Acute inflammation pathology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have all the content and key diagrams. Let me compile the comprehensive answer.
Acute Inflammation - Pathology
Acute inflammation is the rapid, stereotyped response of vascularized tissue to injury, infection, or necrosis. Its purpose is to deliver leukocytes and plasma proteins to the site of damage and eliminate the offending agent. It is characterized by five cardinal signs: rubor (redness), calor (heat), tumor (swelling), dolor (pain), and functio laesa (loss of function).
Acute inflammation has three core components:
- Dilation of small vessels (increased blood flow)
- Increased permeability of the microvasculature
- Emigration of leukocytes from the microcirculation
- Robbins & Kumar Basic Pathology, p. 44
1. Vascular Reactions
Changes in Vascular Flow and Caliber
After injury, a transient vasoconstriction is followed rapidly by vasodilation, primarily of postcapillary venules, mediated mainly by histamine acting on vascular smooth muscle. This produces heat and redness (erythema).
Vasodilation is quickly followed by increased vascular permeability, with outpouring of protein-rich fluid into extravascular tissues.
The sequence:
- Vasodilation → increased blood flow
- Fluid loss + increased vessel diameter → stasis (slowed blood flow)
- Stasis → concentration of red cells → vascular congestion
- Leukocytes (principally neutrophils) accumulate along the endothelium (margination)
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 84
Exudate vs. Transudate
| Feature | Exudate | Transudate |
|---|---|---|
| Protein content | High | Low (mainly albumin) |
| Cells | Leukocytes, debris | Few or none |
| Cause | Increased vascular permeability | Osmotic/hydrostatic imbalance |
| Specific gravity | >1.020 | <1.012 |
| Context | Inflammation | Heart failure, cirrhosis, nephrotic syndrome |
Pus (purulent exudate) = neutrophils + liquefied necrotic debris + microbes.
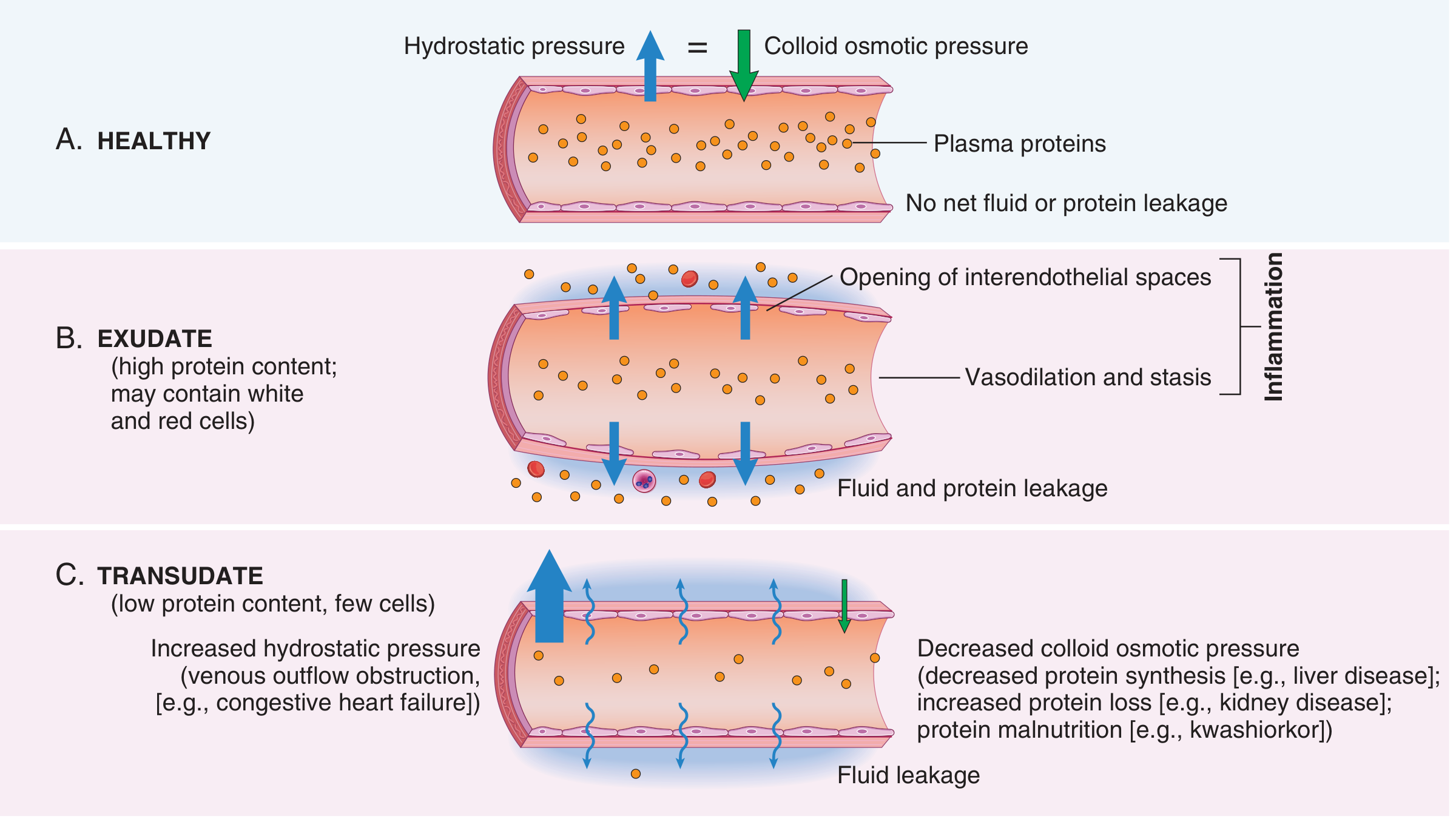
Fig. 2.2 - Robbins & Kumar Basic Pathology, p. 45
Mechanisms of Increased Vascular Permeability
The principal mechanism is contraction of endothelial cells, creating interendothelial openings (gaps), induced by histamine, bradykinin, and leukotrienes. This occurs within 15-30 minutes of mediator exposure and is typically short-lived.
In severe injury (e.g., burns), direct endothelial injury causes immediate, sustained leakage until vessels are thrombosed or repaired.
2. Leukocyte Recruitment
The journey of leukocytes from the lumen to the tissue is a multistep process:
Margination → Rolling → Adhesion → Transmigration → Chemotaxis
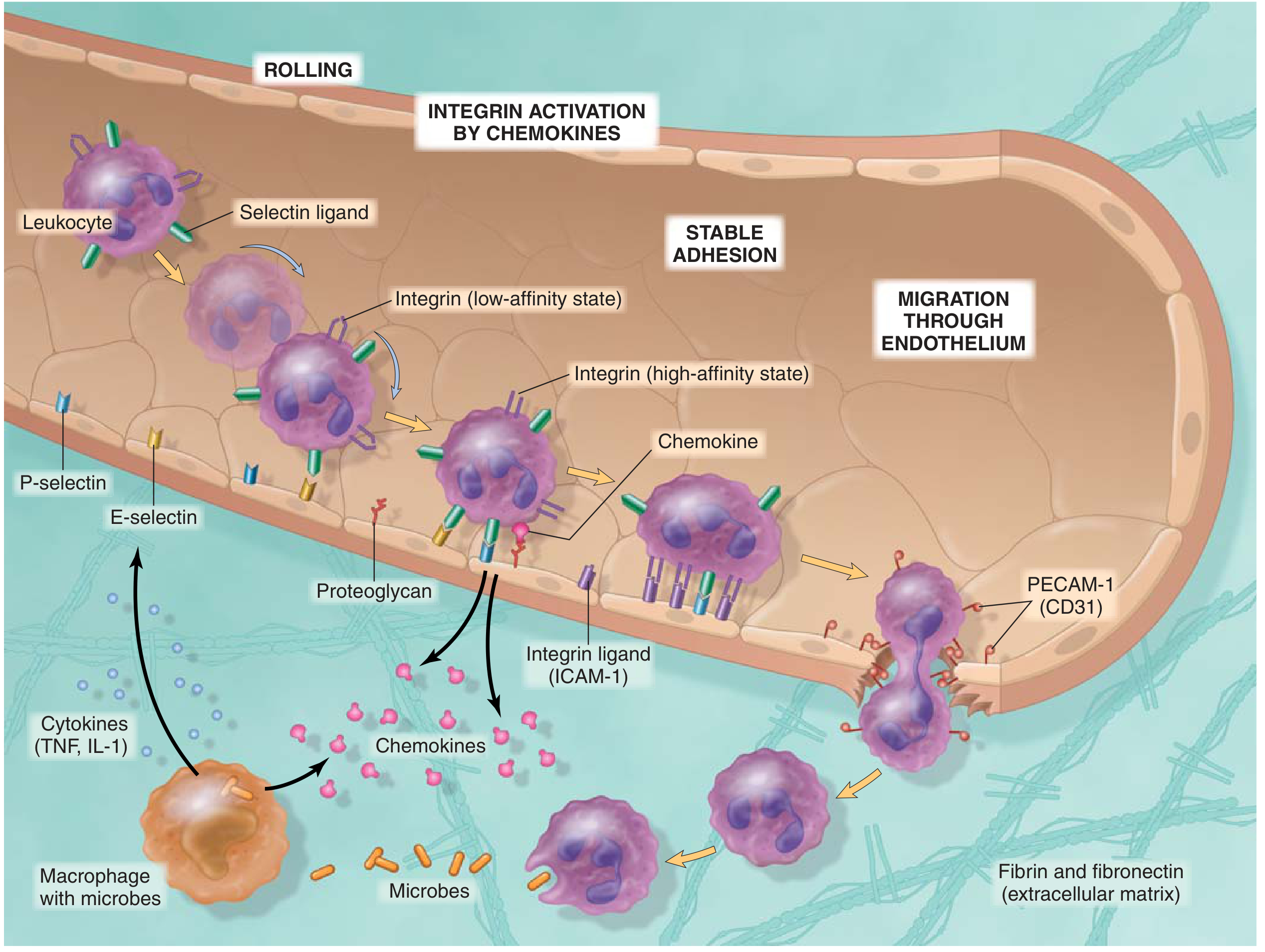
