Presbycusis in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
presbycusis age-related hearing loss pathophysiology classification types
search_medical_text
presbycusis audiological evaluation diagnosis management rehabilitation hearing aids
search_medical_image
presbycusis cochlea inner ear anatomy age-related changes audiogram
GradeResponse
GradeResponse
GradeResponse
Good results obtained. Now let me compile the comprehensive 50-mark answer synthesizing all the referenced textbooks and recent advances.
PRESBYCUSIS (Age-Related Hearing Loss)
A Comprehensive 50-Mark Answer
As per RGUHS University Syllabus | References: Scott-Brown, Cummings, Stell & Maran, Zakir Hussain, Dhingra, Hazarika, Harrison's, and Recent Literature
1. DEFINITION
Presbycusis (Greek: presbys = old man; akousis = hearing) is a bilateral, symmetrical, progressive sensorineural hearing loss due to age-related degenerative changes of the cochlea and/or central auditory pathways, typically occurring in individuals above 60 years of age, in the absence of other causative factors.
(Dhingra – Diseases of Ear, Nose & Throat; Scott-Brown's Otorhinolaryngology, Head & Neck Surgery)
2. EPIDEMIOLOGY
| Age Group | Approximate Prevalence |
|---|---|
| 60–70 years | ~25–30% |
| 70–80 years | ~40–50% |
| >80 years | >60–70% |
| >75 years (USA) | >50% |
- Most common cause of sensorineural hearing loss (SNHL) in adults (Harrison's, p. 1026)
- More common in males (occupational noise exposure as contributing factor)
- The aging population is expected to double over the next 40 years, making this a major public health concern
3. ANATOMY RELEVANT TO PRESBYCUSIS
Cochlear Anatomy (Sites of Age-Related Degeneration)
COCHLEA — Key Structures Affected
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
┌─────────────────────────────────┐
│ SCALA VESTIBULI (perilymph) │
├─────────────────────────────────┤
│ SCALA MEDIA (endolymph) │ ← Stria vascularis (metabolic)
│ ┌─────────────────────────┐ │
│ │ Organ of Corti │ │ ← Hair cells (sensory)
│ │ - Inner Hair Cells │ │
│ │ - Outer Hair Cells │ │
│ └─────────────────────────┘ │
│ Basilar Membrane │ ← Mechanical changes
│ Reissner's Membrane │
├─────────────────────────────────┤
│ SCALA TYMPANI (perilymph) │
└─────────────────────────────────┘
Spiral Ganglion Neurons ────────── Neural (neural presbycusis)
Stria Vascularis ────────────────── Metabolic (strial presbycusis)
- Basal turn of cochlea (high-frequency region) is most vulnerable
- Tonotopic organization: High frequencies (8–16 kHz) at base; Low frequencies (250–500 Hz) at apex
4. ETIOPATHOGENESIS
Causative Factors
┌───────────────────────────────────────────┐
│ PRESBYCUSIS — ETIOLOGY │
├─────────────────┬─────────────────────────┤
│ INTRINSIC │ EXTRINSIC │
│ (Aging itself) │ (Accelerating factors) │
├─────────────────┼─────────────────────────┤
│ • Genetic │ • Noise exposure (NIHL) │
│ predisposition│ • Ototoxic drugs │
│ • Mitochondrial │ • Cardiovascular disease│
│ DNA mutations │ • Diabetes mellitus │
│ • Apoptosis of │ • Smoking │
│ hair cells │ • Poor diet/nutrition │
│ • Oxidative │ • Chronic infections │
│ stress │ • Head trauma │
└─────────────────┴─────────────────────────┘
Molecular Mechanisms (Recent Advances)
- Mitochondrial DNA (mtDNA) deletions — "common deletion" (4977 bp) accumulates in cochlear cells with age
- Reactive Oxygen Species (ROS) — Oxidative stress leads to hair cell apoptosis
- Glutamate excitotoxicity — Excess neurotransmitter damages spiral ganglion neurons
