Cardiac conduction disorder
Reading File
search_medical_text
cardiac conduction disorders classification pathophysiology ECG findings
search_medical_text
heart block bundle branch block diagnosis management treatment
search_medical_image
cardiac conduction system ECG heart block bundle branch block
GradeResponse
GradeResponse
GradeResponse
Cardiac Conduction Disorders
Cardiac conduction disorders encompass a spectrum of abnormalities in the generation or propagation of electrical impulses through the heart's specialized conduction system. They range from benign incidental findings to life-threatening emergencies requiring urgent intervention.
Anatomy of the Conduction System
The normal cardiac conduction pathway:
SA Node → AV Node → Bundle of His → Right & Left Bundle Branches → Purkinje Fibers → Ventricular myocardium
Disruption at any level produces a characteristic conduction disorder.
Classification
I. Sinoatrial (SA) Node Disorders
| Disorder | Description |
|---|---|
| Sinus bradycardia | Rate < 60 bpm; can be physiologic (athletes) or pathologic |
| Sick Sinus Syndrome (SSS) | Dysfunction of SA node: bradycardia, sinus arrest, sinoatrial block, tachy-brady syndrome |
| Sinus arrest / SA block | Failure of SA node to fire or conduct to atria |
II. Atrioventricular (AV) Block
| Degree | ECG Finding | Clinical Significance |
|---|---|---|
| 1st Degree | PR interval > 200 ms; all P waves conduct | Usually benign; can be drug-induced |
| 2nd Degree – Mobitz I (Wenckebach) | Progressive PR prolongation until a QRS is dropped | Often at AV node level; usually benign; may be vagally mediated |
| 2nd Degree – Mobitz II | Constant PR interval with sudden dropped QRS | Infranodal (His-Purkinje); unpredictable — high risk of progression to complete block |
| 3rd Degree (Complete) | No relationship between P waves and QRS; AV dissociation | Life-threatening; requires pacemaker |
III. Bundle Branch & Fascicular Blocks
| Block | Key ECG Features | Common Associations |
|---|---|---|
| RBBB | rsR' in V1; wide slurred S in I, V6; QRS ≥ 120 ms | ASD, PE, RV strain; also seen in normal hearts |
| LBBB | Broad monophasic R in I, aVL, V6; no septal Q waves; QRS ≥ 120 ms | Coronary artery disease, hypertensive heart disease, aortic valve disease, dilated cardiomyopathy |
| Left Anterior Fascicular Block (LAFB) | Left axis deviation (−45° to −90°); qR in I, aVL; rS in II, III, aVF | Most common fascicular block; often isolated |
| Left Posterior Fascicular Block (LPFB) | Right axis deviation; rS in I, aVL; qR in III, aVF | Less common; diagnosis of exclusion |
| Bifascicular block | RBBB + LAFB (most common) or RBBB + LPFB | Carries risk of progression to complete block |
| Trifascicular block | Bifascicular block + 1st/2nd degree AV block | High risk; pacemaker often indicated |
Per Harrison's Principles (p. 6801), LBBB specifically is a marker of one of four high-risk underlying conditions: coronary heart disease (often with impaired LV function), hypertensive heart disease, aortic valve disease, and dilated cardiomyopathy.
ECG Example: Multilevel Conduction Disease
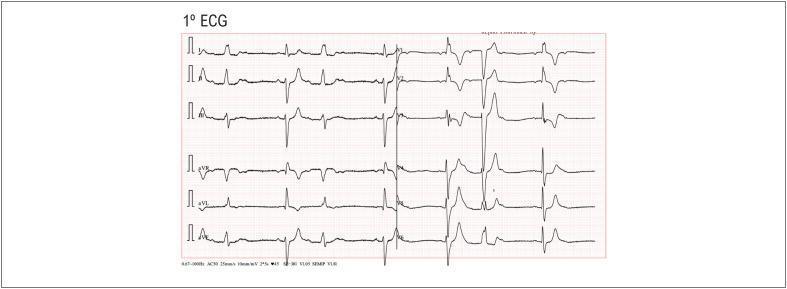
This 12-lead ECG shows alternating RBBB and LBBB on a beat-to-beat basis with concomitant Mobitz I (Wenckebach) AV block — representing extensive multilevel His-Purkinje disease with high risk of progression to complete heart block.