Fig. 2.3 - Robbins & Kumar Basic Pathology, p. 46
Step-by-Step:
Rolling - Mediated by selectins (E-selectin and P-selectin on endothelium; L-selectin on leukocytes). Selectins bind sialic acid-containing oligosaccharide ligands. P-selectin is stored in Weibel-Palade bodies and redistributes to the surface within minutes after histamine/thrombin stimulation.
Firm Adhesion - Chemokines produced at the injury site bind endothelial proteoglycans and activate leukocyte integrins (e.g., LFA-1, MAC-1/CD11b/CD18), switching them from low- to high-affinity state. Integrins then bind their ligands on endothelium: ICAM-1 (ligand for LFA-1 and MAC-1) and VCAM-1 (ligand for VLA-4). TNF and IL-1 upregulate expression of these endothelial ligands.
Transmigration (Diapedesis) - Leukocytes migrate through interendothelial junctions, directed by PECAM-1 (CD31) on both leukocytes and endothelial cells. They then traverse the basement membrane aided by metalloproteinases.
Chemotaxis - Movement toward chemoattractants along a concentration gradient. Key chemoattractants include:
- Bacterial products (N-formylmethionine peptides)
- Complement C5a
- Leukotriene B4 (LTB4)
- Chemokines (e.g., IL-8/CXCL8)
Neutrophils predominate in the first 6-24 hours; monocytes/macrophages replace them by 24-48 hours (neutrophils are short-lived; monocytes survive longer and proliferate in tissues).