- Telomere shortening — Reduced regenerative capacity of supporting cells
- Decreased BDNF (Brain-Derived Neurotrophic Factor) — Reduced survival signaling for spiral ganglion neurons
- Inflammaging — Chronic low-grade inflammation in elderly cochlea
5. CLASSIFICATION (Schuknecht's Classification — MOST IMPORTANT)
H.F. Schuknecht (1955, revised 1993) classified presbycusis into 4 pure types and 2 mixed types based on histopathological findings:
┌──────────────────────────────────────────────────────────────────────┐
│ SCHUKNECHT'S CLASSIFICATION OF PRESBYCUSIS │
├─────────────────┬────────────────────────────────────────────────── ┤
│ TYPE │ SITE OF LESION │ AUDIOGRAM PATTERN │
├─────────────────┼──────────────────────┼────────────────────────────┤
│ 1. SENSORY │ Organ of Corti │ Sharply sloping high-freq │
│ │ (OHC > IHC) │ loss; good discrimination │
│ │ Basal turn atrophy │ │
├─────────────────┼──────────────────────┼────────────────────────────┤
│ 2. NEURAL │ Spiral ganglion │ Flat or gradually sloping; │
│ │ neurons (↓ 50%) │ POOR discrimination >loss │
│ │ │ Disproportionate │
├─────────────────┼──────────────────────┼────────────────────────────┤
│ 3. STRIAL / │ Stria vascularis │ Flat audiogram; │
│ METABOLIC │ (atrophy >30%) │ Excellent discrimination; │
│ │ Endolymph ion pump ↓ │ Best prognosis with HA │
├─────────────────┼──────────────────────┼────────────────────────────┤
│ 4. MECHANICAL / │ Basilar membrane │ Linearly descending slope; │
│ COCHLEAR │ (stiffening/thicken- │ Calculated not measured │
│ CONDUCTIVE │ ing — base to apex) │ │
├─────────────────┼──────────────────────┼────────────────────────────┤
│ 5. MIXED │ Combination of above │ Variable │
├─────────────────┼──────────────────────┼────────────────────────────┤
│ 6. INDETERMINATE│ No identifiable │ Variable │
│ │ histopathology │ │
└─────────────────┴──────────────────────┴────────────────────────────┘
Key Point for Exams (RGUHS): Strial presbycusis has the best prognosis with hearing aids; Neural presbycusis has the worst speech discrimination.
Additional Classification by Gates & Mills (2005) — "Gates Classification"
- Peripheral presbycusis (cochlear)
- Central presbycusis (brainstem/cortical — decreased temporal processing)
- Combined presbycusis
6. PATHOLOGY — HISTOPATHOLOGICAL CHANGES
A. Sensory Presbycusis
- Loss of outer hair cells (OHC) > inner hair cells
- Atrophy starts at basal turn → progresses apically
- Degeneration of stereocilia (loss of tip links, fusion)
- Supporting cells (Deiters', pillar cells) collapse
B. Neural Presbycusis
- Loss of spiral ganglion neurons (Type I > Type II)
- Reduced myelination of cochlear nerve fibers
- Up to 50% neuronal loss before audiometric changes appear
C. Strial (Metabolic) Presbycusis
- Atrophy of stria vascularis (responsible for K⁺-rich endolymph)
- Reduction in endocochlear potential (normally +80 mV)
- Impairs the "cochlear battery" — reduces driving force for mechanotransduction
- Most common type in humans (30–35% of presbycusis cases)
D. Mechanical Presbycusis
- Stiffening and thickening of basilar membrane
- Changes in viscoelastic properties
- Base more affected than apex
7. CLINICAL FEATURES
Symptoms (RGUHS Emphasis)
TRIAD OF PRESBYCUSIS:
1. Bilateral, symmetrical, progressive SNHL
2. Difficulty understanding SPEECH (especially in noise)
3. Tinnitus (high-pitched; in ~30%)
Characteristic Features:
- Insidious onset — patient and family may not notice initially
