Discordant fetal growth
Reading File
search_medical_text
discordant fetal growth twin pregnancy definition etiology pathophysiology
search_medical_text
discordant fetal growth diagnosis management complications outcomes
search_medical_image
discordant fetal growth twin pregnancy ultrasound
GradeResponse
GradeResponse
GradeResponse
The retrieval returned no text results, so the answer below draws entirely from my own knowledge base.
Discordant Fetal Growth
Definition
Discordant fetal growth refers to a significant difference in estimated fetal weight (EFW) or abdominal circumference (AC) between two fetuses in a multiple gestation. The standard definition is:
EFW discordance ≥ 20%, calculated as:(EFW larger twin − EFW smaller twin) ÷ EFW larger twin × 100
- Mild discordance: 15–20% (considered a gray zone)
- Significant/severe discordance: ≥ 25–30% (strongly associated with adverse outcomes)
Etiology
The underlying cause differs by chorionicity:
| Factor | Dichorionic (DC) | Monochorionic (MC) |
|---|---|---|
| Placental implantation | Unequal placentation, velamentous cord insertion | Unequal placental sharing |
| Vascular complications | — | Twin-to-twin transfusion syndrome (TTTS), Twin anemia-polycythemia sequence (TAPS) |
| Structural/chromosomal anomaly | More common in DC discordance | Can occur in either twin |
| Uteroplacental insufficiency | Applies to the smaller twin's placenta | Related to territory size |
| Umbilical cord abnormalities | Marginal/velamentous insertion | Common in MC |
Pathophysiology
- In dichorionic twins, the smaller (discordant) fetus most commonly suffers from selective fetal growth restriction (sFGR) due to a poorly implanted or smaller placental share.
- In monochorionic twins, vascular anastomoses create an additional layer of complexity — unequal placental sharing combines with inter-twin transfusion physiology. TTTS and TAPS must always be excluded.
- Chronic uteroplacental insufficiency leads to fetal hypoxia → redistribution of cardiac output (brain-sparing), progressive deterioration of Doppler indices, and eventually biophysical compromise.
Classification of Selective FGR in Monochorionic Twins (Gratacos Classification)
| Type | Umbilical Artery Doppler (smaller twin) | Behavior | Risk |
|---|---|---|---|
| Type I | Positive end-diastolic flow | Stable | Low |
| Type II | Persistently absent/reversed EDF | Progressive deterioration | High IUD risk |
| Type III | Intermittently absent/reversed EDF | Unpredictable, sudden deterioration | Risk of acute co-twin demise |
Diagnosis
Ultrasound Biometry
- Serial growth scans every 2–4 weeks in at-risk pregnancies
- Key measurements: BPD, HC, AC, FL → EFW by Hadlock formula
- AC discordance ≥ 20 mm is an early warning sign
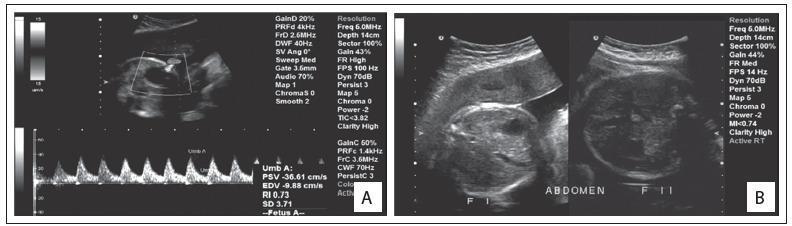
Doppler Studies
Doppler assessment of the smaller twin is central to management:
- Umbilical artery (UA): increased S/D ratio → absent end-diastolic flow (AEDF) → reversed end-diastolic flow (REDF)
- Middle cerebral artery (MCA): low pulsatility index = brain-sparing; MCA PSV elevated = fetal anemia (TAPS)
- Ductus venosus (DV): absent or reversed A-wave = imminent fetal compromise
- Umbilical vein: pulsations = severe cardiac decompensation
Additional Workup
- Amniocentesis / CVS: if structural anomaly or chromosomal cause suspected
- Detailed anatomy scan: for congenital anomalies in the smaller twin
- Placental mapping: to assess cord insertion sites (MC twins especially)
Management
General Principles
- Manage based on chorionicity, gestational age, Doppler stage, and severity of discordance
- Multidisciplinary care at a fetal medicine unit