Etiology
- Ischemic heart disease (most common cause of acquired block)
- Degenerative/fibrotic disease (Lev's disease, Lenègre's disease — progressive fibrosis of the conduction system)
- Infectious: Lyme disease, Chagas disease, myocarditis, infective endocarditis with abscess
- Infiltrative: Sarcoidosis, amyloidosis, hemochromatosis
- Metabolic: Hyperkalemia, hypothyroidism
- Autoimmune: SLE (neonatal lupus → congenital complete heart block)
- Iatrogenic: Drug toxicity (digoxin, beta-blockers, calcium channel blockers, antiarrhythmics), post-cardiac surgery, catheter ablation
- Congenital: Congenitally corrected TGA, ASD, Ebstein's anomaly
- Neuromuscular disorders: Myotonic dystrophy, Kearns-Sayre syndrome
Clinical Presentation
| Symptom | Underlying Mechanism |
|---|---|
| Fatigue, exercise intolerance | Reduced cardiac output |
| Presyncope / syncope (Stokes-Adams attacks) | Sudden complete heart block or pause |
| Palpitations | Escape rhythms, compensatory changes |
| Dyspnea | Low output, especially with LBBB + LV dysfunction |
| Asymptomatic | Many BBBs and 1st-degree blocks |
Diagnosis
- 12-lead ECG — cornerstone of diagnosis
- Ambulatory monitoring (Holter, event recorder, implantable loop recorder) — for intermittent/paroxysmal blocks
- Exercise stress testing — to unmask rate-dependent blocks or exercise-induced AV block
- Electrophysiology (EP) study — measures HV interval; HV > 70 ms suggests infranodal disease; HV > 100 ms strongly predicts progression to complete block
- Echocardiography — assess structural heart disease, LV dysfunction (especially with LBBB)
- Cardiac MRI — evaluate myocardial scar, infiltrative disease (sarcoid, amyloid)
- Lab work — electrolytes, thyroid function, Lyme serology, iron studies, ANA/anti-Ro in appropriate context
Management
Acute / Reversible Causes
- Correct underlying cause first: treat hyperkalemia, withhold offending drugs, antibiotics for Lyme disease
- Atropine (0.5–1 mg IV) for symptomatic vagally mediated bradycardia/AV block
- Transcutaneous pacing — for hemodynamically unstable patients
- Transvenous temporary pacing — bridge for high-degree blocks pending definitive therapy
Permanent Pacemaker Indications (ACC/AHA Guidelines)
| Indication | Class |
|---|---|
| Symptomatic complete (3rd-degree) AV block | I (mandatory) |
| Symptomatic Mobitz II 2nd-degree AV block | I |
| Asymptomatic complete AV block with documented pauses > 3 s or escape rate < 40 bpm | I |
| Asymptomatic Mobitz II with wide QRS | IIa |
| Bifascicular or trifascicular block with syncope and suspected advanced AV block | I |
| HV interval ≥ 100 ms on EP study (non-physiologic) | IIa |
| SSS with symptomatic bradycardia | I |
Device Therapy Considerations
- CRT (Cardiac Resynchronization Therapy): Indicated in LBBB with QRS ≥ 150 ms, EF ≤ 35%, NYHA Class II–IV despite optimal medical therapy — restores ventricular synchrony and improves outcomes
- His-bundle pacing / Left bundle branch area pacing (LBBAP): Emerging alternatives to conventional RV pacing that preserve physiologic conduction and avoid pacing-induced cardiomyopathy
Complications
- Progression to complete heart block (especially Mobitz II, trifascicular block)
- Sudden cardiac death
- Pacing-induced cardiomyopathy from chronic RV apical pacing (dyssynchrony → LV dysfunction)
- Syncope and trauma
- Reduced quality of life from fatigue and exercise intolerance
Key Clinical Pearls
- RBBB alone in an otherwise healthy person is generally benign and does not require workup beyond baseline ECG.
- New LBBB warrants urgent evaluation to exclude acute MI (STEMI equivalent if new with chest pain — Sgarbossa criteria apply).
- Alternating bundle branch block (beat-to-beat RBBB/LBBB alternation) signals extensive His-Purkinje disease and is a near-absolute indication for permanent pacemaker.
- Lyme carditis is a reversible cause of high-degree AV block — always check Lyme serology in endemic areas with unexplained AV block, especially in young patients.
- Mobitz I in inferior MI reflects ischemia to the AV node (RCA territory) — usually transient. Mobitz II in anterior MI indicates massive infranodal ischemia — carries poor prognosis and requires pacing.
This is a shared conversation. Sign in to Orris to start your own chat.