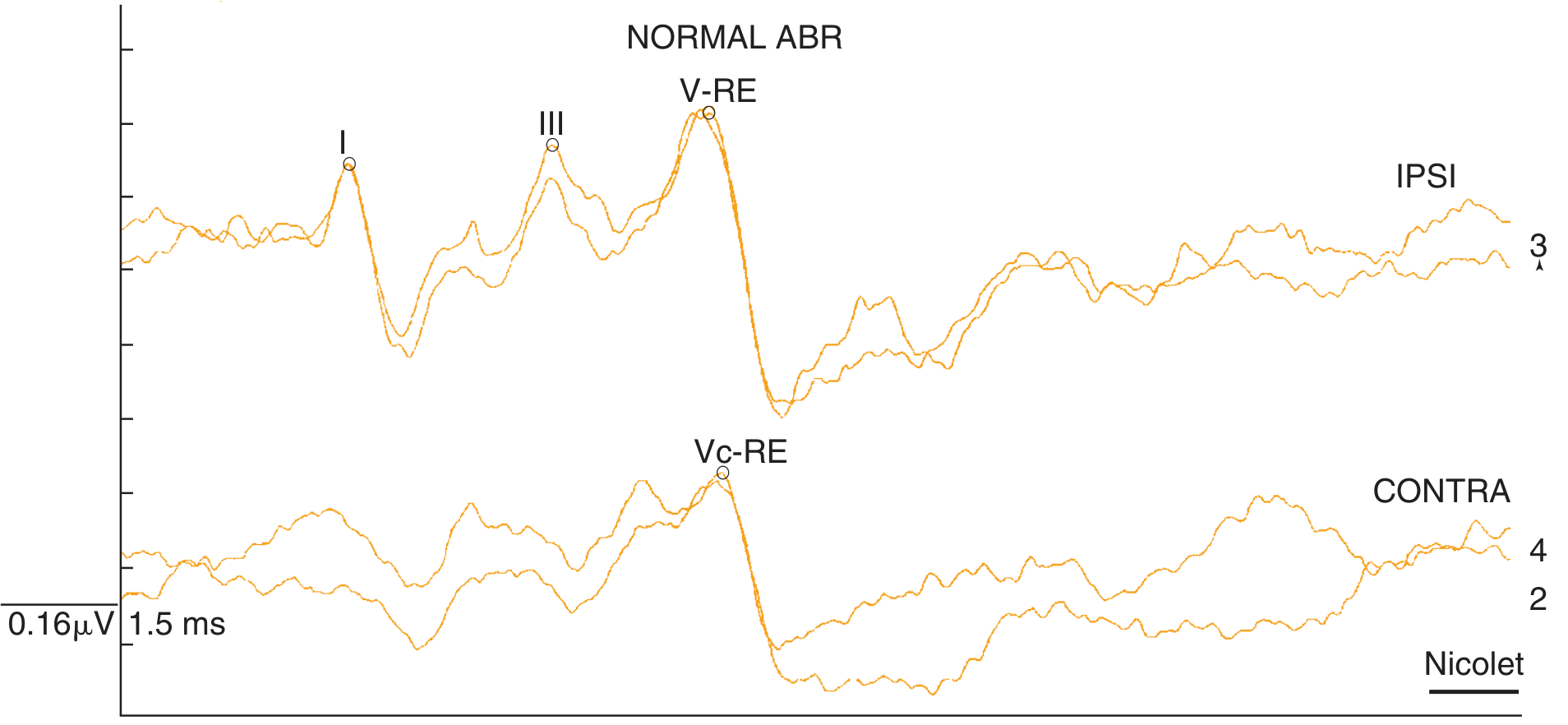
Normal ABR: Waves I, III, and V labelled. Two replicated traces overlying each other confirm validity. Wave V is the most prominent and robust peak.
Generator sites - Mnemonic: "EECOL" (from K.J. Lee)
| Wave | Generator | Latency (approx) |
|---|---|---|
| I | Distal CN VIII (cochlear nerve) | ~1.5 ms |
| II | Proximal CN VIII | ~2.5 ms |
| III | Cochlear nucleus (ipsilateral) | ~3.5 ms |
| IV | Superior olivary complex | ~4.5 ms |
| V | Lateral lemniscus / inferior colliculus | ~5.5 ms |
Wave V is most robust - persists at low stimulus levels and with significant hearing loss. Wave I is most affected by peripheral hearing loss.
12. NORMAL INTERPEAK LATENCIES (CRITICAL NUMBERS)
| Interval | Normal Value | What it assesses |
|---|---|---|
| I-III | 2.3 ms | Cochlear nerve → cochlear nucleus (peripheral to low brainstem) |
| III-V | 2.1 ms | Cochlear nucleus → lateral lemniscus (brainstem) |
| I-V | 4.4 ms | Entire auditory nerve + brainstem pathway |
| Interaural Wave V latency difference | <0.2-0.4 ms | Symmetry of brainstem function |
Abnormal = any interpeak latency above these values, or interaural wave V difference >0.2-0.4 ms
13. ABR USES
A. Threshold ABR (Hearing Estimation)
- Click ABR correlates with pure-tone thresholds at 2000-4000 Hz
- Tone-burst ABR gives frequency-specific thresholds
- Used for: Newborns, uncooperative patients, malingering, medico-legal
- Wave V threshold correlates to behavioural threshold +10-15 dB (click-ABR)
B. Neurodiagnostic ABR (Retrocochlear screening)
- High stimulus level: 80-95 dB nHL
- Screens for acoustic neuroma / vestibular schwannoma and brainstem lesions
- Sensitivity for acoustic neuroma: >90% in older studies; modern MRI has largely replaced it but ABR used when MRI contraindicated
ABR abnormalities indicating retrocochlear pathology:
- I-V interpeak latency >4.4 ms
- I-III interpeak latency >2.3 ms
- III-V interpeak latency >2.1 ms
- Interaural wave V latency difference >0.2-0.4 ms
- Absent wave V with preserved wave I or III ← definitive sign
- Complete absence of ABR (if not explained by degree of hearing loss)
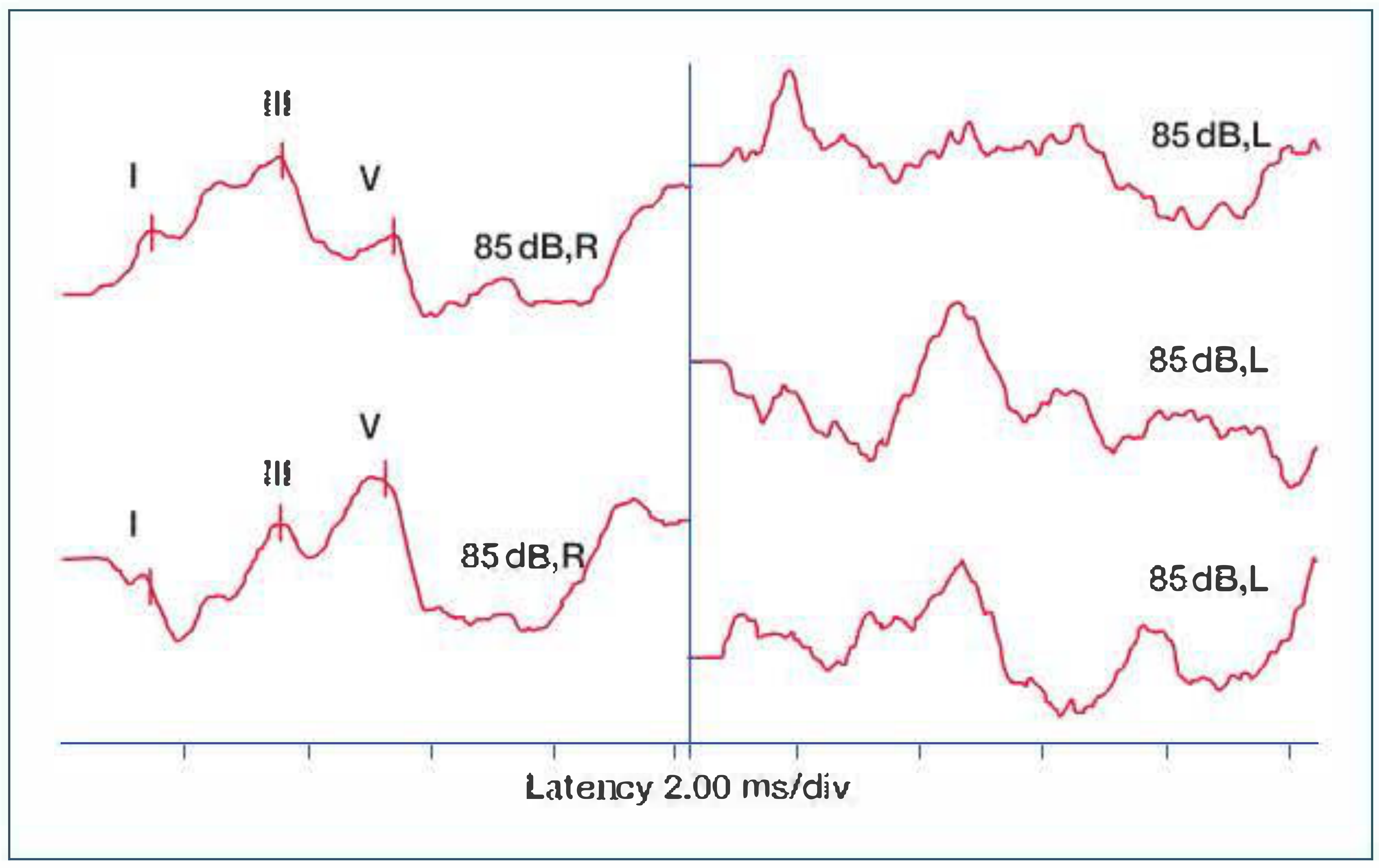
Left ear (L side): Note poorly formed, delayed waveform with no clear Wave V at 85 dB. Right ear (R side): Normal well-defined waves I, III, V. This pattern is characteristic of a left-sided acoustic neuroma.
C. Intraoperative monitoring
- Real-time monitoring during CPA surgery (acoustic neuroma resection, microvascular decompression)
- Changes in wave V latency or amplitude warn surgeon of traction on CN VIII
14. ABR IN AUDITORY NEUROPATHY SPECTRUM DISORDER (ANSD)
ANSD = normal OHC function (OAEs + cochlear microphonic present) but absent/abnormal ABR (inner hair cells or auditory nerve dysfunctional)
| Test | ANSD Result |
|---|---|
| OAEs | Present (OHCs intact) |
| Cochlear microphonic (ECoG) | Present |
| ABR | Absent or severely abnormal |
| PTA | Variable - mild to severe SNHL |