- High-frequency hearing loss first — difficulty hearing doorbells, telephone rings, consonants (s, f, th, sh)
- Recruitment — abnormal loudness growth (sounds seem too loud suddenly)
- Diplacusis — pitch distortion
- Phonemic regression — speech discrimination loss disproportionate to pure-tone average
- Cocktail party effect — difficulty hearing speech in background noise
- Paracusis willisii is ABSENT (differentiates from otosclerosis)
Associated Comorbidities (Recent Evidence):
- Cognitive decline / dementia (strong association) (Harrison's, p. 1026)
- Increased risk of falls and accidents
- Social isolation, depression, anxiety
- Reduced quality of life
8. AUDIOLOGICAL EVALUATION
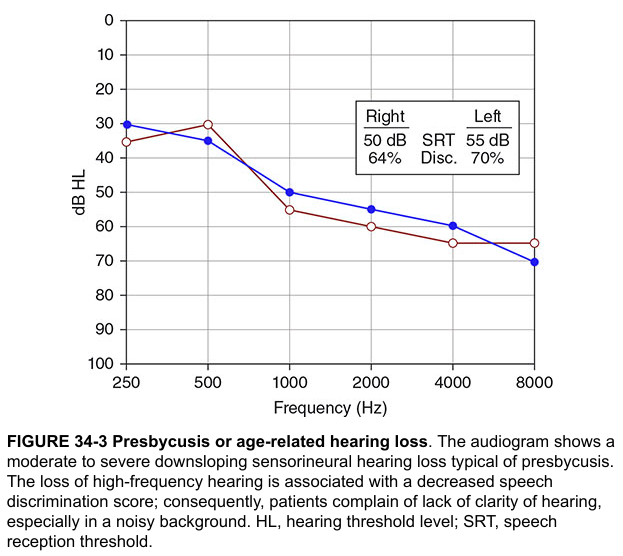
A. Pure Tone Audiogram (PTA) — GOLD STANDARD
The classic audiogram of presbycusis shows a bilateral symmetric downsloping SNHL predominantly affecting high frequencies:
Audiogram Patterns by Schuknecht Type:
dB HL
0 ├────────────────────── Strial (flat)
20 │ ╲
40 │ ╲──────────── Sensory (high-freq drop)
60 │ ╲
80 │ Neural (flat, poor discrimination)
250 500 1K 2K 4K 8K Hz
B. Speech Audiometry
| Parameter | Finding |
|---|---|
| Speech Reception Threshold (SRT) | Elevated (matches PTA) |
| Speech Discrimination Score (SDS) | Reduced (especially neural type) |
| Most Comfortable Level (MCL) | Reduced range due to recruitment |
| Uncomfortable Loudness Level (UCL) | Low (recruitment) |
C. Impedance Audiometry (Tympanometry)
- Type A tympanogram (normal middle ear compliance)
- Acoustic reflexes — absent at high frequencies (may be elevated threshold)
- Rules out middle ear pathology
D. Otoacoustic Emissions (OAE)
- Distortion Product OAE (DPOAE): Reduced or absent at high frequencies
- Reflects OHC dysfunction
- Useful for early detection before PTA changes
E. Auditory Brainstem Response (ABR)
- Prolonged I-V interpeak latency — indicates neural transmission delay
- Wave I amplitude reduction — reflects peripheral neural loss
- Useful to rule out retrocochlear pathology
F. High-Frequency Audiometry (Extended High-Frequency Testing)
- Tests 8,000–20,000 Hz
- Most sensitive early indicator of presbycusis
- Detects subclinical cochlear aging
9. DIAGNOSTIC CRITERIA AND DIFFERENTIAL DIAGNOSIS
Diagnostic Criteria for Presbycusis:
- Age > 50–60 years
- Bilateral, symmetrical SNHL
- Gradual, progressive onset
- High-frequency loss predominant
- No other identifiable cause (noise, ototoxins, Ménière's disease, acoustic neuroma)
- Normal tympanogram (Type A)
Differential Diagnosis:
| Condition | Key Differentiating Feature |
|---|---|
| Noise-induced hearing loss (NIHL) | Notch at 4 kHz; history of noise exposure |
| Ototoxic hearing loss | Drug history; may be reversible |
| Ménière's disease | Fluctuating, unilateral; vertigo; aural fullness |
| Acoustic neuroma | Unilateral; poor speech discrimination; ABR abnormal |
| Otosclerosis | Conductive/mixed; Paracusis Willisii present; Carhart's notch |
| Autoimmune SNHL | Rapid progression; younger; responds to steroids |
| Hypothyroidism | Systemic features; reversible with treatment |
10. FLOWCHART: DIAGNOSTIC APPROACH TO PRESBYCUSIS
ELDERLY PATIENT WITH HEARING DIFFICULTY
│
▼
HISTORY & PHYSICAL EXAMINATION
• Age, onset, progression, laterality
• Drug history (aminoglycosides, cisplatin)
• Noise exposure history
• Family history
• Otoscopy (rule out wax, perforated TM)
│
▼
AUDIOLOGICAL WORKUP
│
┌──────────┴──────────┐
▼ ▼
PTA (250–8000 Hz) TYMPANOMETRY
│
┌──────────┴──────────┐
▼ ▼
Bilateral SNHL Conductive/Mixed?
