Difference between sensitivity and specificity
Reading File
search_medical_image
sensitivity specificity 2x2 contingency table diagnostic test
Upper Gastrointestinal and Ulcer Bleeding
Page 4
GradeResponse
GradeResponse
Sensitivity vs. Specificity
These are two fundamental measures of a diagnostic test's performance.
Core Definitions
| Sensitivity | Specificity | |
|---|---|---|
| Also called | True Positive Rate | True Negative Rate |
| Question answered | "If the disease IS present, how often does the test correctly say YES?" | "If the disease is NOT present, how often does the test correctly say NO?" |
| Formula | TP / (TP + FN) | TN / (TN + FP) |
| Misses | False Negatives | False Positives |
The 2×2 Table
Disease + Disease −
Test Positive | True Positive | False Positive |
Test Negative | False Negative | True Negative |
- Sensitivity = TP ÷ (TP + FN) → reads down the Disease+ column
- Specificity = TN ÷ (TN + FP) → reads down the Disease− column
Practical Mnemonics
- SnNout: High Snsitivity → a Negative result rules out disease (few false negatives)
- SpPin: High Specificity → a Positive result rules in disease (few false positives)
The Sensitivity-Specificity Trade-off
Lowering the test threshold increases sensitivity but decreases specificity (and vice versa). This trade-off is visualized on an ROC curve — the area under the curve (AUC) reflects overall test performance.
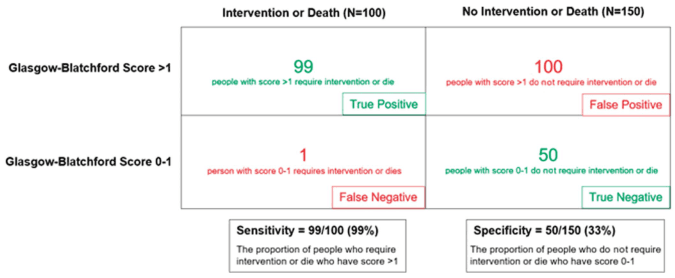
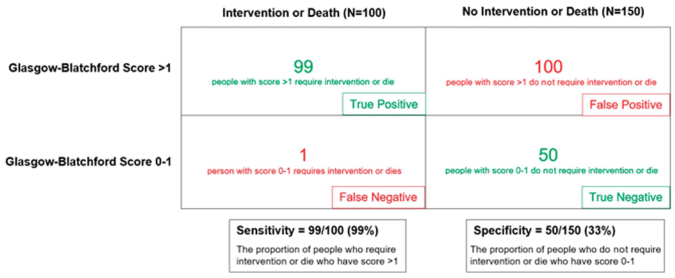
Example from clinical practice (Upper GI Bleeding guidelines, p. 4):
The Glasgow-Blatchford Score >1 has a sensitivity of 99% (misses almost no patients needing intervention) but a specificity of only 33% (many false positives). This is an acceptable trade-off when the goal is to avoid missing a serious outcome.
When to Prioritize Each
| Priority | Use High Sensitivity | Use High Specificity |
|---|---|---|
| Goal | Don't miss disease (rule out) | Confirm disease (rule in) |
| When false negatives are costly | Screening tests (e.g., HIV ELISA, cancer screening) | Confirmatory tests (e.g., HIV Western blot) |
| Consequence of error | Missing a treatable/dangerous disease | Unnecessary treatment or patient harm |
Key Takeaway
- Sensitivity is about catching all the sick — high sensitivity = few missed cases.
- Specificity is about correctly clearing the healthy — high specificity = few false alarms.
- No single test is perfect at both; the clinical context determines which matters more.