| Word recognition | Disproportionately poor |
Causes: neonatal jaundice, hypoxia, genetic (otoferlin mutations), auditory neuropathy
PART 4: THE DECAY TEST (Tone Decay Test)
15. WHAT IS TONE DECAY?
Tone decay tests measure auditory adaptation/fatigue - the ability to maintain perception of a continuous tone over time.
Principle: In a normal ear, a continuous tone just above threshold remains audible. In retrocochlear (nerve) pathology, the nerve fatigues rapidly and the tone seems to "fade" away, requiring progressive loudness increases to remain audible.
16. PERFORMING THE TEST
Method (Carhart/Rosenberg tone decay test):
- Present a continuous tone at 5 dB above threshold for 60 seconds
- Patient signals as long as they hear it
- If perception fades before 60 seconds, raise level by 5 dB
- Continue raising until audible for the full 60 seconds
- The total rise in dB above threshold = the decay value
17. INTERPRETING TONE DECAY
| Decay amount | Interpretation |
|---|---|
| 0-5 dB | Normal |
| 5-15 dB | Mild - can be cochlear or normal variant |
| ≥20-25 dB | Significant - retrocochlear pathology (CN VIII lesion) |
| ≥30 dB at any single frequency | Strongly suggestive of acoustic neuroma |
Acoustic reflex decay test (see previous guide) uses the same principle: reflex fades within 5-10 seconds at 10 dB above reflex threshold = retrocochlear.
Rollover on PIPB (Performance Intensity Function for PB words):
- As speech level increases, WRS normally improves then plateaus
- If WRS falls (rollover) at higher levels = retrocochlear lesion
- Retrocochlear lesions → "rollover phenomenon" - discrimination worsens at louder levels
Shambaugh: "Decay of the reflexive stiffening of the tympanic membrane to half-amplitude in 5 sec or less is suggestive of retrocochlear pathology."
Clinical note: Tone decay and stapedial reflex decay tests are now largely replaced by ABR + MRI for acoustic neuroma screening. They remain conceptually important and exam-relevant.
18. SUMMARY: COCHLEAR vs RETROCOCHLEAR DIFFERENTIATION
| Test | Cochlear Loss | Retrocochlear Loss |
|---|---|---|
| OAEs | Absent (OHC damage) | Present (cochlea intact) |
| Tone decay | Minimal (<15 dB) | Significant (≥20 dB) |
| Reflex decay | Normal (sustained) | Decay within 5 sec |
| ABR interpeak latency | Normal or mildly prolonged | Prolonged >4.4 ms I-V |
| Rollover (PIPB) | Absent | Present |
| Recruitment | Present | Absent |
| SISI score | High (>70%) | Low (<20%) |
| Word recognition (WRS) | Good (correlates with PTA) | Poor (disproportionately) |
PART 5: SPEECH AUDIOMETRY
19. WHAT IS SPEECH AUDIOMETRY?
Speech audiometry tests hearing for speech rather than pure tones. It assesses both the threshold for speech and the ability to understand speech at suprathreshold levels.
Tests pure-tone thresholds + functional speech understanding. Expressed as dB HL.
Preferred method: recorded speech (CD/digital) rather than monitored live voice (MLV), which is less reproducible.