- Robbins & Kumar Basic Pathology, pp. 46-50
3. Phagocytosis and Leukocyte Functions
Once at the site, leukocytes eliminate the offending agent through three steps:
1. Recognition and opsonization - Phagocyte receptors (mannose receptors, scavenger receptors, Fc receptors, complement receptors) bind microbes. Opsonins - IgG antibodies and C3b - greatly enhance phagocytosis.
2. Engulfment - Cytoplasmic extensions flow around the target, forming a phagosome, which fuses with a lysosomal granule to form a phagolysosome.
3. Intracellular killing - Via:
- Reactive oxygen species (ROS): NADPH oxidase converts O₂ to superoxide (O₂⁻), then H₂O₂. Myeloperoxidase converts H₂O₂ + Cl⁻ to hypochlorous acid (HOCl) - the most potent oxidant in neutrophils (the "respiratory burst"). Deficiency of NADPH oxidase causes chronic granulomatous disease.
- Reactive nitrogen species: iNOS generates nitric oxide (NO), which forms peroxynitrite (ONOO⁻), a potent microbicide.
- Lysosomal enzymes: elastase, cathepsins, lysozyme, defensins.
Neutrophil Extracellular Traps (NETs) - Activated neutrophils expel chromatin lattices coated with antimicrobial proteins (histones, elastase, MPO). NETs trap and kill extracellular bacteria and fungi but also contribute to thrombosis and tissue damage.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 89-92
4. Mediators of Inflammation
Vasoactive Amines
| Mediator | Source | Actions |
|---|---|---|
| Histamine | Mast cells, basophils, platelets | Vasodilation, increased vascular permeability; released immediately by IgE, trauma, complement C3a/C5a |
| Serotonin (5-HT) | Platelets | Similar to histamine; vasoactive |
Arachidonic Acid (AA) Metabolites (Eicosanoids)
AA is released from membrane phospholipids by phospholipase A₂ (inhibited by corticosteroids). Two key pathways:
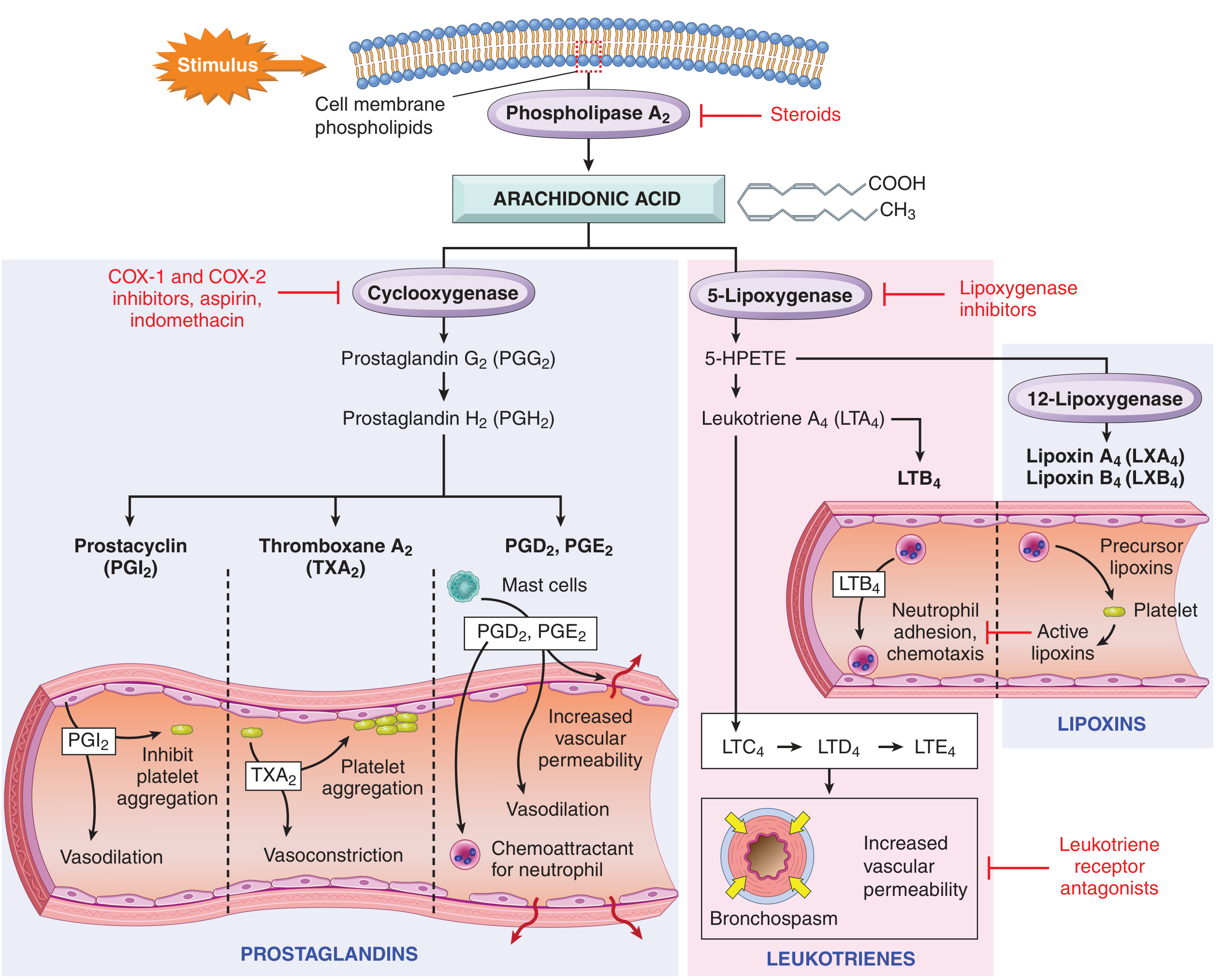
Fig. 2.6 - Robbins & Kumar Basic Pathology, p. 54
COX pathway (prostaglandins/thromboxane):
- PGE₂, PGD₂, PGI₂ → vasodilation, increased permeability, pain, fever
- TxA₂ (from platelets) → vasoconstriction, platelet aggregation
- PGI₂ (prostacyclin, from endothelium) → vasodilation, inhibits platelet aggregation
- Inhibited by aspirin/NSAIDs (aspirin irreversibly inhibits COX)
5-Lipoxygenase pathway (leukotrienes):
- LTB₄ (from neutrophils/macrophages) → potent chemotaxis, neutrophil activation
- LTC₄, LTD₄, LTE₄ (from mast cells) → intense vasoconstriction, bronchospasm, increased permeability
- Inhibited by zileuton (5-LOX inhibitor); receptor blocked by montelukast (used in asthma)
