Appendicitis
Reading File
search_medical_text
appendicitis etiology pathophysiology clinical presentation diagnosis
search_medical_text
appendicitis management treatment surgery complications scoring systems
search_medical_image
appendicitis imaging ultrasound CT scan findings
GradeResponse
GradeResponse
GradeResponse
Appendicitis
Overview
Appendicitis is acute inflammation of the vermiform appendix and represents the most common cause of emergency abdominal surgery worldwide. It affects approximately 7–8% of the population at some point in life, with peak incidence in the second and third decades.
Pathophysiology
The central mechanism is luminal obstruction of the appendix, most commonly by:
- Faecolith (hardened stool) — most frequent cause
- Lymphoid hyperplasia (especially in children, following viral infections)
- Tumours, foreign bodies, or parasites (less common)
Obstruction leads to bacterial overgrowth, mucosal ischaemia, transmural inflammation, and, if untreated, perforation (typically within 24–72 hours of onset).
Clinical Presentation
| Feature | Detail |
|---|---|
| Pain | Classically periumbilical at onset, migrating to right iliac fossa (RIF) over 6–12 hours |
| Anorexia | Nearly universal — its absence should raise doubt |
| Nausea/vomiting | Common, usually follows onset of pain |
| Fever | Low-grade (37.5–38.5°C); high fever suggests perforation |
| Diarrhoea/urinary symptoms | Possible if appendix is pelvic or retrocaecal |
Key Examination Signs (Bailey & Love's, p. 1360)
- McBurney's point tenderness — maximum tenderness 1/3 of the way from ASIS to umbilicus
- Rovsing's sign — palpation in LIF causes pain in RIF
- Psoas sign — extension of right hip causes pain (retrocaecal appendix)
- Obturator sign — internal rotation of right hip causes pain (pelvic appendix)
- Rebound tenderness / guarding — suggest peritoneal irritation
- Pointing sign — patient points to where pain started and migrated
Diagnosis
Laboratory
- WBC: Elevated (>10,000/mm³) in ~80% — left shift (neutrophilia) is characteristic
- CRP: Elevated; rises later but useful in delayed presentations
- Urinalysis: May show mild pyuria/haematuria (do not exclude appendicitis)
- β-hCG: Must be checked in women of reproductive age (to exclude ectopic pregnancy)
Clinical Scoring Systems
| Score | Components | Interpretation |
|---|---|---|
| Alvarado (MANTRELS) | Migration of pain, Anorexia, Nausea/vomiting, Tenderness RIF, Rebound, Elevated temp, Leukocytosis, Shift to left | ≥7 = likely appendicitis |
| Appendicitis Inflammatory Response (AIR) | Similar with CRP added | More validated in adults |
| pAAS | Paediatric variant |
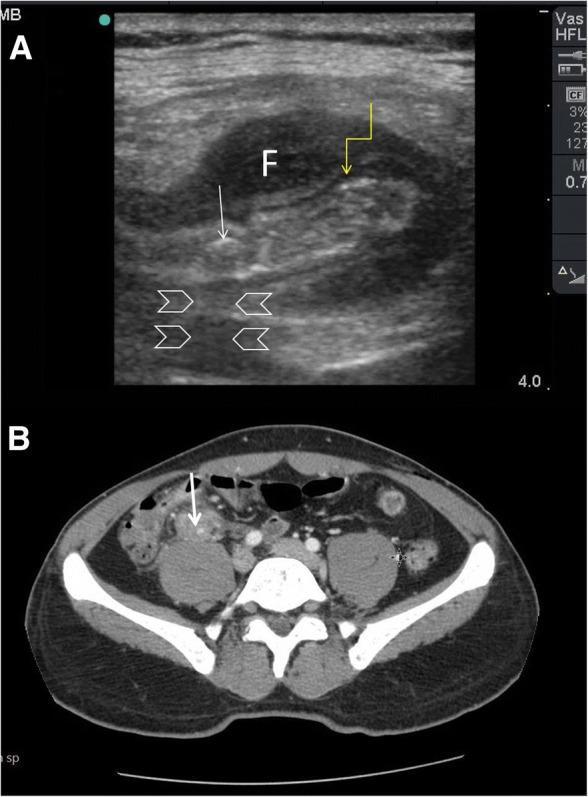
Imaging
| Modality | Findings | Use |
|---|---|---|
| Ultrasound | Non-compressible appendix >6 mm diameter, faecolith with posterior acoustic shadowing, periappendiceal fluid | First-line (no radiation); operator-dependent |
| CT abdomen/pelvis | Dilated appendix with wall enhancement, faecolith, periappendiceal fat stranding | Gold standard; sensitivity ~98% |
| MRI | Similar to CT without radiation | Preferred in pregnancy |
Differential Diagnosis
- Women: Ovarian cyst/torsion, ectopic pregnancy, PID, Mittelschmerz
- Men/Children: Mesenteric adenitis, Meckel's diverticulitis, intussusception
- All ages: Right ureteric colic, Crohn's disease, caecal carcinoma, psoas abscess, right-sided diverticulitis
Management
Preoperative Preparation (Bailey & Love's, p. 1365)
- IV fluids (target adequate urine output)
- IV antibiotics covering Gram-negative bacilli + anaerobes (e.g., ceftriaxone + metronidazole)
- VTE prophylaxis (mechanical ± pharmacological)
- Single perioperative dose of antibiotics reduces wound infection in uncomplicated cases
Surgical Treatment
- Appendicectomy is the definitive treatment — laparoscopic preferred (shorter hospital stay, less wound infection, faster recovery)
- Open appendicectomy remains valid when laparoscopy is unavailable or contraindicated
- In perforated appendicitis: therapeutic antibiotics, thorough washout; drain placement controversial
Non-operative Management
- Select uncomplicated cases (no perforation, no faecolith, low-risk patients) may be managed with IV antibiotics alone (e.g., ertapenem or ceftriaxone + metronidazole for 24–48h then oral step-down)
- Recurrence rate ~20–35% at 5 years; patients must be counselled appropriately
- Not appropriate for perforated appendicitis or appendiceal mass
Complicated Appendicitis (Abscess/Phlegmon)
- Appendiceal phlegmon: IV antibiotics first; interval appendicectomy at 6–8 weeks (debated)
- Appendiceal abscess: Percutaneous drainage + antibiotics; interval appendicectomy
Complications
| Complication | Notes |
|---|---|
| Perforation | ~20–30% at presentation; higher in extremes of age |
| Peritonitis | Local or generalised; requires urgent surgery |
| Appendiceal abscess/phlegmon | Walled-off infection |
| Portal pyaemia / liver abscess | Rare but serious |
| Post-op wound infection | Most common surgical complication |
| Stump appendicitis | Rare recurrence in residual stump after appendicectomy |
Special Populations
- Children: Perforation rates higher (thin appendiceal wall, delayed diagnosis); mesenteric adenitis is a common mimic
- Elderly: Atypical presentation common; higher perforation and mortality rates
- Pregnancy: MRI preferred for imaging; appendix displaced superiorly by gravid uterus; higher risk of preterm labour post-operatively
- Immunocompromised: May lack classic inflammatory signs; high index of suspicion required
Prognosis
- Uncomplicated appendicitis treated promptly: mortality <0.1%
- Perforated appendicitis: mortality rises to 1–5%, higher in elderly
- Laparoscopic appendicectomy is associated with faster return to normal activity and lower wound infection rates compared to open surgery
This is a shared conversation. Sign in to Orris to start your own chat.