20. COMPONENTS OF SPEECH AUDIOMETRY
A. Speech Awareness/Detection Threshold (SAT / SDT)
- Lowest level at which patient can detect the presence of speech (not identify it)
- Used when SRT cannot be obtained (children, language barriers, cognitive impairment)
- Should agree with the best pure-tone threshold within 10 dB anywhere on the audiogram (speech is a complex broad-band signal)
- Typically 5-10 dB better than SRT
B. Speech Recognition Threshold (SRT)
- Lowest level at which patient can correctly repeat spondee words in 50% of presentations
- Spondee = two-syllable compound word with equal stress on both syllables
- Examples: railroad, sidewalk, eardrum, baseball, hotdog, airplane, birthday
- Key relationship: SRT should be within ±10 dB of the PTA (500 + 1000 + 2000 Hz ÷ 3)
- If SRT and PTA disagree by >10 dB → consider non-organic hearing loss (malingering), or use 2-frequency best PTA for sloping audiograms
Uses of SRT:
- Confirms PTA accuracy
- Establishes reference point for WRS testing
- Detects non-organic hearing loss (functional/malingering)
C. Word Recognition Score (WRS) / Speech Discrimination Score (SDS)
(Older term: "speech discrimination")
- Percentage of phonetically balanced (PB) words correctly repeated
- Presented at 25-35 dB above SRT (sensation level) - this is the "most comfortable level" range
- Uses PB word lists (phonemes occur in same proportions as in natural English)
- UK/ENT: Often uses Phonetically Balanced (PB) or Consonant-Vowel-Nucleus-Consonant (CNC) word lists
WRS Score Interpretation (K.J. Lee):
| Score | Category |
|---|---|
| 90-100% | Normal |
| 76-88% | Slight difficulty |
| 60-74% | Moderate difficulty |
| 40-58% | Poor |
| ≤40% | Very poor |
Normal hearing and pure CHL: WRS typically 88-100% (middle ear problem doesn't affect cochlear discrimination)
Cochlear SNHL: Variable WRS - usually reduced in proportion to hearing loss
Retrocochlear / CN VIII lesion: WRS disproportionately poor relative to degree of PTA loss ("poor discrimination out of proportion to loss") + rollover phenomenon
21. THE SPEECH AUDIOGRAM AND ROLLOVER
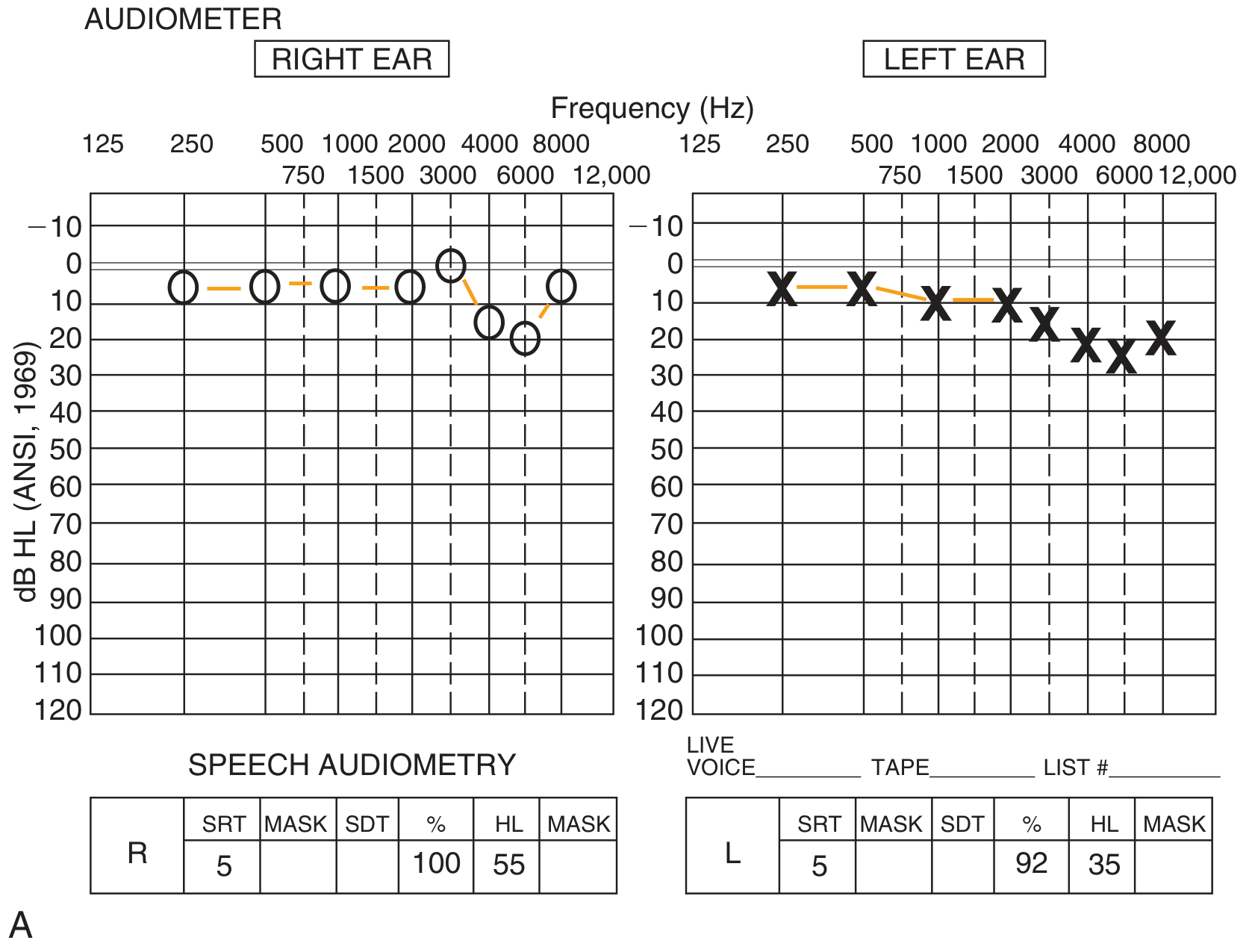
Speech audiometry section of a complete audiogram report: SRT 5 dB both ears; right ear 100% WRS at 55 dB HL; left ear 92% WRS at 35 dB HL.
The PIPB (Performance Intensity Function for PB words) / Rollover:
- Normal pattern: WRS increases as presentation level increases, reaching a plateau (PB-MAX)
- Rollover pattern: WRS peaks then decreases at higher presentation levels
- Rollover index = (PB-MAX - PB-Min) ÷ PB-Max
- If rollover index >0.45 = suggestive of retrocochlear pathology
22. MOST COMFORTABLE LEVEL (MCL) & UNCOMFORTABLE LOUDNESS LEVEL (UCL)
- MCL (Most Comfortable Level): Intensity at which speech is most comfortably heard (~40-50 dB SL above SRT)
- UCL (Uncomfortable Loudness Level): Intensity at which sound is uncomfortably loud (~90-100 dB HL in normal ears)
- Dynamic Range = UCL - SRT: Normal = ~90 dB; Reduced in cochlear SNHL (loudness recruitment = UCL normal but SRT elevated → narrow dynamic range → important for hearing aid fitting)
23. SPEECH AUDIOMETRY IN SITE-OF-LESION TESTING
| Condition | SRT-PTA agreement | WRS | Rollover |
|---|---|---|---|
| Normal | Agrees (±10 dB) | 90-100% | None |
| Pure CHL | Agrees | Normal (88-100%) | None |
| Cochlear SNHL | Agrees | Reduced (correlates with loss) | Absent |
| Retrocochlear | May agree | Disproportionately poor | Present |
| Non-organic | Disagreement | Variable/inconsistent | - |
PART 6: THE COMPLETE TEST BATTERY - HOW IT ALL FITS TOGETHER
| Question | Test(s) |
|---|---|
| Is there hearing loss? | PTA audiogram |
| What type? (CHL / SNHL / Mixed) | PTA + tympanometry |
| Is cochlea (OHC) intact? | OAE |
| Is the nerve/brainstem intact? | ABR (BERA) |
| Is it cochlear or retrocochlear? | OAE + ABR + tone decay + reflex decay + WRS |
| Is it Meniere's / endolymphatic hydrops? | ECoG (SP/AP ratio) |
| How well does patient understand speech? | WRS / speech audiometry |
| Newborn screening? | OAE (TEOAE) or ABR |
| Auditory neuropathy? | OAE present + ABR absent |
| Acoustic neuroma screening? | ABR → if abnormal → MRI |
| Malingering / non-organic? | OAE, ABR, SRT-PTA disagreement |
KEY NUMBERS TO MEMORISE
| Number | Meaning |
|---|---|
| 35-40 dB HL | OAEs absent above this cochlear loss |
| 2f₁-f₂ | DPOAE frequency formula |
| SP/AP >50% (TIPtrode) | Abnormal ECoG (Meniere's) |
| SP/AP >35% (Tymptrode) | Abnormal ECoG |
| SP/AP >30% (Transtympanic) | Abnormal ECoG |
| I-III: 2.3 ms | Normal ABR interpeak latency |
| III-V: 2.1 ms | Normal ABR interpeak latency |
| I-V: 4.4 ms | Normal ABR interpeak latency |
| Interaural Wave V: <0.2-0.4 ms | Normal asymmetry |
| SRT within ±10 dB of PTA | Normal agreement (confirms PTA) |
| 25-35 dB above SRT | Level for WRS testing |
| WRS 90-100% | Normal discrimination |
| Rollover index >0.45 | Retrocochlear suspect |
| Tone decay ≥20 dB | Retrocochlear suspect |
| Reflex decay >50% in 5-10 sec | Retrocochlear suspect |
Sources: Cummings Otolaryngology (Ch. 134); Scott-Brown's Vol. 2 (Ch. 51); K.J. Lee's Essential Otolaryngology (Ch. 14); Shambaugh Surgery of the Ear; Harrison's Principles of Internal Medicine 22e
Pediatrics hearing assessment
Finding Sources
Finding Sources
Finding Sources
Searching the Web
pediatric hearing assessment age-appropriate tests BOA VRA CPA play audiometry newborn screening
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK580492
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading Web Page
https://www.entlecture.com/audiometry-objective-tests-for-he…
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, rich data from multiple authoritative sources. Let me compile the complete guide.
