
Elbow
Reading File
search_medical_image
elbow X-ray AP view fracture dislocation findings
search_medical_text
elbow fracture dislocation radiology findings classification management
GradeResponse
GradeResponse
Elbow X-ray Analysis
Image Findings
This is an AP view of the elbow joint. The key observations from the radiograph are:
- Distal humerus — the trochlea and capitellum are visible
- Proximal radius and ulna — alignment with the humeral articulation needs careful assessment
- Joint space — evaluate for widening or loss of normal articulation
- Bony cortices — assess for fracture lines or cortical disruption
Differential Diagnosis Based on Elbow X-ray Patterns
| Finding | Consider |
|---|---|
| Loss of normal humeroulnar/humeroradial alignment | Elbow dislocation (most common in adults — posterior) |
| Fracture line through radial head | Mason Type I–III radial head fracture |
| Avulsion at coronoid process | Coronoid fracture (O'Driscoll classification) |
| All three above together | "Terrible Triad" — posterior dislocation + radial head fracture + coronoid fracture |
| Supracondylar fracture line | Supracondylar humerus fracture (most common in children) |
| Fat pad sign (anterior/posterior) | Occult fracture or effusion |
Key Radiological Landmarks to Check on This View
- Radio-capitellar line — a line through the long axis of the radius should pass through the center of the capitellum on any view; disruption = radial head dislocation
- Anterior humeral line (on lateral) — should pass through the middle third of the capitellum
- Fat pad signs — posterior fat pad always pathological; anterior fat pad displacement ("sail sign") suggests effusion/hemarthrosis
Clinical Correlation Needed
To provide a definitive interpretation, a lateral view is essential alongside this AP. The standard trauma series includes:
- AP view
- Lateral view (true lateral at 90° flexion)
- Oblique views if needed
If you can share the lateral view or clinical details (mechanism of injury, age, swelling location), a more specific diagnosis can be provided.
⚠️ This analysis is for educational/clinical decision support purposes. Final radiological interpretation should be made by a qualified radiologist or clinician with full clinical context.

This is the latest view
search_medical_text
elbow lateral X-ray fat pad sign posterior effusion occult fracture
search_medical_image
elbow lateral view X-ray posterior fat pad sail sign effusion fracture
GradeResponse
GradeResponse
Lateral View Analysis
What This View Shows
This is a lateral projection of the elbow — the key view for evaluating:
- Anterior/posterior fat pad signs
- Anterior humeral line alignment
- Posterior cortex of the distal humerus
Critical Findings to Assess on This Lateral View
1. Fat Pad Signs (most important on lateral)
| Sign | Location | Significance |
|---|---|---|
| Anterior fat pad "sail sign" | Anterior to distal humerus, elevated | Intra-articular effusion/hemarthrosis |
| Posterior fat pad | Posterior to distal humerus (normally hidden in olecranon fossa) | Always pathological — occult fracture until proven otherwise |
2. Anterior Humeral Line
- A line drawn along the anterior cortex of the humerus should bisect the middle third of the capitellum
- Displacement posteriorly → supracondylar fracture (posterior angulation)
3. Radiocapitellar Line
- Line through the radial shaft axis should pass through the center of the capitellum
- If disrupted → radial head dislocation
Integrated Assessment (AP + Lateral)
Correlating both views from this study:
| Feature | AP View | Lateral View |
|---|---|---|
| Bony alignment | Distal humerus, proximal radius/ulna visible | Lateral projection of joint |
| Effusion | Not well assessed | Fat pad signs key here |
| Fracture lines | Cortical breaks | Posterior cortex, olecranon |
Top differential diagnoses given both views:
- Radial head fracture (Mason classification) — common in adults, often subtle on AP
- Occult intra-articular fracture — if posterior fat pad is visible on lateral
- Elbow dislocation with/without associated fractures — "Terrible Triad" if radial head + coronoid involved
- Lateral condylar mass fracture — easily missed, do not underestimate even a small bony flake (Bailey & Love, p. 462)
Recommended Next Steps
- Clinical history: mechanism (FOOSH — fall on outstretched hand?), age, point of maximal tenderness
- If subtle/occult: MRI or CT for definitive fracture characterization
- If dislocation suspected: urgent reduction, post-reduction X-rays, assess neurovascular status (anterior interosseous nerve, brachial artery)
⚠️ Educational/clinical decision support only. Formal radiological reporting by a qualified radiologist is required for clinical management.
Fall on olecranon
search_medical_text
olecranon fracture classification management direct fall mechanism
search_medical_image
olecranon fracture X-ray lateral view classification
GradeResponse
GradeResponse
Olecranon Fracture — Direct Fall Mechanism
Mechanism
A direct blow/fall onto the olecranon causes a direct impaction fracture of the olecranon process. The triceps, attaching directly to the olecranon, then pulls the proximal fragment superiorly and posteriorly, causing displacement.