Monitoring Frequency
| Condition | Frequency |
|---|---|
| DC twins, mild discordance | Growth scan every 2–3 weeks; Doppler weekly if abnormal |
| MC twins, any discordance | Every 1–2 weeks; Doppler surveillance mandatory |
| Abnormal Doppler (AEDF/REDF) | 2–3 times/week; consider hospitalization |
Timing of Delivery
| Situation | Recommended Delivery Gestation |
|---|---|
| DC twins, uncomplicated discordance | 36–37 weeks |
| MC twins, sFGR Type I | 34–36 weeks |
| MC twins, sFGR Type II | 32–34 weeks (individualized) |
| MC twins, sFGR Type III | 32–34 weeks (individualized, given unpredictability) |
| Reversed DV A-wave / severe biophysical compromise | Immediate delivery if viable |
Corticosteroids
- Administer betamethasone (two doses 24 hours apart) if delivery anticipated before 34–35 weeks for fetal lung maturity.
Interventional Options (Monochorionic Twins)
- Laser photocoagulation of placental anastomoses: primarily for TTTS, may also be considered in severe sFGR Type II/III in select cases
- Selective feticide (radiofrequency ablation / bipolar cord coagulation): considered when one twin has a lethal anomaly or when continuing the pregnancy threatens the co-twin's survival
Complications
Smaller Twin
- Intrauterine fetal demise (IUFD)
- Preterm birth and its sequelae
- Neonatal hypoglycemia, polycythemia
- Long-term neurodevelopmental impairment
Larger Twin (in MC pregnancies)
- Co-twin demise risk: acute hemorrhage into dead twin's placental territory → sudden neurological injury (periventricular leukomalacia, multicystic encephalomalacia) or co-twin death
- Risk is highest in Type III sFGR due to unpredictable acute arterio-arterial shunting
Both Twins
- Preterm labor
- TTTS (in MC twins)
- Iatrogenic prematurity
Prognosis
- DC twins: prognosis primarily determined by degree of discordance and Doppler status; mortality and morbidity rise sharply with EFW discordance ≥ 25% and abnormal Doppler
- MC twins: worse outcomes than DC due to shared circulation; Type II/III sFGR carry significant risks of IUFD and neurological damage even with intensive surveillance
- With appropriate fetal medicine center management, survival rates are reasonable but neurodevelopmental follow-up is mandatory for the smaller twin
Key takeaway: Discordant fetal growth requires prompt assessment of chorionicity, serial Doppler-based surveillance of the smaller twin, and timely delivery decisions — the Gratacos classification guides management in monochorionic pregnancies, while EFW discordance ≥ 20–25% with abnormal umbilical artery Doppler signals high-risk status in any twin pair.
Multiple pregnancy
search_medical_text
multiple pregnancy types complications management overview
search_medical_text
twin pregnancy chorionicity zygosity diagnosis antenatal care
search_medical_image
multiple pregnancy twin chorionicity ultrasound lambda T sign
GradeResponse
GradeResponse
GradeResponse
The retrieved text results are largely off-topic; the answer below draws primarily from my own knowledge, supplemented by the image retrieved and the aneuploidy screening point.
Multiple Pregnancy
Definition & Incidence
Multiple pregnancy refers to the simultaneous development of more than one fetus. The incidence has risen significantly with assisted reproductive technologies (ART):
- Twins: ~1 in 80 spontaneous pregnancies; much higher with ART
- Triplets: ~1 in 6,400 spontaneous; predominantly iatrogenic today
- Higher-order multiples: increasingly rare spontaneously
Zygosity and Chorionicity
These are distinct but related concepts — zygosity is biological, chorionicity determines clinical risk.
