AFP surveillance and differential diagnosis
Reading File
search_medical_text
AFP alpha-fetoprotein surveillance hepatocellular carcinoma screening guidelines
search_medical_text
alpha-fetoprotein elevated differential diagnosis causes
search_medical_image
AFP hepatocellular carcinoma surveillance algorithm
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive overview of AFP surveillance and differential diagnosis.
Alpha-Fetoprotein (AFP): Surveillance & Differential Diagnosis
What Is AFP?
AFP is a glycoprotein produced primarily by the fetal liver and yolk sac. In adults, serum levels are normally < 10 ng/mL. Elevation can reflect hepatocellular malignancy, germ cell tumors, or physiologic/benign hepatic processes.
AFP Surveillance: Who, When, and How
Indications for Surveillance
AFP is used in combination with hepatic ultrasound (US) every 6 months for HCC surveillance. Target populations include:
| Population | Rationale |
|---|---|
| Cirrhosis from any cause | High baseline HCC risk |
| Chronic hepatitis B (with or without cirrhosis) | HBV integrates into host DNA, enabling HCC even without cirrhosis |
| Chronic hepatitis C with F3–F4 fibrosis (treated or untreated) | Residual risk persists even after SVR in advanced fibrosis |
| HIV-positive patients with any of the above | Coinfection accelerates fibrosis progression |
(Primary Care Guidance for Persons With HIV, p. 29; Management of HCC, p. 3)
Surveillance Protocol
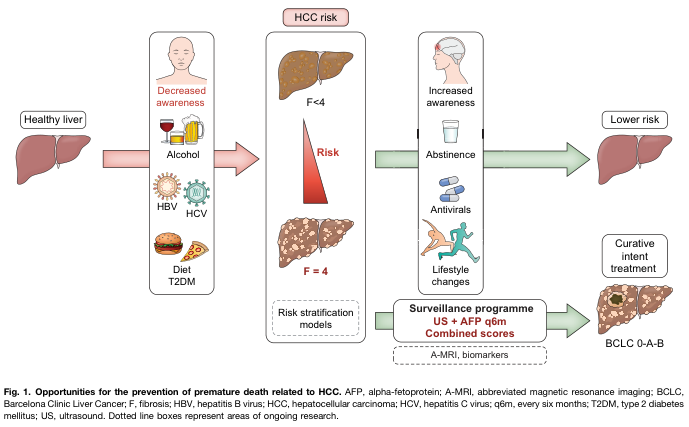
- Modality: Ultrasound + AFP every 6 months is the standard
- Emerging adjuncts: Combined risk scores (e.g., GALAD score), abbreviated MRI (A-MRI), and novel serum biomarkers (AFP-L3, DCP/PIVKA-II) are under active investigation
- AFP alone is insufficient — sensitivity for early HCC is only ~40–60%; US alone misses ~20% of nodules in cirrhotic livers; the combination improves detection
BCLC Staging Threshold for Curative Intent
Early detection via surveillance targets BCLC 0/A (very early/early stage), where resection, ablation, and transplantation offer curative potential.
Differential Diagnosis of Elevated AFP
Elevated AFP does not equal HCC. A structured differential is essential.
Malignant Causes
| Condition | AFP Level | Notes |
|---|---|---|
| Hepatocellular carcinoma (HCC) | Often >400 ng/mL in advanced disease; early HCC can be <20 | AFP >400 has ~95% specificity but low sensitivity |
| Hepatoblastoma | Markedly elevated | Pediatric tumor; most common malignant liver tumor in children <5 |
| Yolk sac tumor (endodermal sinus tumor) | Markedly elevated | Produced by >90% of yolk sac tumors (Paediatric Urology, p. 21) |
| Mixed germ cell tumor / teratoma | Moderately elevated | Teratomas produce AFP but less than yolk sac tumors |
| Gastric carcinoma with hepatoid differentiation | Variable | Rare; mimics HCC biochemically |
| Intrahepatic cholangiocarcinoma | Occasionally mildly elevated | Usually CEA/CA19-9 predominant |
Benign / Physiologic Causes
| Condition | Typical AFP |
|---|---|
| Pregnancy | Rises from week 10; maternal serum AFP used in prenatal screening (neural tube defects, Down syndrome) |
| Neonates / infants | AFP is normally very high at birth; takes up to 12 months to fall to adult values (<10 ng/mL) (Paediatric Urology, p. 21) |
| Acute hepatitis (especially viral) | Mild–moderate elevation due to hepatocyte regeneration |
| Chronic hepatitis / cirrhosis (non-HCC) | Low-level persistent elevation; complicates interpretation |
| Alcoholic liver disease | Mild elevation |
| Primary biliary cholangitis | Occasionally mildly elevated |
Diagnostic Approach to an Elevated AFP
Elevated AFP (>10 ng/mL)
│
├─ Clinical context: pediatric patient?
│ └─ Yes → Consider yolk sac tumor, hepatoblastoma, teratoma
│ (adjust for age-appropriate reference ranges — normal in infants)
│
├─ Pregnancy? → Interpret with gestational-age nomograms
│
├─ Adult, known cirrhosis / chronic liver disease
│ └─ Ultrasound → if nodule detected:
│ └─ Multiphasic CT or MRI with contrast → LI-RADS classification
│ └─ LI-RADS 4/5 → biopsy or proceed to treatment per BCLC
│
├─ Adult, no liver disease
│ └─ AFP >200–400 ng/mL → imaging for HCC; also consider GCT
│ └─ Testicular/ovarian exam + scrotal US (if male)
│ Tumor markers: β-hCG, LDH (for GCT characterization)
│
└─ Mildly elevated AFP (<20–50 ng/mL)
└─ Repeat in 3–6 months; evaluate for active hepatitis, NAFLD
Key Cutoffs and Interpretive Caveats
| AFP Level | Interpretation |
|---|---|
| < 10 ng/mL | Normal adult reference |
| 10–20 ng/mL | Borderline — monitor; evaluate for active liver disease |
| 20–200 ng/mL | Nonspecific; requires imaging correlation |
| > 200–400 ng/mL | High suspicion for HCC or GCT in appropriate context |
| > 400 ng/mL | Strongly suggestive of HCC (~95% specificity) |
| Very high (thousands) | HCC, yolk sac tumor, hepatoblastoma |
AFP Variants and Newer Biomarkers
- AFP-L3 (lectin-reactive AFP): >10–15% of total AFP suggests malignant transformation even at low total AFP levels; useful when total AFP is borderline
- DCP / PIVKA-II (des-gamma-carboxyprothrombin): Complementary to AFP; elevated in HCC; less affected by viral hepatitis flares
- GALAD score: Combines Gender, Age, AFP-L3, AFP, and DCP — outperforms AFP alone for early HCC detection, particularly in non-alcoholic fatty liver disease
Summary
AFP surveillance (US + AFP q6 months) is the standard of care for at-risk populations (cirrhosis, chronic HBV, advanced HCV fibrosis). However, AFP must always be interpreted in clinical context — elevation is nonspecific and can reflect hepatocellular regeneration, germ cell tumors, or physiologic states (neonates, pregnancy). A rising AFP trend or AFP >200–400 ng/mL mandates prompt imaging and specialist referral.
This is a shared conversation. Sign in to Orris to start your own chat.