(High-freq, symmetric) → Rule out middle ear disease
│
▼
SPEECH AUDIOMETRY
(SRT, SDS, SISI, Tone Decay)
│
▼
DPOAE / ABR
(Confirm cochlear vs neural)
│
┌──────────┴──────────┐
▼ ▼
Normal ABR Abnormal ABR
(Peripheral/cochlear) → MRI CP angle
(Rule out schwannoma)
│
▼
DIAGNOSIS: PRESBYCUSIS
(Classify Schuknecht type)
│
▼
MANAGEMENT PLAN
11. MANAGEMENT
A. Medical Management
No pharmacological agent is currently proven to reverse or halt presbycusis.
However, the following are under investigation (Recent Advances):
| Drug/Agent | Mechanism | Evidence Level |
|---|---|---|
| Antioxidants (Vit C, E, NAC) | Reduce ROS-mediated hair cell death | Animal models; limited human trials |
| Coenzyme Q10 | Mitochondrial protection | Experimental |
| Magnesium | Reduces cochlear ischemia | Some clinical data |
| Aldosterone | Stria vascularis function | Clinical trial ongoing |
| Nicotinamide riboside | NAD+ precursor; mitochondrial repair | Recent phase I/II trials |
B. Hearing Aids — MAINSTAY OF MANAGEMENT
Indications for Hearing Aids:
- PTA > 25–30 dB HL in better ear
- Difficulty with speech understanding in daily life
Types:
HEARING AID SELECTION FOR PRESBYCUSIS
│
┌──────────┴──────────┐
▼ ▼
ANALOG DIGITAL
(Less preferred) (PREFERRED — better speech in noise)
│
┌──────────┼──────────┐
▼ ▼ ▼
BTE ITE ITC/CIC
(Behind (In-the- (Canal/Completely
the ear) ear) in canal)
BTE (Behind-the-Ear):
- Best for severe-profound loss
- Easiest to handle (elderly patients with poor manual dexterity)
Digital Hearing Aids Features:
- Directional microphones — improve signal-to-noise ratio
- Digital noise reduction
- Feedback cancellation
- Frequency compression — beneficial in steeply sloping high-frequency loss
- Bluetooth connectivity (recent)
C. Cochlear Implants
Indications:
- Profound bilateral SNHL (>90 dB in better ear)
- Hearing aid benefit < 50% sentence recognition
- No medical contraindications
Results in Elderly:
- Good outcomes even in 70–90 age group
- Improves quality of life, reduces social isolation
- Neural presbycusis responds less favorably than strial type
Recent Advance: Hybrid cochlear implants (electroacoustic stimulation) — preserve residual low-frequency hearing while electrically stimulating high frequencies
D. Auditory Brainstem Implant (ABI)
- For patients with cochlear nerve aplasia
- Less commonly used in presbycusis
E. Aural Rehabilitation
A comprehensive program including:
AURAL REHABILITATION PROGRAM
│
┌──────┼──────┬──────────┐
▼ ▼ ▼ ▼
HA Speech Lip Environmental
Fitting Reading Training Modifications
│
┌──────┼──────┐
▼ ▼ ▼
LACE Group Assistive
Program Therapy Listening
(Listen- Devices (ALD)
ing in
noise)
Assistive Listening Devices (ALDs):
- FM systems (loop systems in theaters/churches)
- Captioned telephones
- Visual alerting systems (flashing doorbell)
- Vibrotactile devices
F. Patient and Family Counseling
- Speak clearly, face the patient, reduce background noise
- Avoid shouting (triggers recruitment)
- Use short sentences, check comprehension
- Adequate lighting for lip reading
12. CENTRAL PRESBYCUSIS
(Emphasized in Scott-Brown and Cummings)
- Age-related changes in central auditory processing beyond the cochlea
- Sites: cochlear nucleus, inferior colliculus, auditory cortex
- Characterized by:
- Difficulty understanding rapid speech
- Poor performance in competing message tests
- Abnormal Auditory Processing Disorder (APD) tests
- Diagnosis: Dichotic listening tests, temporal processing tests (Gap Detection Threshold)