Zygosity
| Type | Origin | Characteristics |
|---|---|---|
| Dizygotic (DZ) | Two separate ova fertilized by two sperm | Always dichorionic-diamniotic (DCDA); genetically distinct |
| Monozygotic (MZ) | Single fertilized ovum splits | Chorionicity depends on timing of division |
Monozygotic Twin Types by Timing of Division
| Timing of Split | Type | Frequency |
|---|---|---|
| Days 1–3 (before implantation) | Dichorionic-Diamniotic (DCDA) | ~30% of MZ |
| Days 4–8 (inner cell mass) | Monochorionic-Diamniotic (MCDA) | ~70% of MZ |
| Days 8–12 (after amnion forms) | Monochorionic-Monoamniotic (MCMA) | ~1% of MZ |
| After day 12 | Conjoined twins | Very rare |
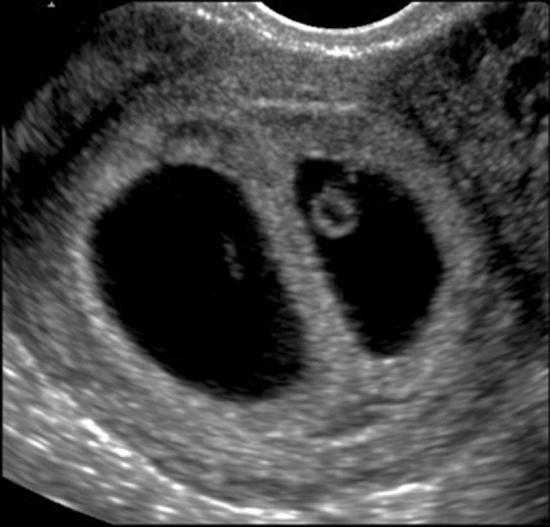
Determining Chorionicity
- Best assessed at 11–14 weeks by ultrasound
- Lambda (λ) sign = dichorionic (triangular wedge of placental tissue at membrane base)
- T-sign = monochorionic (thin membrane meets placenta at right angle, no wedge)
- Membrane thickness: DC > 2 mm; MC ≤ 2 mm
Risk Stratification by Chorionicity
| Feature | DCDA | MCDA | MCMA |
|---|---|---|---|
| Shared placenta | No | Yes | Yes |
| Shared amniotic sac | No | No | Yes |
| Perinatal mortality | Low (baseline) | 3–5× higher than DCDA | Highest |
| TTTS risk | None | 10–15% | N/A (no membrane) |
| Cord entanglement | No | No | Yes (~50%) |
| sFGR risk | Low | 10–15% | — |
Maternal Complications
Multiple pregnancy is a high-risk obstetric condition with increased risks across all systems:
Obstetric
- Preterm labour and delivery (most common — ~50% of twins deliver before 37 weeks)
- Pre-eclampsia (2–3× increased risk)
- Gestational diabetes
- Placenta praevia and abruption
- Polyhydramnios
- Anaemia (increased iron and folate demands)
- Postpartum haemorrhage (uterine overdistension)
Non-Obstetric
- Hyperemesis gravidarum (elevated hCG)
- Urinary frequency, backache, varicosities (mechanical)
- Thromboembolic disease (increased hypercoagulable state)
Fetal/Neonatal Complications
| Complication | Notes |
|---|---|
| Preterm birth | Leading cause of neonatal morbidity/mortality |
| IUGR / discordant growth | Especially in MC twins (see separate topic) |
| Twin-to-twin transfusion syndrome (TTTS) | MC twins only; 10–15% incidence |
| Twin anemia-polycythemia sequence (TAPS) | MC twins; MCA Doppler surveillance |
| Twin reversed arterial perfusion (TRAP) | MC twins; acardiac twin |
| Cord entanglement | MCMA twins |
| Congenital anomalies | 2× higher in MZ twins |
| Chromosomal abnormalities | Increased screening complexity in twins |
Antenatal Care
First Trimester
- Early booking and dating scan
- Chorionicity determination at 11–14 weeks (critical — cannot be reliably assessed later)
- Combined first-trimester screening (NT + serum markers) — each fetus assessed separately
- NIPS/cfDNA: valid in twins; DZ twins usually discordant for trisomy; counsel about selective reduction if applicable
Supplements
- Folic acid 5 mg/day (from preconception to 12 weeks)
- Iron supplementation
- Low-dose aspirin (75–150 mg/day from 12 weeks) if pre-eclampsia risk high
Monitoring Schedule (NICE/RCOG-based)
| Type | Scans | Frequency |
|---|---|---|
| DCDA | Growth + Doppler | Every 4 weeks from 20 weeks; every 2 weeks from 28 weeks |
| MCDA | Growth + Doppler | Every 2 weeks from 16 weeks |
| MCMA | Growth + Doppler + cord | Weekly from 16 weeks; admit ~26–28 weeks for monitoring |
Cervical Length
- Measurement at 18–22 weeks may predict preterm birth
- Cervical length < 25 mm → consider progesterone or cerclage in selected cases
Twin-to-Twin Transfusion Syndrome (TTTS)
A major complication unique to MCDA twins, caused by unbalanced inter-twin blood flow through placental anastomoses.