Lipoxins (from AA via 15-LOX) → suppress inflammation by inhibiting neutrophil recruitment; part of the resolution mechanism.
Cytokines and Chemokines
| Cytokine | Source | Key Actions |
|---|---|---|
| TNF | Macrophages, dendritic cells, mast cells, T cells | Endothelial activation, adhesion molecule upregulation, fever, systemic effects |
| IL-1 | Macrophages, dendritic cells, epithelial cells | Similar to TNF; major role in fever via hypothalamic COX-2 |
| IL-6 | Macrophages, other cells | Acute-phase response (hepatic protein synthesis) |
| IL-8 (CXCL8) | Macrophages, endothelium | Neutrophil chemotaxis |
| IL-17 | T lymphocytes | Recruitment of neutrophils and monocytes |
Complement System
- C3a, C5a (anaphylatoxins) → stimulate mast cell degranulation (histamine release), increased vascular permeability
- C5a → potent chemotaxis for neutrophils and monocytes; also activates lipoxygenase pathway
- C3b → opsonin, enhances phagocytosis
- C5b-9 (MAC) → direct cell lysis
Other Mediators
- Bradykinin: causes vasodilation, increased permeability, smooth muscle contraction, pain; generated by the kinin system (Hageman factor XII activates)
- Platelet-activating factor (PAF): produced by mast cells, neutrophils, platelets; causes platelet aggregation, bronchoconstriction, increased permeability
- Nitric oxide (NO): vasodilation, microbicidal
- Coagulation cascade: thrombin and fibrin degradation products are pro-inflammatory
- Robbins & Kumar Basic Pathology, pp. 51-60
5. Morphologic Patterns of Acute Inflammation
Serous Inflammation
- Outpouring of thin, protein-poor fluid into serous cavities (pleura, pericardium, peritoneum) or beneath the skin
- Example: skin blister in a burn or viral infection
- The fluid comes from plasma or from mesothelial cell secretions
Fibrinous Inflammation
- Larger vascular leaks allow fibrinogen to escape and polymerize into fibrin
- Appears as eosinophilic meshwork (threads or amorphous coagulum) histologically
- Classic example: fibrinous pericarditis ("bread-and-butter" pericardium) - seen in uremia, myocardial infarction
- Fate: fibrinolysis + macrophage clearance (resolution) OR organization → fibrosis → obliteration of pericardial space
Purulent (Suppurative) Inflammation
- Dominated by pus = neutrophils + liquefied necrotic cells + edema fluid
- Caused by pyogenic bacteria (staphylococci, streptococci)
- Abscess: localized collection of pus with central necrotic core, surrounding rim of neutrophils, outer zone of vascular congestion and repair