Pediatric Hearing Assessment - Complete Master Guide
1. WHY PEDIATRIC HEARING ASSESSMENT IS DIFFERENT
Children cannot reliably perform adult PTA. The test approach must match:
- Developmental age (not just chronological age - always test to the child's developmental level)
- Cooperation and attention span
- Motor control (head turning, hand movements)
The result: a stepped, age-appropriate battery of tests is used.
2. EPIDEMIOLOGY & PREVALENCE
- Congenital permanent hearing loss (moderate-profound): ~1.1-1.6 per 1000 live births
- NICU infants: 2-4 per 1000 (nearly double general population)
- WHO estimate: 7.5 million children worldwide with clinically significant hearing loss
- Risk-factor-based targeted screening identifies only ~50% of affected infants - which is why universal screening is needed
- Late-onset/progressive PCHI adds to this: prevalence rises from ~0.91/1000 at age 3 to ~1.65/1000 at age 9
3. THE 1-3-6 RULE (JCIH - Joint Committee on Infant Hearing)
The gold standard framework for early intervention:
| Target | Deadline |
|---|---|
| Screen all newborns | By 1 month of age |
| Diagnose those who fail screen | By 3 months of age |
| Intervene (amplification/therapy) | By 6 months of age |
Why it matters: Every month of delay in intervention worsens speech, language, literacy, educational, behavioural, and quality-of-life outcomes. Early identification (before 6 months) dramatically improves speech-language outcomes.
Before universal NHS, median age of hearing aid fitting in the UK was 26 months. With NHS, diagnosis is confirmed by 9 months. - Scott-Brown's
4. RISK FACTORS FOR PERMANENT CONGENITAL HEARING LOSS (JCIH)
| Category | Specific Factors |
|---|---|
| Family history | Family member with childhood SNHL |
| NICU stay | >48 hours (10x increased risk) |
| In utero infections (TORCH) | Toxoplasmosis, Rubella, CMV (most common), Herpes, Syphilis |
| Craniofacial | Pinna/ear canal anomalies, ear tags, ear pits, temporal bone anomalies |
| Syndrome | Down syndrome, CHARGE, Waardenburg, Usher, Pendred, Branchio-oto-renal |
| Neurological | Hyperbilirubinemia (requiring exchange transfusion), hypoxic-ischemic encephalopathy |
| Ototoxic medications | Aminoglycosides, loop diuretics, cisplatin |
| Bacterial meningitis / encephalitis | Post-infectious SNHL |
| Head trauma | Basal skull/temporal bone fracture |
| Chemotherapy | Cisplatin especially |
Important: The most common causes of congenital hearing loss in infants without apparent risk factors are:
- Recessive genetic hearing loss (GJB2/connexin 26 mutations - most common genetic cause)
- Congenital CMV infection
This is why universal (not just risk-factor-based) screening is needed.
5. AGE-APPROPRIATE HEARING TESTS - THE MASTER CHART
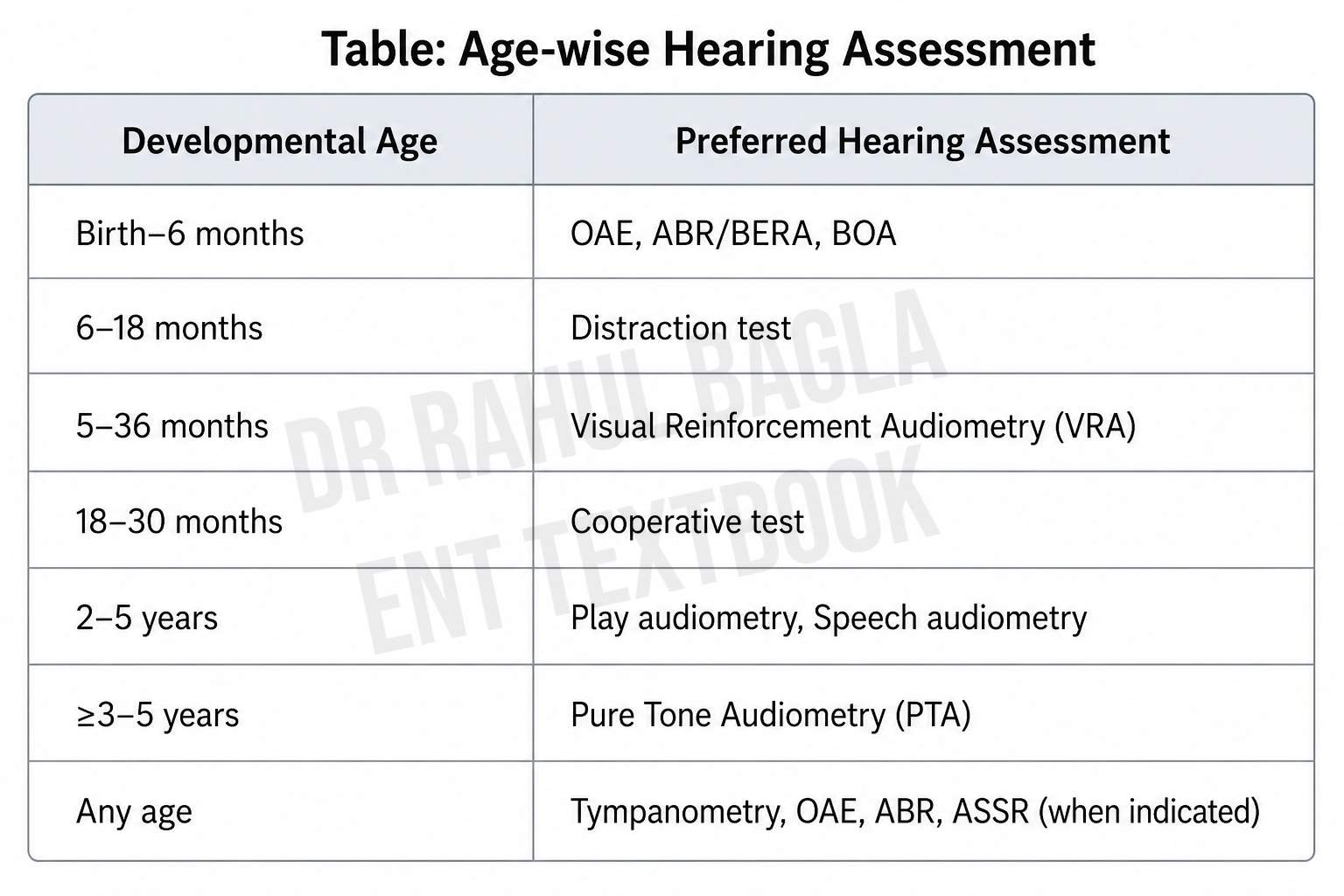
STAGE 1: BIRTH TO 6 MONTHS - Newborn Hearing Screening (NHS)
Tools: OAE + AABR (Automated ABR)
OAE Screening:
- TEOAE: Click-evoked; broad frequency; detectable from ~30 weeks gestation
- DPOAE: More frequency-specific but less sensitive below 4 kHz
- Both give binary PASS/REFER result
- Fast, inexpensive, no patient cooperation needed
- Limitation: Misses auditory neuropathy; affected by middle ear fluid/debris
AABR (Automated ABR):
- Automated algorithm gives PASS/REFER based on Wave V detection
- Preferred in NICU infants - catches auditory neuropathy that OAE misses
- Slightly higher cost but lower false-positive rate than OAE
Screening Protocols:
- Well babies: Two-stage - TEOAE first; if fail → AABR
- NICU/SCBU babies: TEOAE + AABR (both); AABR is primary
- Screen at least 12-24 hours after birth (to allow amniotic fluid to clear)
- False-positive rate: 1-2% (well below earlier 6-10%)
Key limitation of OAE-only programmes: Will miss auditory neuropathy spectrum disorder (ANSD) - OAEs present, ABR absent. This is predominantly a NICU population problem, so AABR is prioritised there.