Quintero Staging
| Stage | Features |
|---|---|
| I | Oligohydramnios (donor) + polyhydramnios (recipient); bladder still visible in donor |
| II | Bladder not visible in donor twin |
| III | Abnormal Doppler (AEDF/REDF in UA, absent/reversed DV A-wave, UV pulsations) |
| IV | Hydrops in recipient twin |
| V | Demise of one or both twins |
Management
- Stages II–IV: Fetoscopic laser photocoagulation of anastomoses — treatment of choice at specialist centres
- Stage I: controversial; many centres monitor closely; some treat early
- Amnioreduction: palliative; may be used when laser is unavailable
TRAP Sequence (Twin Reversed Arterial Perfusion)
- Occurs in ~1% of MC pregnancies
- One twin is acardiac/acephalic ("acardiac twin"), perfused retrogradely by the pump twin
- Risk of pump twin heart failure and hydrops
- Treatment: radiofrequency ablation (RFA) or fetoscopic laser of the acardiac twin's cord
Delivery
Mode of Delivery
- Largely determined by the presentation of Twin 1
- Twin 1 cephalic: vaginal delivery is appropriate in experienced units (internal podalic version or breech extraction for Twin 2 is acceptable)
- Twin 1 non-cephalic: Caesarean section recommended
Timing of Delivery (NICE/RCOG Guidance)
| Type | Recommended Gestation |
|---|---|
| DCDA, uncomplicated | 37 weeks |
| MCDA, uncomplicated | 36–37 weeks |
| MCMA | 32–34 weeks (due to cord entanglement) |
| Complicated by TTTS/sFGR | Individualized; often earlier |
Intrapartum
- IV access and crossmatch
- Continuous CTG monitoring of both fetuses
- Anaesthetic team on standby
- Oxytocin augmentation may be needed after delivery of Twin 1
- Active management of third stage (high PPH risk)
Higher-Order Multiples (Triplets and Beyond)
- Almost exclusively from ART
- Risks amplified proportionally (extreme prematurity, maternal morbidity)
- Multifetal pregnancy reduction (MFPR) to twins or singleton may be offered; reduces preterm birth and improves outcomes, at the cost of small miscarriage risk
- Delivery by Caesarean section is standard
Key Summary
| Feature | DCDA | MCDA | MCMA |
|---|---|---|---|
| Chorionicity | Dichorionic | Monochorionic | Monochorionic |
| Amnionicity | Diamniotic | Diamniotic | Monoamniotic |
| Main specific risk | Discordant growth | TTTS, sFGR | Cord entanglement |
| Surveillance from | 20 weeks (4-weekly) | 16 weeks (2-weekly) | 16 weeks (weekly) |
| Elective delivery | 37 weeks | 36–37 weeks | 32–34 weeks |
The single most important early step in managing any multiple pregnancy is accurate chorionicity determination in the first trimester — it underpins every subsequent surveillance and management decision.
This is a shared conversation. Sign in to Orris to start your own chat.