Topics to be discussed: The hypothalamic-pituitary-adrenal axis The growth hormone axis The prolactin axis Learning objectives - describes the regulatory function of the hypothalamus and pituitary explains and interprets the processes induced by the growth hormone describes and analysis the role of prolactin .explain
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content for all three learning objectives. Let me compile the full educational response.
The Hypothalamic-Pituitary Axes: A Comprehensive Guide
Overview: The Hypothalamus and Pituitary as Regulatory Masters
The hypothalamus and pituitary gland form a master regulatory system that coordinates nearly all endocrine activity in the body. The hypothalamus sits at the base of the brain and releases small regulatory peptides into the hypothalamo-hypophyseal portal system - a specialized blood supply that carries these hormones directly to the anterior pituitary. This arrangement allows the hypothalamus to either stimulate or inhibit pituitary hormone release without those signals entering the general circulation.
The anterior pituitary contains five main cell types, each producing distinct hormones under hypothalamic control:
| Cell Type | % of Pituitary | Hypothalamic Regulator | Hormone Produced | Main Target |
|---|---|---|---|---|
| Somatotrophs | 45-50% | Stimulation: GHRH, ghrelin; Inhibition: somatostatin | Growth Hormone (GH) | Liver, muscle, bone, cartilage, adipose tissue |
| Thyrotrophs | 5% | Stimulation: TRH | TSH | Thyroid gland |
| Lactotrophs | 10-30% | Stimulation: TRH; Inhibition: dopamine | Prolactin (PRL) | Mammary gland |
| Gonadotrophs | 10% | Stimulation: GnRH | LH, FSH | Gonads |
| Corticotrophs | 15-20% | Stimulation: CRH, AVP | ACTH | Adrenal cortex |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Table 56.1
1. The Hypothalamic-Pituitary-Adrenal (HPA) Axis
Structure and Signalling Cascade
The HPA axis is the body's primary stress-response system. The cascade flows as follows:
Hypothalamus → CRH + AVP → Anterior Pituitary → ACTH → Adrenal Cortex → Cortisol → Negative Feedback
Step 1 - Hypothalamic input: Corticotrophin-releasing hormone (CRH) and arginine vasopressin (AVP) are both synthesized in the paraventricular nucleus of the hypothalamus. CRH provides the basal drive for ACTH secretion, while AVP acts synergistically with CRH and adds peaks during acute stress. Both reach the anterior pituitary via short portal vessels.
Step 2 - Pituitary response: CRH binds to its receptor (CRH-R) on corticotroph cells. AVP binds to V2 receptors. Both signals converge to stimulate production and cleavage of the pro-hormone pro-opiomelanocortin (POMC) into ACTH. Because ACTH is derived from POMC, excess ACTH production also generates alpha-MSH and other POMC-derived peptides - explaining the hyperpigmentation of skin seen in conditions of ACTH excess (e.g. Addison's disease).
Step 3 - Adrenal output: ACTH binds to its receptor MC2R on adrenal cortex cells and stimulates synthesis and release of cortisol (and to a lesser extent aldosterone and androgens). Cortisol then acts on glucocorticoid (GC) receptors throughout the body.
Step 4 - Negative feedback: Cortisol feeds back to inhibit both the hypothalamus (reducing CRH/AVP) and the pituitary (reducing ACTH) - the classic long-loop negative feedback. At peripheral tissues, cortisol undergoes interconversion with cortisone via the enzyme 11-beta hydroxysteroid dehydrogenase (11HSD1 and 2), allowing fine local regulation of glucocorticoid activity.