STAGE 2: 0-6 MONTHS - Behavioural Observation (BOA)
(Also called Behavioural Observation Audiometry - but ASHA prefers "Behavioural Observation" as it does NOT yield thresholds)
Principle: Observe unconditioned reflex responses to sound stimuli
Responses looked for in neonates/infants:
- Moro reflex (startle) to loud sounds
- Auro-palpebral reflex (APR) - eye blink to sudden loud sound
- Cessation of activity (quieting)
- Arousal from sleep
- Eye widening, head turning (rudimentary)
- Changes in sucking pattern
Stimuli used: Warble tones, speech, noisemakers (rattles, bells), narrow-band noise
Important limitations:
- Does not give reliable thresholds - response depends on state, habituation
- Habituation occurs rapidly (only 2-3 responses obtainable)
- Minimum response levels (not thresholds): typically 40-70 dB (neonates), 30-50 dB (6 months)
- Cannot test each ear separately (free-field)
- Used to observe auditory behaviour only - not a screening or threshold test
STAGE 3: 6-18 MONTHS - Distraction Test (Health Visitor Distraction Test - HVDT)
(More commonly used in UK/Indian ENT exams)
Principle: The child, seated on parent's lap, is distracted by an assistant in front while the tester makes sounds to the side and behind at ear level. The child turns to locate the sound.
Setup:
- Two examiners: one distracts child frontally, one presents sounds from the side at ~1 metre distance at ear level
- Sound presented at 35-40 dB (approximate conversation level)
- Stimuli: Manchester rattle (high frequency), voice "s" sound (high frequency), voice "oo" sound (low frequency)
- Positive response: head turn toward sound source
- Ear-specific testing not reliably possible
Prerequisites:
- Child must be able to sit up with some head control
- Must be alert/cooperative
- Age: ideally 7-8 months (before head turning declines)
Limitations:
- Poor sensitivity and specificity (UK abandoned it with UNHS introduction)
- Tester technique-dependent
- Habituation rapidly occurs
- Cannot give reliable frequency-specific thresholds
STAGE 4: 6-24 MONTHS - Visual Reinforcement Audiometry (VRA)
(The primary reliable behavioural test for this age range)
Principle: Operant conditioning - teach the child that turning toward a sound source is rewarded with a visual reinforcer (animated toy / video clip).
How it's done:
- Child sits on parent's lap between two speakers + visual reinforcers (at 90° left and right)
- Conditioning phase: Pair sound + visual reward (toy lights up, animated display activates) several times to teach the association
- Testing phase: Present sound alone; reward only correct head turns toward the stimulus ear
- Start at easy levels to reinforce, then reduce intensity to find threshold
- Threshold = lowest level with consistent correct localisation responses
Testing modes:
- Sound field (speakers): Tests both ears together; cannot give ear-specific data
- Earphones/insert earphones: Gives ear-specific data (preferred)
- Bone conduction oscillator: Tests sensorineural component
Age requirements:
- Child must sit unassisted with adequate head/neck control
- Must sustain attention for head turns
- Typically starts at ~6 months corrected age; optimal 6-24 months
- Some children can use VRA until 36 months
Key teaching point: VRA gives true hearing thresholds (unlike BOA). It is the gold standard behavioural test for 6-24 month olds.
Normal limits in children: ≤15 dB HL (stricter than adults ≤20 dB HL) - because speech/language development depends on more sensitive hearing
STAGE 5: 2-5 YEARS - Conditioned Play Audiometry (CPA)
(Also called Play Audiometry)
Principle: Operant conditioning using a play task instead of a visual reward. The child performs a simple motor action (placing a peg in a board, dropping a ball in a bucket, putting a ring on a stick) each time they hear a tone.