Post exposure prophylaxis for needle stick injury
search_medical_text
post exposure prophylaxis needle stick injury HIV
Harrison's Principles of Internal Medicine, Twenty First Edition
Page 5977
search_medical_text
needle stick injury PEP hepatitis B hepatitis C management
Harrison's Principles of Internal Medicine, Twenty First Edition
Page 9430
GradeResponse
GradeResponse
search_medical_text
HIV PEP regimen antiretroviral drugs preferred regimen occupational exposure
search_medical_text
hepatitis B post exposure prophylaxis HBIG vaccination needle stick occupational
Post-Exposure Prophylaxis (PEP) for Needle Stick Injury
Immediate First Aid (All Cases)
- Do NOT suck the wound
- Wash thoroughly with soap and water for several minutes
- Allow wound to bleed freely (do not squeeze)
- Apply antiseptic (povidone-iodine or 70% alcohol)
- Report to occupational health/emergency department immediately
- Document time, nature of exposure, source patient details
HIV PEP
Treat as a medical emergency — PEP must be started within 72 hours (ideally within 1–2 hours). Efficacy drops significantly with delay and is ineffective after 72 hours. (Harrison's, p. 5977)
Risk Assessment
| Factor | Increases Transmission Risk |
|---|---|
| Deep percutaneous injury | ✓ |
| Visible blood on device | ✓ |
| Device placed in source's vein/artery | ✓ |
| Advanced HIV disease / high viral load in source | ✓ |
| Hollow-bore needle vs. solid needle | ✓ (hollow > solid) |
Average risk of HIV transmission from a single needle stick from an HIV+ source: ~0.3%
Preferred PEP Regimen
3-drug combination for 28 days:
| Regimen | Drugs |
|---|---|
| Preferred | Tenofovir/Emtricitabine (TDF/FTC) + Raltegravir OR Dolutegravir |
| Alternative | TDF/FTC + Lopinavir/ritonavir |
- Duration: 28 days (full course must be completed)
- Consider drug resistance in source patient when selecting regimen
- Pregnancy/breastfeeding: consult specialist — avoid efavirenz in first trimester
Follow-Up Testing (HIV)
| Timepoint | Test |
|---|---|
| Baseline | HIV Ag/Ab (4th generation) |
| 6 weeks | HIV Ag/Ab |
| 3 months | HIV Ag/Ab |
| 6 months | HIV Ag/Ab (if source HCV+, extend to 6 months) |
Hepatitis B PEP
Response depends on the vaccination and immune status of the exposed worker:
| Exposed HCW Status | Source HBsAg+ | Source Unknown/Not Tested |
|---|---|---|
| Unvaccinated | HBIG × 1 + start HBV vaccine series | Start HBV vaccine series |
| Vaccinated, known responder (anti-HBs ≥10 mIU/mL) | No treatment needed | No treatment needed |
| Vaccinated, known non-responder | HBIG × 2 (1 month apart) OR HBIG × 1 + revaccinate | If high-risk source: treat as HBsAg+ |
| Vaccinated, unknown response | Test exposed person for anti-HBs; if inadequate → HBIG + booster | Test anti-HBs; if adequate → no Rx |
- HBIG dose: 0.06 mL/kg IM (ideally within 24 hours, up to 7 days)
- Risk of transmission per needle stick from HBsAg+ source: 6–30% (much higher than HIV)
Hepatitis C PEP
No effective PEP exists for Hepatitis C. (Harrison's, p. 9430)
- Immunoglobulin (IG) is not recommended — shown to be ineffective
- No vaccine available
- Risk per needle stick from HCV+ source: ~1.8%
Management:
- Baseline HCV antibody + ALT
- Follow-up at 4–6 weeks (HCV RNA), 3 months, and 6 months
- If HCV RNA becomes positive (acute HCV): refer for early antiviral treatment with direct-acting antivirals (DAAs) — very high cure rate (~95%+)
Summary Table
| Pathogen | PEP Available? | Agent | Start Within | Duration |
|---|---|---|---|---|
| HIV | Yes | TDF/FTC + Dolutegravir (preferred) | 72 hours | 28 days |
| Hepatitis B | Yes (if unvaccinated/non-immune) | HBIG ± vaccine | 24–48 hours | Single dose HBIG |
| Hepatitis C | No | Monitor + treat if infected | N/A | Early DAA therapy |
Special Considerations
- Source patient testing: Rapid HIV, HBsAg, HCV Ab should be obtained from the source (with consent) to guide decisions
- Unknown source: Treat based on risk assessment of the environment (e.g., needle from HIV ward = higher risk)
- Pregnancy: Avoid certain antiretrovirals; specialist consultation required
- Complete the 28-day HIV PEP course — partial courses offer incomplete protection