- Example: acute appendicitis, lung abscess in bronchopneumonia
Ulcers
- Local defect produced by sloughing of inflamed necrotic tissue on or near a surface
- Acute phase: intense neutrophilic infiltration, vascular dilation at margins
- With chronicity: fibroblastic proliferation, scarring, lymphocytes/macrophages/plasma cells
- Example: peptic ulcer (stomach/duodenum), lower limb ulcers in diabetes/vascular disease
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 99-102
6. Termination of Acute Inflammation
Active resolution mechanisms prevent excessive tissue damage:
- Short half-life of mediators; mediator synthesis ceases
- Neutrophil apoptosis is triggered once the stimulus is eliminated
- Anti-inflammatory signals are produced: lipoxins, resolvins, IL-10, TGF-β, IL-1 receptor antagonist
- Arachidonic acid is shifted toward lipoxin/resolvin production (pro-resolution)
- Macrophages efferocytose apoptotic neutrophils and switch to repair mode
- Robbins & Kumar Basic Pathology, p. 56
7. Outcomes of Acute Inflammation
| Outcome | Mechanism | Example |
|---|---|---|
| Complete resolution | Elimination of stimulus, removal of debris, restoration of normal tissue | Lobar pneumonia |
| Healing by fibrosis (scarring) | When injury is extensive or tissue lacks regenerative capacity | Myocardial infarction |
| Abscess formation | Walling off pus in a cavity | Skin abscess |
| Progression to chronic inflammation | If acute response fails to clear the agent | Viral hepatitis → chronic hepatitis |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 102; Robbins & Kumar Basic Pathology, p. 61
Quick Summary Table
| Component | Key Events | Key Mediators |
|---|---|---|
| Vascular changes | Vasodilation → stasis → exudation | Histamine, PGI₂, PGE₂, bradykinin, NO |
| Increased permeability | Endothelial contraction, interendothelial gaps | Histamine, bradykinin, LTC₄/D₄/E₄, C5a |
| Leukocyte recruitment | Margination, rolling, adhesion, transmigration | Selectins, integrins, ICAM-1, PECAM-1, chemokines |
| Chemotaxis | Directed leukocyte migration | C5a, LTB₄, IL-8, bacterial peptides |
| Phagocytosis/killing | ROS (respiratory burst), NO, lysosomal enzymes | NADPH oxidase, MPO, iNOS |
| Resolution | Lipoxins, resolvins, apoptosis of neutrophils | Lipoxins, IL-10, TGF-β |
Sources:
- Robbins & Kumar Basic Pathology, Chapter 2 (Inflammation and Repair), pp. 44-64
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 3, pp. 67-105
This is a shared conversation. Sign in to Orris to start your own chat.