How it's done:
- Establish the game: "Wait... listen... do it!" - demonstrate with hand-over-hand guiding
- Once conditioned, present tones at different frequencies and intensities
- Child completes the play action only when they hear the tone
- Threshold = lowest level with consistent responses
Testing setup: Same as adult PTA - earphones, bone oscillator, soundproofed room
- Frequencies tested: 250-8000 Hz (as tolerated)
- Gives ear-specific, frequency-specific thresholds
- Speech audiometry also possible: SAT (speech detection) or picture-pointing WRS tasks
Age range: 2-5 years; some 2-year-olds require VRA technique
Advantages over VRA:
- Motor response is more deliberate and reliable
- Less dependent on visual reinforcer novelty
- Can test more frequencies
STAGE 6: ≥5 YEARS - Standard Pure Tone Audiometry (PTA)
- Adult technique from ~age 5, or earlier if child can cooperate
- All standard PTA procedures apply
- Normal hearing in children: ≤15 dB HL across frequencies
- Speech audiometry using picture-pointing and then words as appropriate
6. OBJECTIVE TESTS - USED AT ANY AGE
These do not require patient cooperation and supplement or replace behavioural tests:
Tympanometry in Children
- Standard probe tone: 226 Hz (children >6-7 months)
- Infants <6 months: 1000 Hz probe tone (external canal too compliant at 226 Hz → spuriously normal or flat results)
- Normal ECV in children: 0.3-0.9 mL
- Key use: Detecting OME (glue ear) - very common cause of conductive hearing loss in children
- Type B flat tympanogram = OME until proven otherwise
- Normal hearing in children ≤15 dB HL (not 20 dB like adults)
OAE in Children
- Can be performed at any age including neonates
- Requires intact middle ear (check tympanogram first)
- Used for: Newborn screening, monitoring ototoxicity, screening in school programs
- Present = OHCs functioning; Absent = OHC damage or middle ear problem
Diagnostic ABR in Children
- Done when behavioural testing is unreliable or when retrocochlear pathology suspected
- Requires sedation in infants and young children (natural sleep or chloral hydrate)
- Threshold ABR (tone-burst): Used to estimate frequency-specific hearing thresholds before behavioural testing is possible
- Wave V threshold correlates to PTA at 2000-4000 Hz (±10-15 dB)
- Click ABR for neurodiagnostic purposes (retrocochlear, ANSD)
ASSR (Auditory Steady State Response)
- Presents modulated tones; computer determines response statistically
- Frequency-specific (500, 1000, 2000, 4000 Hz separately)
- Objective thresholds in each ear across all speech frequencies
- Better than click-ABR for estimating low-frequency thresholds
- Used for: Infants with failed NHS, when tone-burst ABR thresholds are needed across all frequencies, hearing aid prescription in infants
- ASSR thresholds correlate well with behavioural audiogram
Acoustic Reflexes in Children
- Useful at any age
- In combination with tympanometry adds diagnostic value
- Absent reflexes + Type B tympanogram = strong evidence for OME
7. NORMAL HEARING DEVELOPMENTAL MILESTONES
| Age | Expected Auditory Behaviour |
|---|---|
| 0-3 months | Startles to loud sounds; stirs/wakes to sound; quiets to familiar voice |
| 3-6 months | Turns eyes toward sound source; responds to voice; vocalises (cooing) |
| 6-9 months | Localises sounds on same plane (head turn); babbles; responds to name |
| 9-12 months | Localises sounds above and below; responds to "no"; one word |
| 12-18 months | Points to named objects/body parts; 1-3 words; imitates sounds |
| 18-24 months | 2-word phrases; follows 2-step commands; 50+ words |
| 2-3 years | Short sentences; understood by strangers 50-75% |
| 3-4 years | Complex sentences; understood by strangers; asks "why" questions |
| 4-5 years | Complete sentences; understood nearly 100%; tells stories |
Red flags requiring urgent referral:
- No response to sound by 3 months
- No babbling by 12 months
- No single words by 16 months
- No 2-word phrases by 24 months
- Any loss of previously acquired language at any age
8. UNIVERSAL NEWBORN HEARING SCREENING (UNHS) PROGRAMMES
US Programme (EHDI - Early Hearing Detection and Intervention)
- Goal: 1-3-6 rule (screen by 1 month, diagnose by 3 months, intervene by 6 months)
- Coverage: 98% of US newborns now screened before 1 month
- OAE (TEOAE/DPOAE) or AABR depending on nursery (well-baby vs NICU)
UK Programme (NHSP - Newborn Hearing Screening Programme)
- Well-baby protocol: TEOAE → if fail → AABR (two-stage, two-technology)
- NICU protocol: TEOAE + AABR (both performed); AABR is primary decision-maker
- Pass criteria: Pass in both ears at either stage
- Babies passing AABR but failing OAE in both ears = on CMV risk register (possible ANSD)
Screening result workflow:
PASS → Ongoing developmental surveillance (can develop later-onset loss)
REFER → Repeat screen → REFER again → Diagnostic audiological assessment by 3 months
↓
Full battery: Diagnostic ABR, ASSR, OAE, tympanometry, ± tone-burst ABR
9. CONGENITAL CMV - SPECIAL CONSIDERATION
- Most common non-genetic cause of congenital SNHL
- 90% of infected infants are asymptomatic at birth - yet still develop hearing loss
- SNHL from CMV can be progressive and late-onset - can pass newborn screen but develop loss later
- Up to 23% of asymptomatic congenital CMV infants develop SNHL
- Treatment: Valganciclovir (oral) for 6 months if symptomatic CMV with SNHL - improves hearing outcomes
- All infants failing newborn screen should be screened for cCMV within 3 weeks of birth (saliva PCR)
10. AUDITORY NEUROPATHY SPECTRUM DISORDER (ANSD) IN CHILDREN
| Feature | Finding |
|---|---|
| OAE | Present (OHCs intact) |
| Cochlear microphonic (ECoG/ABR) | Present |
| ABR | Absent or severely abnormal |
| PTA (when possible) | Variable; often disproportionately poor word recognition |
| Risk factors | Prematurity, hyperbilirubinemia, anoxia, genetic (otoferlin) |
Critical: OAE-only screening misses ANSD. AABR screening in NICU catches it. This is why AABR is mandatory for NICU infants.
11. COMPLETE PAEDIATRIC HEARING ASSESSMENT BATTERY
| Test | Age | What it assesses |
|---|---|---|
| Automated OAE | All ages (screening) | OHC function - pass/fail |
| AABR | Neonates (especially NICU) | Auditory nerve + brainstem - pass/fail |
| Tympanometry (1000 Hz) | <6 months | Middle ear |
| Tympanometry (226 Hz) | >6 months | Middle ear |
| Acoustic reflexes | >6 months | Reflex arc; supplements tympanometry |
| BOA | 0-6 months | Auditory behaviour observation (no thresholds) |
| Distraction test | 6-18 months | Gross hearing check |
| VRA | 6-24 months | Behavioural hearing thresholds |
| CPA (Play audiometry) | 2-5 years | Behavioural hearing thresholds (ear-specific) |
| Standard PTA | ≥5 years | Complete audiogram |
| Diagnostic ABR | Any age | Threshold estimation; retrocochlear; ANSD |
| ASSR | Any age (esp. infants) | Frequency-specific objective thresholds |
| Speech audiometry | ≥2 years (picture-pointing) | Speech detection, recognition |
12. KEY NUMBERS TO MEMORISE
| Number | What |
|---|---|
| 1/1000 live births | Prevalence congenital moderate-profound SNHL |
| 2-4/1000 | NICU population rate |
| 1-3-6 rule | Screen 1 month, diagnose 3 months, intervene 6 months |
| ≤15 dB HL | Normal hearing in children (stricter than adult ≤20 dB HL) |
| 6 months (corrected) | Earliest reliable VRA |
| 2-5 years | Play audiometry (CPA) age range |
| ≥5 years | Standard PTA |
| 1000 Hz | Probe tone for tympanometry in infants <6-7 months |
| 226 Hz | Standard probe tone (children >6-7 months) |
| 50% | What risk-factor-based screening identifies (not enough = need UNHS) |
| 30 weeks gestation | When OAEs first detectable |
| 6 months valganciclovir | Treatment for symptomatic congenital CMV with SNHL |
13. CROSS-CHECK PRINCIPLE (Jerger & Hayes, 1976)
No single test is sufficient in children. Always use a test battery and cross-check results:
- OAE + ABR + tympanometry + behavioural test should all agree
- When they disagree, investigate further
- Example: Child passes OAE but ABR absent → ANSD
- Example: Behavioural response present but OAE absent → may have OME (check tympanogram)
Sources: Scott-Brown's Otorhinolaryngology Vol. 2 (Ch. 8, 13); Cummings Otolaryngology (Ch. 193, 199); StatPearls - Hearing Loss Assessment in Children; JCIH 2019 Position Statement; AAA/ASHA Pediatric Audiologic Assessment Guidelines
Ok net issue so start again pediatrics hearing assessment again
The full guide is right above in this chat - you don't need to scroll far. Here it is again in full:
Pediatric Hearing Assessment - Complete Master Guide
1. WHY IT'S DIFFERENT FROM ADULT TESTING
Children cannot perform standard PTA. Every test must match the child's developmental age (not chronological age). A stepped, age-appropriate battery is used across all age groups.
