Vitiligo treatment
Reading File
search_medical_text
vitiligo treatment management therapies
search_medical_text
vitiligo phototherapy topical agents repigmentation
search_medical_image
vitiligo skin depigmentation clinical appearance
GradeResponse
GradeResponse
GradeResponse
Vitiligo Treatment
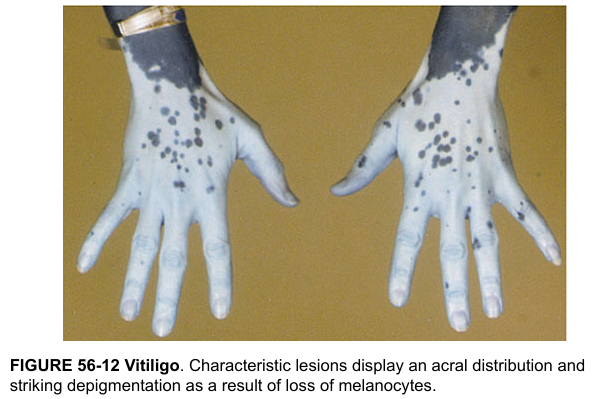
Vitiligo is an autoimmune disorder causing loss of melanocytes, resulting in well-demarcated depigmented patches. Treatment aims to halt progression and achieve repigmentation.
Goals of Treatment
- Stop active disease progression
- Repigment affected skin
- Maintain achieved repigmentation
First-Line Therapies
Topical Agents
| Agent | Details |
|---|---|
| Topical corticosteroids (TCS) | High-potency (e.g., clobetasol) for trunk/extremities; moderate-potency for face. First-line for localized disease. Monitor for skin atrophy with prolonged use. |
| Topical calcineurin inhibitors (TCIs) | Tacrolimus 0.1% or pimecrolimus 1%. Preferred for face and intertriginous areas (steroid-sparing). Safe for long-term use. |
| Ruxolitinib cream (JAK inhibitor) | FDA-approved (2022) for non-segmental vitiligo in adults/adolescents ≥12 years. JAK1/2 inhibitor targeting the IFN-γ/CXCL10 pathway. Most effective repigmentation agent to date for facial lesions. |
Phototherapy
Narrow-band UVB (NB-UVB) is the mainstay of phototherapy for vitiligo (Harrison's, p. 1712):
- Fluorescent bulbs emitting ~311 nm radiation
- Superior efficacy over broad-band UVB
- Suitable for widespread disease or lesions resistant to topicals
- 2–3 sessions/week for a minimum of 6–12 months
- Can be combined with topical agents for enhanced effect
PUVA (Psoralen + UVA):
- Oral or topical psoralen + UVA exposure
- Effective but higher risk (nausea, phototoxicity, cataract risk with oral psoralen)
- Less commonly used now that NB-UVB is available
Excimer laser (308 nm):
- Targeted phototherapy for localized lesions
- Allows high-dose UV delivery to affected patches while sparing normal skin
- Faster response than whole-body NB-UVB
Surgical Options
Reserved for stable segmental or focal vitiligo (no new lesions for ≥12 months):
| Procedure | Details |
|---|---|
| Suction blister epidermal grafting | Most widely used; good cosmetic outcomes |
| Split-thickness skin grafting | For larger areas |
| Punch grafting | Small, focal patches |
| Melanocyte-keratinocyte transplantation (MKTP) | Cultured cells; can cover large areas |
Systemic Therapies
- Oral mini-pulse corticosteroids (e.g., betamethasone 5 mg on 2 consecutive days/week): used to halt rapidly progressive disease
- Oral JAK inhibitors (ruxolitinib, baricitinib — investigational/emerging): promising phase II/III trial data for widespread disease
- Afamelanotide (MC1R agonist implant): used in combination with NB-UVB, accelerates repigmentation
Camouflage / Depigmentation
- Cosmetic camouflage (waterproof concealers, self-tanners) for psychosocial impact
- Depigmentation with monobenzone (monobenzyl ether of hydroquinone): considered only when >50% BSA is affected and repigmentation has failed — permanently depigments remaining normal skin
Special Considerations
| Factor | Guidance |
|---|---|
| Segmental vitiligo | Less responsive to medical treatment; surgical options preferred |
| Active/inflammatory vitiligo | Treat inflammation first (TCIs, TCS, systemic steroids) before surgery |
| Children | Prefer TCIs and NB-UVB; avoid prolonged high-potency TCS |
| Face/eyelids | TCIs + NB-UVB or excimer laser; avoid TCS long-term |
| Koebner phenomenon | Minimize trauma; treat wounds promptly |
Monitoring
- Assess repigmentation at 3–6 months
- Wood's lamp examination to detect early lesions and assess progress
- Screen for associated autoimmune conditions: thyroid disease (most common), type 1 diabetes, Addison's disease, alopecia areata
Key takeaway: Mild/localized disease → topical TCS or TCIs ± excimer. Moderate/widespread → NB-UVB ± topicals. Rapidly progressive → systemic mini-pulse steroids. Stable localized → surgical grafting. Ruxolitinib cream is a significant recent advance for facial non-segmental vitiligo.
This is a shared conversation. Sign in to Orris to start your own chat.