The HPA Axis Diagram
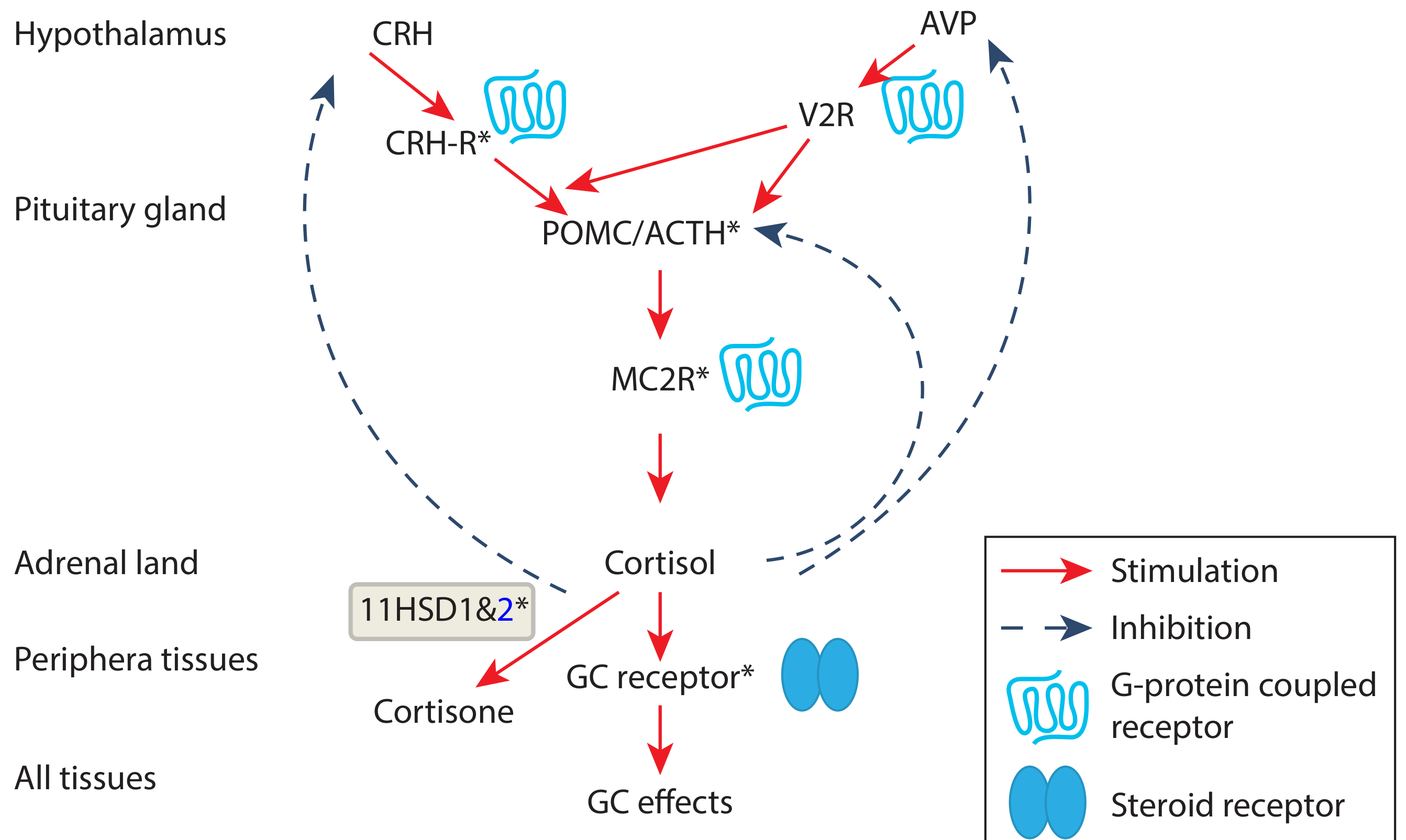
Figure: The HPA axis. CRH stimulates corticotrophs to produce ACTH (from POMC). ACTH binds MC2R at the adrenal cortex to stimulate cortisol. Cortisol inhibits both pituitary and hypothalamus (dashed blue arrows = inhibition; red arrows = stimulation). 11HSD1/2 enzymes in peripheral tissues interconvert cortisol and cortisone. - Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Fig. 56.9
Key Physiological Features
Circadian rhythm: The HPA axis displays a prominent circadian pattern. Cortisol and ACTH levels peak in the early morning and gradually fall throughout the day, reaching near-undetectable levels at night. ACTH also has a superimposed pulsatile release pattern layered on top of this rhythm.
Stress response: Virtually all types of stress - physical, emotional, or metabolic - cause immediate, marked rises in ACTH and cortisol. This is the basis of the stress cortisol response that mobilizes energy, suppresses inflammation, and prepares the body for fight-or-flight.
Clinical significance: If the HPA axis is compromised (e.g. after prolonged exogenous glucocorticoid therapy), the body cannot mount an adequate cortisol response during stress. In such patients, cortisol replacement is life-saving during infections or surgery. The standard approach is:
- For infection: double the normal glucocorticoid replacement dose
- For surgery: 100 mg IM hydrocortisone every 8 hours for 24 hours, then taper
Laboratory assessment: A morning serum cortisol > 11-15 μg/dL (303-414 nmol/L) suggests an intact HPA axis. Low or equivocal levels prompt the cosyntropin (Synacthen) stimulation test - 250 μg IV/IM, with cortisol measured at 30 and 60 minutes. The insulin tolerance test (ITT) remains the definitive test of the entire HPA axis, though it is contraindicated in patients over 70 years, or those with cardiac disease or seizures.