2. EPIDEMIOLOGY
| Stat | Value |
|---|---|
| Congenital moderate-profound SNHL | ~1.1-1.6 per 1000 live births |
| NICU infants | 2-4 per 1000 (double general population) |
| Risk-factor-based screening identifies | Only ~50% of affected infants |
| Prevalence rises to age 9 | 1.65/1000 (late-onset + progressive cases) |
3. THE 1-3-6 RULE (JCIH - Joint Committee on Infant Hearing)
| Step | Deadline |
|---|---|
| Screen all newborns | By 1 month |
| Diagnose those who fail | By 3 months |
| Intervene (hearing aids/therapy) | By 6 months |
Why: Every month of delay worsens speech, language, literacy, behaviour, and quality of life. Early identification (before 6 months) dramatically improves outcomes. Before UNHS, median hearing aid fitting in UK was 26 months.
4. RISK FACTORS FOR CONGENITAL HEARING LOSS (JCIH)
| Category | Examples |
|---|---|
| Family history | Childhood SNHL in a family member |
| NICU stay >48 hours | 10x increased risk |
| In utero infections (TORCH) | Toxoplasmosis, Rubella, CMV (most common), Herpes, Syphilis |
| Craniofacial anomalies | Pinna/ear canal anomalies, ear tags, ear pits, temporal bone |
| Syndromes | Down, CHARGE, Waardenburg, Usher, Pendred, Branchio-oto-renal |
| Hyperbilirubinemia | Requiring exchange transfusion |
| Ototoxic drugs | Aminoglycosides, cisplatin, loop diuretics |
| Post-infectious | Bacterial meningitis, encephalitis |
| Head trauma | Basal skull/temporal bone fracture |
| Chemotherapy | Especially cisplatin |
Most common causes in infants WITHOUT risk factors:
- Recessive genetic hearing loss (GJB2/connexin 26 - most common overall genetic cause)
- Congenital CMV infection
→ This is why universal screening (not just targeted) is essential.
5. AGE-APPROPRIATE TESTS - THE MASTER CHART
STAGE 1: BIRTH → 6 MONTHS - Newborn Hearing Screening
Two tools: OAE and AABR
OAE (Automated OAE):
- TEOAE (click-evoked) - broadband; detectable from ~30 weeks gestation
- DPOAE - more frequency-specific but weaker below 4 kHz
- Result: binary PASS / REFER
- Fast, cheap, no cooperation needed
- Limitation: Misses auditory neuropathy; fails if middle ear has fluid/debris
AABR (Automated ABR):
- Automated algorithm detects Wave V → PASS/REFER
- Preferred for NICU infants - catches auditory neuropathy (ANSD) that OAE misses
- Slightly higher cost, lower false-positive rate than OAE
- Referral rate ~2-9% (AABR) vs 10-30% (TEOAE in suboptimal conditions)
Screening protocols:
| Population | Protocol |
|---|---|
| Well babies | TEOAE first → fail → AABR (two-stage two-technology) |
| NICU/SCBU (>48 hours) | TEOAE + AABR both performed; AABR is primary decision-maker |
- Screen at ≥12-24 hours after birth (allow amniotic fluid to clear → reduces false positives)
- False-positive rate now: 1-2% (was 6-10% early on)
NICU babies passing AABR but failing OAE in both ears → placed on CMV/ANSD risk register
STAGE 2: 0-6 MONTHS - Behavioural Observation (BOA)
Principle: Observe unconditioned reflexes to sound (no conditioning, no training)
Responses observed:
- Moro/startle reflex to sudden loud sound
- Auro-palpebral reflex (APR) - eye blink to loud sound
- Quieting / cessation of activity
- Arousal from sleep
- Eye widening, rudimentary head turn
- Changes in sucking pattern
Stimuli: Noisemakers (rattles, bells), warble tones, voice, narrow-band noise
Critical limitations:
- Does NOT give hearing thresholds - only shows auditory behaviour
- Rapid habituation (only 2-3 valid responses)
- Minimum response levels (not thresholds): ~40-70 dB neonates; 30-50 dB at 6 months
- Cannot test ears separately (sound field only)
- Not a screening test - used to observe global auditory development
Memory: BOA = Behaviour Only, no Audiogram
STAGE 3: 6-18 MONTHS - Distraction Test (HVDT)
(Health Visitor Distraction Test - important for UK/Indian ENT exams)
Setup:
- Two examiners needed
- Child sits on parent's lap, facing forward
- Distractor in front holds child's attention
- Tester presents sounds from 1 metre behind/to the side at ear level (45-90°)
- Sound level: ~35-40 dB (conversational)
- Stimuli: Manchester rattle (high-frequency), voiced "s" sound (high-frequency), "oo" sound (low-frequency)
Positive response: Child turns head toward sound source
Optimal age: 7-8 months (head control established, localisation reflex strong, habituation less rapid)
Limitations:
- Tester technique-dependent, unreliable
- Cannot give frequency-specific thresholds
- Poor sensitivity and specificity
- UK abandoned with introduction of UNHS (poor sensitivity, high refer rate, not cost-effective)
STAGE 4: 6-24 MONTHS - Visual Reinforcement Audiometry (VRA)
The primary reliable behavioural test for this age group
Principle: Operant conditioning - child learns that turning toward a sound earns a visual reward (animated toy, video clip, lighted display activating at 90° left or right)
How it works:
Phase 1 - Conditioning:
- Present sound + immediately activate visual reinforcer together
- Child learns the association: sound → turn head → see reward
- Several paired presentations until child turns reliably
Phase 2 - Testing:
- Present sound alone; reward correct head turns only
- Vary frequency and intensity to find threshold at each frequency
- Threshold = lowest level with consistent, reliable head-turn responses
Testing modes:
| Mode | What it gives |
|---|---|
| Sound field (loudspeakers) | Binaural threshold (better ear); no ear separation |
| Insert earphones | Ear-specific thresholds - preferred |
| Bone conductor | Sensorineural component per ear |
Prerequisites:
- Child can sit unsupported
- Good head and neck control for head turns
- Reliable at ~6 months corrected age onward
- Works until ~24-36 months
Key advantage: Gives TRUE hearing thresholds, unlike BOA
Normal hearing in children: ≤15 dB HL (stricter than adults ≤20 dB HL - important for speech-language development)
STAGE 5: 2-5 YEARS - Conditioned Play Audiometry (CPA / Play Audiometry)
Principle: Operant conditioning using a play motor task as the response instead of a visual reinforcer
The game: Child performs a simple action each time they hear a tone:
- Dropping a ball into a bucket
- Placing a peg in a board
- Stacking rings on a peg
- Placing a block in a box
How to condition:
- Hold the child's hand with toy ready
- "Wait... listen..." (pause for silence)
- Present tone → "Now!" → guide hand to complete task
- Repeat until child responds independently
- Begin threshold testing
What it gives:
- Ear-specific, frequency-specific thresholds (250-8000 Hz)
- Same type of result as adult PTA
- Both air and bone conduction possible
- Speech audiometry: SAT using picture-pointing; WRS with pictures
Age range: 2-5 years (some 2-year-olds need VRA; some precocious children can start CPA at 18 months)
Key difference from VRA: Motor response is deliberate and less dependent on attention to a visual reward - slightly more reliable
STAGE 6: ≥5 YEARS - Standard Pure Tone Audiometry (PTA)
- Full adult technique from ~age 5 (or earlier if able)
- Normal = ≤15 dB HL in children
- All frequencies 250-8000 Hz
- Speech audiometry with picture-pointing at 2-3 years → word lists at school age
6. OBJECTIVE TESTS - ANY AGE
These do not need patient cooperation and run alongside behavioural tests at all ages.