- Managed with: central auditory training programs, LACE therapy
13. FLOWCHART: MANAGEMENT OF PRESBYCUSIS
CONFIRMED PRESBYCUSIS
│
▼
SEVERITY ASSESSMENT
(PTA Average in Better Ear)
│
┌────┴────────────────┐
▼ ▼
25–70 dB HL >70–90 dB HL
(Mild–Moderate– (Severe–Profound)
Moderately Severe)
│ │
▼ ▼
HEARING AIDS POWERFUL HA trial
(BTE/ITE/Digital) + Cochlear Implant
│ Evaluation
▼
AURAL REHABILITATION
(Speech therapy, lip reading,
ALD, counseling)
│
▼
MEDICAL CO-MORBIDITY MANAGEMENT
(Cardiovascular, diabetes control)
│
▼
FOLLOW-UP EVERY 6–12 MONTHS
(Repeat PTA, HA fine-tuning)
14. RECENT ADVANCES IN PRESBYCUSIS (Critical for RGUHS 50-mark answer)
A. Genetic Research
- KCNQ4 gene mutations (DFNA2 locus) → OHC degeneration
- GJB2/GJB6 (Connexin 26/30) variants modify age-related loss
- Mitochondrial haplogroups influence presbycusis susceptibility
- GWAS studies (Genome-Wide Association Studies) — identified >50 loci
B. Biomarkers
- Serum BDNF levels — correlate with spiral ganglion neuron density
- Inflammatory cytokines (IL-6, TNF-α) as predictors of cochlear aging
- Cochlin — inner ear specific protein as biomarker
C. Regenerative Therapies (Experimental)
| Approach | Status |
|---|---|
| Gene therapy (AAV-BDNF, Atoh1/Math1) | Animal models — regenerates hair cells |
| Stem cell therapy | Phase I human trials initiated |
| Lgr5+ progenitor cell activation | Cochlear supporting cell → hair cell transdifferentiation |
| Notch inhibition | Promotes hair cell regeneration from supporting cells |
| CRISPR-Cas9 gene editing | Silencing of otoprotective gene variants |
D. Drug Delivery
- Intratympanic drug delivery (round window membrane absorption)
- Nanoparticle-based cochlear drug delivery
- Hydrogel sustained-release into the round window niche
E. AI and Digital Health
- AI-powered hearing aids — automatic environment classification
- OTC (Over-The-Counter) hearing aids — FDA approved 2022 (USA)
- Smartphone-based audiometry (validated for screening)
- Deep neural network processing in cochlear implants
- Teleaudiology — remote hearing aid fitting and follow-up
F. Cochlear Implant Advances
- Totally implantable cochlear implants (TICI)
- Optical cochlear implants (using near-infrared laser stimulation of neurons)
- Auditory nerve regeneration at implant-cochlea interface
- Fine structure processing (FSP) strategies — improve music perception
G. Preventive Strategies (Evidence-Based)
- Cardiovascular risk factor modification (HTN, diabetes, dyslipidemia)
- Avoidance of ototoxic drugs in elderly
- Noise protection throughout life
- Mediterranean diet — associated with slower presbycusis progression
- Exercise — increases cochlear blood flow
15. PREVENTION OF PRESBYCUSIS
PRIMARY PREVENTION SECONDARY PREVENTION TERTIARY PREVENTION
│ │ │
Reduce risk factors Early detection Rehabilitation
• Noise protection • Screening ≥60 yrs • Hearing aids
• Avoid ototoxins • OAE/PTA • Cochlear implants
• Cardiovascular control • Geriatric audiometry • Aural rehab
• Antioxidant-rich diet • HHIE Questionnaire • Counseling
• Exercise (Hearing Handicap • Support groups
• Smoking cessation Inventory for Elderly)
Screening Tools:
- HHIE (Hearing Handicap Inventory for Elderly) — validated questionnaire
- Whisper test
- Finger rub test
- Smartphone-based apps (recent advance)
16. PRESBYCUSIS AND COGNITION — A CRITICAL RECENT CONCEPT
(Hazarika; Recent Literature)