- Tietz Textbook of Laboratory Medicine, 7th Edition; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
2. The Growth Hormone (GH) Axis
Structure and Chemistry
GH is a 191-amino acid polypeptide synthesized by somatotroph cells, which make up 40-50% of all anterior pituitary cells. The existence of a growth-promoting hormone was first proposed by Cushing in the early 1910s; the hormone itself was isolated in 1956.
Hypothalamic regulators:
- GHRH (Growth Hormone Releasing Hormone) and ghrelin - stimulate GH release
- Somatostatin (SST) - inhibits GH release
GH secretion is pulsatile, with the largest pulses occurring during deep (slow-wave) sleep. Levels are also elevated by exercise, hypoglycaemia, fasting, stress, and high protein meals.
Cellular Mechanism of Action
GH binds to the GH receptor (GHR), a member of the type I cytokine receptor family. GH binding causes receptor dimerisation, activating Janus Kinase 2 (JAK2), which in turn activates the STAT (Signal Transducer and Activator of Transcription) pathway. This JAK2-STAT signalling cascade drives gene transcription for growth, metabolic effects, and IGF-1 production.
Metabolic and Growth Effects
GH exerts effects both directly and indirectly via Insulin-Like Growth Factor-1 (IGF-1), which is produced mainly by the liver in response to GH:
| Effect | Detail |
|---|---|
| Protein synthesis | Facilitates amino acid transport and incorporation |
| Fat mobilisation | Mobilises free fatty acids from adipose tissue (lipolysis) |
| Glucose metabolism | Decreases glucose uptake by cells; increases gluconeogenesis (anti-insulin effect) |
| Bone growth | Stimulates elongation at growth plates of long bones during childhood |
| Soft-tissue growth | Regulates growth of muscle, connective tissue, and organs |
| Cell turnover and repair | General anabolic effects throughout the body |
Negative feedback loop: Elevated IGF-1 and GH itself feed back to the hypothalamus (increasing somatostatin, decreasing GHRH) and directly to the pituitary to suppress further GH release.
Clinical Consequences of GH Excess
The target of GH excess depends on whether the epiphyseal (growth) plates are open or fused:
- In children (open plates): Excess GH causes gigantism - overly increased linear bone length
- In adults (fused plates): Elongation is no longer possible, so bones widen instead. This causes acromegaly, characterised by:
- Prominent facial changes and enlargement of hands and feet
- Soft-tissue swelling of internal organs (heart, bowels, liver)
- Cartilaginous enlargement causing rheumatological problems
- Altered laryngeal anatomy with deepening of the voice
- Enlargement of paranasal sinuses (especially frontal sinuses)
- Jaw enlargement with prognathism and malocclusion
GH deficiency in children causes growth failure and short stature. In adults it causes fatigue, reduced lean body mass, increased fat mass, and reduced quality of life.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
3. The Prolactin (PRL) Axis
Structure and Unique Regulation
Prolactin is produced by lactotroph cells (10-30% of anterior pituitary cells). It is unique among anterior pituitary hormones in one important way: the hypothalamus exerts a primary inhibitory influence on prolactin, rather than stimulatory. This means that cutting the pituitary stalk or damaging the hypothalamus causes prolactin levels to RISE, not fall.
Regulation:
| Factor | Effect on PRL | Mechanism |
|---|---|---|
| Dopamine (from hypothalamus) | Inhibits (primary control) | Acts on D2 receptors on lactotrophs |
| TRH | Stimulates | Direct stimulation of lactotrophs |
| Vasoactive intestinal peptide (VIP) | Stimulates | Direct effect |
| Estrogen | Stimulates | Stimulates PRL transcription; promotes lactotroph proliferation |
| Suckling/nipple stimulation | Stimulates | Neural reflex arc |
| Stress, exercise | Stimulates | Hypothalamic |
Receptor Signalling
Prolactin binds to the prolactin receptor, a member of the type I cytokine receptor family (the same superfamily as the GH receptor). Janus Kinase-2 (JAK2) mediates prolactin's intracellular effects. Notably, the prolactin receptor also serves as the receptor for placental lactogens - hormones synthesized during pregnancy.