Tympanometry in Children
| Child's Age | Probe Tone |
|---|---|
| <6 months | 1000 Hz |
| >6 months | 226 Hz (standard) |
Why 1000 Hz for infants? The external ear canal is highly compliant in neonates. At 226 Hz, the canal wall compliance dominates and gives falsely normal (or flat) results. 1000 Hz separates canal from middle ear compliance.
- Normal ECV in children: 0.3-0.9 mL (adults 0.6-1.5 mL)
- Type B + normal ECV = OME (most common cause of conductive loss in children)
- Type B + large ECV = TM perforation or PE tube
- Normal hearing in children = ≤15 dB HL; OME typically causes flat 20-40 dB CHL
OAE in Children
- Any age including neonates
- Always check tympanogram first - middle ear effusion will suppress OAEs → false negative
- TEOAE for screening; DPOAE for ototoxicity/noise monitoring
Diagnostic ABR
- When behavioural testing unreliable (very young, developmental delay, suspected ANSD)
- Requires sedation in infants/toddlers (natural sleep, chloral hydrate, or GA)
- Threshold ABR (tone-burst): Frequency-specific threshold estimation
- Wave V threshold ≈ behavioural threshold ± 10-15 dB (at 2000-4000 Hz)
- Neurodiagnostic ABR: ANSD diagnosis, retrocochlear lesions
ASSR (Auditory Steady State Response)
- Modulated tones → computer determines response statistically (no subjectivity)
- Frequency-specific at 500, 1000, 2000, 4000 Hz per ear
- Better than click ABR for low-frequency thresholds
- Used for: Hearing aid fitting and prescription in infants before VRA is possible
- ASSR thresholds correlate well with behavioural PTA
7. NORMAL AUDITORY DEVELOPMENTAL MILESTONES
| Age | Expected Behaviour | Red Flag if Absent |
|---|---|---|
| 0-3 months | Startles to loud sound; quiets to familiar voice | No startle by 3 months |
| 3-6 months | Eyes turn toward sound; coos | No response to voices |
| 6-9 months | Localises sound on same horizontal plane; babbles | No babbling |
| 9-12 months | Localises sounds above/below; responds to name | No response to name |
| 12-16 months | Points to objects; first words | No single words by 16 months |
| 18-24 months | 2-word phrases; 50+ words | No phrases by 24 months |
| 2-3 years | Short sentences; 50-75% intelligible to strangers | |
| 3-5 years | Full sentences; nearly 100% intelligible |
Any loss of previously acquired language at any age = urgent investigation
8. UNIVERSAL NEWBORN HEARING SCREENING (UNHS) - SCREENING FLOWCHART
ALL NEWBORNS
↓
OAE / AABR (by 1 month)
↓ ↓
PASS REFER
↓ ↓
Ongoing Repeat screen
surveillance (allow amniotic fluid to clear if early)
↓
REFER again
↓
Full diagnostic assessment
(by 3 months):
ABR + ASSR + OAE + Tympanometry
± Genetic testing
± CMV testing (within 3 weeks of birth)
↓
INTERVENTION by 6 months
(hearing aids / cochlear implant referral / AVPT)
9. AUDITORY NEUROPATHY SPECTRUM DISORDER (ANSD)
| Test | ANSD Result |
|---|---|
| OAE | Present (outer hair cells intact) |
| Cochlear microphonic (ABR/ECoG) | Present |
| ABR | Absent or severely abnormal |
| PTA (when testable) | Variable; word recognition disproportionately poor |
Risk factors in children: Prematurity, hyperbilirubinemia (jaundice), perinatal hypoxia, genetic (otoferlin gene mutations)
Critical: OAE-only screening misses ANSD entirely. AABR is mandatory for NICU infants specifically because of this.
10. CONGENITAL CMV - KEY POINTS
- Most common non-genetic cause of congenital SNHL
- 90% of infected infants are asymptomatic at birth but still develop SNHL
- Hearing loss from CMV can be late-onset and progressive - passes newborn screen but develops loss later → need ongoing surveillance
- Diagnosis: Saliva/urine CMV PCR within first 3 weeks of life
- Treatment: Valganciclovir oral for 6 months in symptomatic infants → improves hearing and neurodevelopmental outcomes
11. COMPLETE TEST SELECTION BY AGE - QUICK REFERENCE
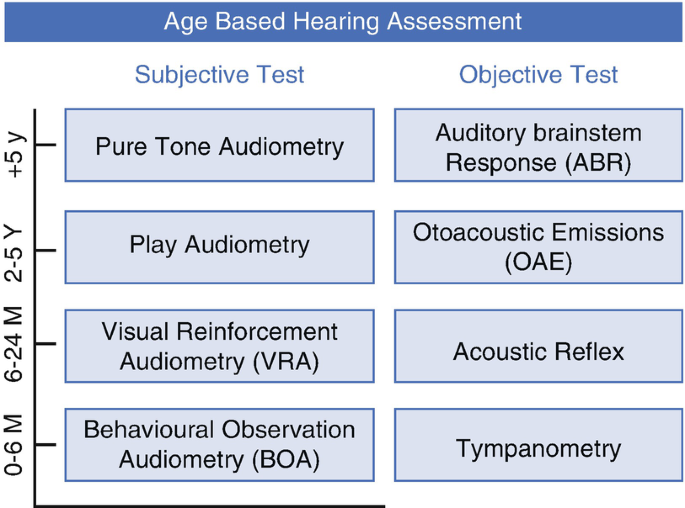
| Age | Subjective Test | Objective Tests |
|---|---|---|
| Birth - 6 months | BOA (observation only) | AABR/OAE (screening), Tympanometry (1000 Hz), ABR |
| 6 - 18 months | Distraction test, VRA | OAE, Tympanometry (226 Hz), Acoustic reflex, ASSR |
| 18 months - 2 years | VRA → CPA transition | OAE, Tympanometry, Acoustic reflex |
| 2 - 5 years | CPA (Play audiometry) | OAE, Tympanometry, Acoustic reflex |
| ≥5 years | Standard PTA | Full immittance battery |
| Any age | - | ABR, ASSR, OAE, Tympanometry (age-appropriate probe) |
12. KEY NUMBERS TO MEMORISE
| Number | Meaning |
|---|---|
| 1/1000 | Prevalence congenital moderate-profound SNHL |
| 2-4/1000 | NICU population rate |
| 1-3-6 | Screen 1m, Diagnose 3m, Intervene 6m |
| ≤15 dB HL | Normal hearing in children (not ≤20 dB like adults) |
| 6 months corrected age | Earliest reliable VRA |
| 2-5 years | CPA (Play audiometry) |
| ≥5 years | Standard PTA |
| 1000 Hz | Tympanometry probe tone for infants <6 months |
| 226 Hz | Standard probe tone for children >6 months |
| ~50% | What targeted (risk-factor) screening identifies |
| 30 weeks gestation | Earliest OAEs detectable |
| 3 weeks after birth | Window for CMV diagnosis (PCR) |
| 6 months valganciclovir | Treatment for symptomatic congenital CMV + SNHL |
Sources: Scott-Brown's Otorhinolaryngology Vol. 2 (Ch. 8, 13); Cummings Otolaryngology (Ch. 193, 199); StatPearls - Hearing Loss in Children; JCIH 2019 Position Statement; AAA/ASHA Pediatric Audiologic Assessment Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.