Parotid gland anatomy from visharam Singh
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I have comprehensive information. Let me now compile the full answer based on Gray's Anatomy for Students (the closest equivalent available in the library to Vishram Singh's standard anatomy text).
Note: Vishram Singh's Textbook of Anatomy is not in the library's collection. The content below is sourced from Gray's Anatomy for Students - the standard anatomy reference available - which covers the same parotid anatomy as Vishram Singh's text. The topics are identical across both books.
Parotid Gland - Anatomy
Overview
The parotid gland is the largest of the three pairs of major salivary glands. It is enclosed within the split investing layer of deep cervical fascia. It produces a watery saliva containing salivary amylase, which aids in food bolus formation and oral digestion.
Position and Extent
The parotid gland lies anterior to and below the lower half of the ear, superficial, posterior, and deep to the ramus of the mandible. It occupies a shallow, triangular-shaped trench bounded by:
- Behind - the sternocleidomastoid muscle
- In front - the ramus of the mandible
- Superiorly - the external acoustic meatus and the posterior aspect of the zygomatic arch
It extends:
- Superiorly up to the zygomatic arch
- Inferiorly to the lower border of the mandible
- Anteriorly halfway across the masseter muscle
- Posteriorly covering the anterior part of the sternocleidomastoid muscle
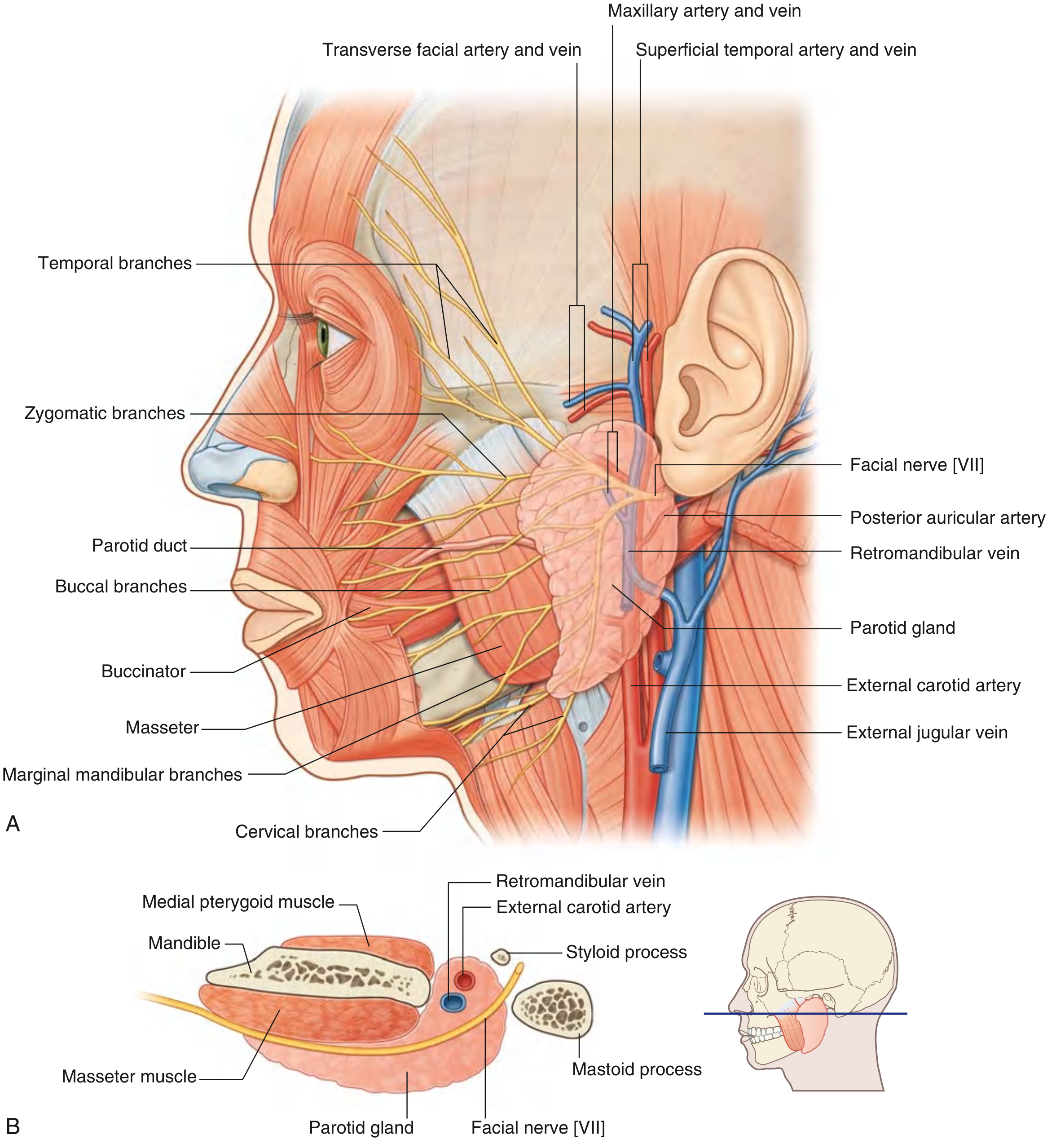
Fig. 8.65 - Parotid Gland. (A) Lateral view showing facial nerve branches, parotid duct, and vascular relations. (B) Cross-sectional view showing the gland's relationship to surrounding structures.