- Frank Lin et al. (2011, JAMA) — Each 10 dB increase in hearing loss → 2× increased dementia risk
- Lancet Commission (2020) — Hearing loss is the single largest modifiable risk factor for dementia (attributable risk = 8%)
- Possible mechanisms:
- Cognitive load theory (brain diverts resources to hearing → less for cognition)
- Social isolation → reduced cognitive stimulation
- Common underlying neurodegenerative process
- Early hearing aid fitting may slow cognitive decline
17. SUMMARY TABLE
| Feature | Details |
|---|---|
| Definition | Bilateral symmetric progressive SNHL due to aging |
| Peak incidence | > 60 years |
| Genetics | Multifactorial; mtDNA deletions; KCNQ4 |
| Histopathology | Schuknecht 4 types: Sensory, Neural, Strial, Mechanical |
| Audiogram | Bilateral, symmetric, downsloping SNHL |
| Best prognosis | Strial type (best discrimination) |
| Worst prognosis | Neural type (worst discrimination) |
| Gold standard Rx | Digital hearing aids (BTE preferred in elderly) |
| Cochlear implant | Profound bilateral SNHL; HA benefit < 50% |
| Recent advance | Gene therapy, stem cells, AI hearing aids, OTC HA |
| Cognition link | Largest modifiable dementia risk factor |
18. RGUHS VIVA / EXAM TIPS
- Schuknecht's classification with audiogram patterns — must know all 4 types
- Neural presbycusis = worst speech discrimination (disproportionate)
- Strial presbycusis = best HA outcome (flat audiogram + good discrimination)
- 4 kHz notch → NIHL, NOT presbycusis
- Recruitment is present in presbycusis (cochlear, not retrocochlear)
- Paracusis Willisii is ABSENT (differentiates from otosclerosis)
- Phonemic regression = speech discrimination worse than PTA predicts
- HHIE = gold standard screening questionnaire for presbycusis
- Cochlear implantation is effective and recommended even in elderly >70 years
- Presbycusis is the most common cause of SNHL in adults
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery (8th Ed.) — Vol. 3, Chapter on Sensorineural Hearing Loss
- Cummings Otolaryngology – Head & Neck Surgery (7th Ed.) — Chapter 152: Presbycusis
- Stell & Maran's Textbook of Head & Neck Surgery and Oncology — Sensorineural Hearing Loss chapter
- Zakir Hussain – Textbook of ENT and Head & Neck Surgery — Presbycusis
- Dhingra – Diseases of Ear, Nose and Throat (7th Ed.) — Chapter: Sensorineural Hearing Loss
- Hazarika – Textbook of ENT & Head-Neck Surgery — Chapter on Deafness
- Harrison's Principles of Internal Medicine (21st Ed.) — p. 1026–1027
- Schuknecht HF — Presbycusis. Laryngoscope 1955; 65(6):402–419
- Gates GA, Mills JH — Presbycusis. Lancet 2005; 366:1111–1120
- Lin FR et al. — Hearing loss and dementia incidence. JAMA 2011; 305(2):166–173
- Lancet Commission on Dementia Prevention (2020) — hearing loss as modifiable risk factor
- FDA OTC Hearing Aid Rule — 2022
- Liberman MC — Noise-induced and age-related hearing loss: new perspectives and potential therapies. F1000Research 2017
This answer is structured for a 50-mark RGUHS University long essay question. It covers definition, epidemiology, anatomy, etiopathogenesis, Schuknecht's classification (the most important classification), histopathology, clinical features, comprehensive audiological workup, diagnostic flowcharts, management algorithm, aural rehabilitation, and recent advances in genetics, regenerative medicine, AI hearing aids, and the critical presbycusis-dementia link.
This is a shared conversation. Sign in to Orris to start your own chat.