Physiological Roles of Prolactin
- Lactation (primary function):
- PRL levels begin rising from the 5th week of pregnancy and peak at parturition
- During pregnancy, high estrogen and progesterone inhibit actual milk secretion despite high PRL
- After delivery, the drop in placental estrogen and progesterone disinhibits the milk ejection response to suckling
- Basal PRL returns to normal within weeks of delivery, but each nursing episode triggers a transient PRL surge that maintains milk production
- Inhibition of the gonadal axis:
- Prolactin suppresses reproductive function by inhibiting kisspeptin release from hypothalamic kisspeptin neurons, which normally drive GnRH pulsatility
- This explains why breastfeeding women commonly experience amenorrhoea (lactational amenorrhoea)
- Hyperprolactinaemia in non-pregnant individuals causes hypogonadism, menstrual irregularities, and infertility
- Sexual function:
- Prolactin counteracts the pro-arousal effects of dopamine on sexual arousal circuits
- This explains the decreased libido commonly reported by patients with hyperprolactinaemia
- Immune modulation:
- PRL receptors are found on lymphocytes, implicating prolactin in immune regulation
- Circadian pattern:
- PRL secretion gradually declines during the day and rises overnight, reaching its peak in the early morning
Hyperprolactinaemia - Causes and Diagnosis
Because dopamine normally suppresses prolactin, anything that blocks dopamine will raise PRL:
Drug causes (dopamine blockade):
- Antipsychotics (haloperidol, risperidone, paliperidone) - PRL typically 20-70 pg/mL
- Antiemetics (metoclopramide, domperidone)
- Cyclic antidepressants (clomipramine)
- Opioids (methadone, morphine) - via mu receptor activation
- Verapamil, cocaine
Non-drug causes:
- Prolactinoma (most common pituitary tumour) - macro: 200 to >10,000 pg/mL; micro: 20-250 pg/mL
- Hypothyroidism (increased TRH stimulates lactotrophs)
- Pituitary stalk compression ("stalk effect") - prevents dopamine reaching lactotrophs; PRL 5x upper limit
- Pregnancy (estrogen-driven) - 20-500 pg/mL
- Chronic renal failure, cirrhosis - decreased clearance
- PCOS, herpes zoster of chest, thoracic surgery
Pattern of PRL elevation:
- Stress alone: up to 2x upper limit
- Stalk effect: up to 5x
- Drugs or microadenoma: 5-10x
- Large macroadenoma: 10-100x or more
Treatment: Dopamine agonists (cabergoline or bromocriptine) are first-line for prolactinomas - they are highly effective at both reducing prolactin levels and shrinking tumour size. Prolactinomas can be part of Multiple Endocrine Neoplasia type 1 (MEN1) syndrome.
- Goldman-Cecil Medicine International Edition; Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Integrated Summary: The Three Axes Side by Side
| Feature | HPA Axis | GH Axis | Prolactin Axis |
|---|---|---|---|
| Hypothalamic driver | CRH + AVP (stimulatory) | GHRH + ghrelin (stimulatory); somatostatin (inhibitory) | Dopamine (inhibitory - unique!) |
| Pituitary cell | Corticotroph | Somatotroph | Lactotroph |
| Pituitary hormone | ACTH | GH | Prolactin |
| Primary target | Adrenal cortex | Liver, bone, muscle | Mammary gland; gonads |
| Key effector | Cortisol | IGF-1 | Direct action |
| Feedback | Cortisol → hypothalamus + pituitary (long-loop) | IGF-1 + GH → hypothalamus + pituitary | Prolactin itself has weak feedback; dopamine dominates |
| Circadian peak | Early morning | Deep sleep | Early morning |
| Excess state | Cushing's syndrome (↑cortisol) | Gigantism (child) / Acromegaly (adult) | Hyperprolactinaemia / Prolactinoma |
| Deficiency state | Addison's / adrenal crisis | Growth failure / GH deficiency in adults | Failure of lactation |
Key Learning Points:
- The hypothalamus regulates the anterior pituitary via releasing/inhibiting hormones delivered through the portal blood system
- CRH + AVP → ACTH → cortisol with negative feedback from cortisol; circadian rhythm peaks in early morning
- GH acts via JAK2-STAT pathway, promotes anabolism, lipolysis, and anti-insulin effects; excess causes gigantism or acromegaly depending on whether growth plates are open
- Prolactin is uniquely under tonic inhibition by dopamine; its main roles are lactation, gonadal suppression (via kisspeptin inhibition), and immune modulation; any disruption of dopamine delivery raises prolactin
This is a shared conversation. Sign in to Orris to start your own chat.