Parotid Duct (Stensen's Duct)
- Leaves the anterior edge of the gland, midway between the zygomatic arch and the corner of the mouth
- Crosses the face transversely over the masseter muscle
- At the medial border of masseter, turns deeply into the buccal fat pad
- Pierces the buccinator muscle
- Opens into the oral cavity adjacent to the crown of the second upper molar tooth
Important Contents and Relationships
Several major structures pass through the gland (from superficial to deep):
| Structure | Detail |
|---|---|
| Facial nerve [VII] | Most superficial; divides into upper and lower trunks inside the gland |
| Retromandibular vein | Formed inside the gland by union of superficial temporal + maxillary veins |
| External carotid artery | Deepest; divides into maxillary and superficial temporal arteries inside/near gland |
Facial Nerve [VII]
- Exits the skull via the stylomastoid foramen and enters the gland
- Divides into upper and lower trunks inside the gland
- Five terminal branch groups emerge from the upper, anterior, and lower borders:
- Temporal
- Zygomatic
- Buccal
- Marginal mandibular
- Cervical
The intimate relationship of facial nerve VII with the parotid gland makes parotidectomy a technically difficult dissection.
External Carotid Artery
- Enters at the inferior border of the gland
- Gives off the posterior auricular artery before dividing terminally into:
- Maxillary artery - passes deep to the mandible
- Superficial temporal artery - exits the upper border after giving off the transverse facial artery
Retromandibular Vein
- Formed inside the gland by union of superficial temporal and maxillary veins
- Passes inferiorly in the substance of the gland
- Divides into anterior and posterior branches just below the inferior border
Arterial Supply
The parotid gland receives its blood supply from the numerous arteries passing through its substance (branches of the external carotid artery system).
Innervation
| Type | Nerve | Pathway |
|---|---|---|
| Sensory | Auriculotemporal nerve (branch of V3/mandibular) | Via foramen ovale |
| Secretomotor (parasympathetic) | Auriculotemporal nerve (carries postganglionic fibers) | Otic ganglion → auriculotemporal nerve → gland |
| Preganglionic parasympathetic | Glossopharyngeal nerve [IX] | Lesser petrosal nerve → otic ganglion |
| Sympathetic | Postganglionic from superior cervical ganglion | Along blood vessels |
The otic ganglion - situated just inferior to the foramen ovale - is the relay station for parasympathetic secretomotor fibers to the parotid.
Clinical Notes
Parotid tumors: The commonest parotid tumors are benign (pleomorphic adenoma, adenolymphoma/Warthin's tumor) and usually involve the superficial part. Their surgical importance lies in their proximity to facial nerve branches - damage to upper branches can prevent eye closure (risking corneal injury); damage to lower branches causes facial asymmetry.
Parotid stones (sialolithiasis): Stones typically form at the main duct confluence or within the main parotid duct. Classic symptom is intense pain on salivation (easily reproduced by lemon juice). Treatment depends on stone location - anterior duct stones may be removed via buccal mucosa incision/sphincterotomy; posterior stones may require complete gland excision.
Frey's syndrome (auriculotemporal syndrome): Damage to the auriculotemporal nerve (e.g., during parotid surgery) can cause aberrant regeneration of parasympathetic fibers to sweat glands in the facial skin, leading to gustatory sweating (sweating over the cheek during eating).
- Gray's Anatomy for Students, pp. 1051-1052
This is a shared conversation. Sign in to Orris to start your own chat.