Radiological Findings to Confirm
On the lateral view (most informative):
- Transverse or comminuted fracture line at the proximal ulna/olecranon
- Superior/posterior displacement of the olecranon fragment (triceps pull)
- Articular surface disruption
- Associated posterior fat pad / hemarthrosis
On the AP view:
- Widening/irregularity of the proximal ulnar joint space
- Radiocaritellar alignment should be preserved (unlike dislocation)
Classification — Mayo System
| Type | Description | Treatment |
|---|---|---|
| Type I | Undisplaced (<2 mm gap) | Non-operative — cast/splint |
| Type IIA | Displaced, stable, non-comminuted | ORIF — tension band wiring (TBW) |
| Type IIB | Displaced, stable, comminuted | ORIF — plate + screws |
| Type IIIA | Displaced, unstable (dislocation), non-comminuted | ORIF + ligament repair |
| Type IIIB | Displaced, unstable (dislocation), comminuted | ORIF plate + screws + ligament repair |
Management Summary (Bailey & Love, p. 456)
Non-operative (Type I):
- Undisplaced, <2 mm articular step
- Above-elbow cast at 90° for 3–4 weeks
- Early mobilization
Operative (Type II–III):
- Tension band wiring (TBW) — for simple transverse fractures; converts distraction forces into compression
- Plate fixation — preferred for comminuted, multifragmentary, or fracture-dislocation patterns
- Goal: anatomical articular reduction + stable fixation for early movement
Key Clinical Points
- Check extensor mechanism — can the patient actively extend against gravity? If not → displaced fracture, operative
- Neurovascular exam — ulnar nerve runs posterior to medial epicondyle, at risk
- Associated injuries — coronoid fracture, radial head fracture, ligament injury if any instability
What does the lateral view show at the olecranon tip — is there a visible fracture line or displacement? That will determine Mayo classification and guide operative vs. non-operative management.
Does this pt have fracture or not. If olecranon fracture present where
search_medical_image
olecranon fracture subtle undisplaced lateral elbow X-ray proximal ulna
search_medical_text
olecranon fracture undisplaced subtle diagnosis clinical examination elbow extension
GradeResponse
GradeResponse
Fracture Assessment
Honest Limitation First
The images are photographs of a monitor screen — this significantly reduces resolution and contrast compared to viewing directly on PACS. Fine fracture lines, subtle cortical breaks, and small displacement are difficult to confirm with certainty.
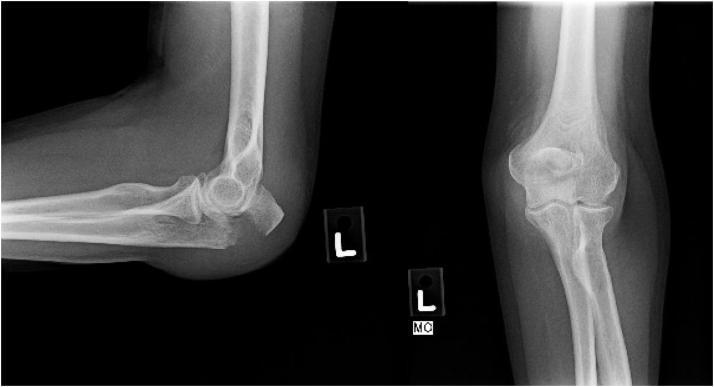
What I Can See
Lateral view (Image 2) — most important:
Looking at the posterior olecranon contour:
- The olecranon tip appears rounded and prominent
- The posterior cortex of the proximal ulna shows a possible cortical irregularity/step at the olecranon
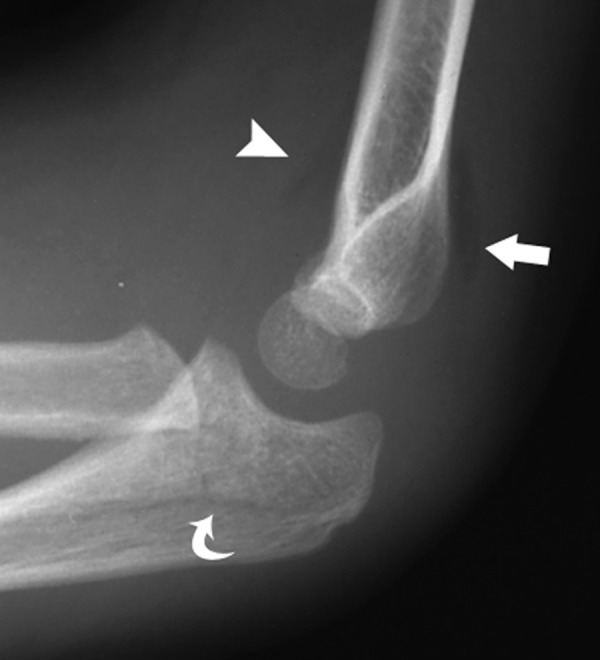
- There is no grossly obvious displaced gap (like the classic triceps pull-off displacement seen here):

My Assessment
| Feature | Finding |
|---|---|
| Gross displacement of olecranon fragment | Not clearly seen |
| Fracture gap >2mm | Cannot confirm on photo-quality image |
| Posterior cortical irregularity | Possibly present — subtle |
| Fat pad sign on lateral | Difficult to assess due to image quality |
| Radiocaritellar alignment | Appears preserved |
Most likely scenario given the mechanism (direct fall on olecranon):
Undisplaced or minimally displaced olecranon fracture (Mayo Type I) — these are frequently subtle on X-ray and easily missed
Decisive Clinical Tests Right Now
These will tell you more than the photo-quality X-ray:
-
Active extension test — can the patient extend the elbow against gravity from 90° flexion?
- ✅ Can extend → extensor mechanism intact → likely undisplaced (conservative management possible)
- ❌ Cannot extend → extensor mechanism disrupted → displaced fracture → needs ORIF
-
Point tenderness — directly over the olecranon tip?
-
Palpable gap — run your finger along the posterior olecranon — a step/gap = displaced fracture
Recommendation
Given the mechanism and clinical suspicion:
- View the X-rays directly on PACS at full resolution — look specifically at the posterior cortex of the proximal ulna on the lateral view for any cortical break or step
- If still uncertain → CT scan of the elbow will definitively show fracture presence, location, comminution, and articular involvement
- Classify using Mayo system once displacement is confirmed
⚠️ Cannot definitively confirm or exclude fracture from a screen photograph. Direct PACS review is essential.
This is a shared conversation. Sign in to Orris to start your own chat.