Clinical significance of vagus nerve and phrenic nerve
Reading File
search_medical_text
vagus nerve clinical significance anatomy functions
search_medical_text
phrenic nerve clinical significance anatomy diaphragm
search_medical_image
vagus nerve phrenic nerve anatomy diagram
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive overview of the clinical significance of both nerves:
Vagus Nerve (CN X)
Anatomy & Course
- Arises from the medulla oblongata (dorsal motor nucleus, nucleus ambiguus, nucleus tractus solitarius)
- Exits the skull via the jugular foramen, then descends in the carotid sheath alongside the carotid artery and internal jugular vein
- Branches into pharyngeal, superior laryngeal, recurrent laryngeal, cardiac, pulmonary, and esophageal branches
- Continues into the abdomen via the esophageal hiatus, supplying foregut and midgut viscera
Functions
| Component | Function |
|---|---|
| GSA (General Somatic Afferent) | Sensation from the external ear (Arnold's nerve), dura of posterior fossa |
| GVA (General Visceral Afferent) | Sensation from pharynx, larynx, trachea, esophagus, heart, lungs, abdominal viscera |
| GVE (General Visceral Efferent) | Parasympathetic to thoracic and abdominal viscera (heart, lungs, gut to splenic flexure) |
| SVA (Special Visceral Afferent) | Taste from epiglottis/posterior pharynx |
| SVE (Special Visceral Efferent) | Motor to pharynx (swallowing), soft palate, larynx (voice) |
Clinical Significance
1. Lesions and their manifestations
- Unilateral vagal palsy: Hoarseness (ipsilateral vocal cord paralysis), dysphagia, loss of gag reflex on the affected side, uvular deviation away from the lesion
- Bilateral vagal palsy: Life-threatening — complete aphonia, severe dysphagia, risk of aspiration
2. Causes of vagal damage
- Intracranial: Tumors, lateral medullary syndrome (PICA infarct — Wallenberg syndrome), motor neuron disease, varicella-zoster infection (Harrison's, p. 12510)
- Neck: Carotid dissection, carotid endarterectomy, neck surgery, lymphadenopathy
- Chest: Aortic aneurysm, enlarged mediastinal lymph nodes, lung tumors (especially left recurrent laryngeal nerve)
- Diphtheria: Pharyngeal branches affected → nasal voice, nasal regurgitation of liquids
3. Recurrent Laryngeal Nerve (RLN) — key branch
- Left RLN loops under the aortic arch; right RLN loops under the subclavian artery
- Left RLN palsy: suspect thoracic pathology (aortic aneurysm, mediastinal mass, apical lung tumor — Pancoast)
- RLN injury during thyroidectomy or parathyroidectomy is a major surgical complication
4. Vasovagal syncope
- Excessive vagal tone → bradycardia + vasodilation → transient loss of consciousness
- Triggered by pain, emotional stress, prolonged standing, Valsalva
5. Vagal maneuvers in arrhythmias
- Carotid sinus massage, Valsalva, diving reflex — used to terminate SVT (AVNRT) by increasing vagal tone
6. Vagus Nerve Stimulation (VNS)
- FDA-approved for refractory epilepsy and treatment-resistant depression
- Investigational in rheumatoid arthritis, IBD (anti-inflammatory vagal arc), heart failure
7. Gut-brain axis
- ~80% of vagal fibers are afferent, transmitting gut microbiome signals, satiety, inflammation to the CNS
- Vagal afferents mediate the inflammatory reflex (cholinergic anti-inflammatory pathway)
Phrenic Nerve (C3, C4, C5)
Anatomy & Course
- Arises from anterior rami of C3, C4, C5 ("C3, 4, 5 keeps the diaphragm alive")
- Formed in the neck on the anterior surface of scalenus anterior
- Enters the thorax by crossing the subclavian artery, then descends between the lung and pericardium
- Right phrenic nerve: Crosses the right subclavian artery, runs along the right atrium, passes through the caval opening (T8) of the diaphragm
- Left phrenic nerve: Crosses the aortic arch, runs along the left ventricle, pierces the left dome of the diaphragm separately
Functions
| Component | Function |
|---|---|
| Motor | Sole motor supply to the ipsilateral hemidiaphragm |
| Sensory | Central part of the diaphragm, mediastinal pleura, pericardium, peritoneum (subphrenic) |
Clinical Significance
1. Phrenic nerve palsy
- Causes elevated hemidiaphragm on CXR, dyspnea, tachypnea, hiccups, thoracic/shoulder tip pain
- Confirmed by fluoroscopy (sniff test) or diaphragm ultrasound — paradoxical upward movement of the affected hemidiaphragm on sniffing (Catheter and Surgical Ablation of AF, p. 73)
- Bilateral palsy → respiratory failure requiring ventilatory support
2. Causes of phrenic nerve injury
| Category | Examples |
|---|---|
| Surgical | Cardiac surgery (ice slush hypothermia), CABG, thyroid/parathyroid surgery, thoracic surgery |
| Procedural | Catheter ablation for AF (proximity of right phrenic to SVC/right superior pulmonary vein), subclavian/internal jugular central line placement |
| Neoplastic | Lung cancer (especially Pancoast), mediastinal tumors, lymphoma |
| Infectious | Herpes zoster, Lyme disease, viral neuritis |
| Neurological | Neuralgic amyotrophy (Parsonage-Turner syndrome), motor neuron disease |
| Trauma | Cervical spine injury (C3–C5), birth trauma (neonatal brachial plexus injury) |
3. Referred pain (C3–C5 dermatome)
- Subdiaphragmatic irritation (ruptured ectopic pregnancy, subphrenic abscess, hemoperitoneum, splenic rupture) → referred pain to the ipsilateral shoulder tip (Kehr's sign)
- Pericarditis and pleuritis can similarly refer to the shoulder via phrenic sensory fibers
4. Hiccups (singultus)
- Phrenic nerve irritation (or central causes) produces involuntary diaphragmatic spasm
- Persistent hiccups (>48 h): investigate for phrenic nerve irritation, medullary lesions, metabolic causes (uremia, GERD)
- Treatment: chlorpromazine, baclofen, gabapentin; phrenic nerve block in refractory cases
5. Phrenic nerve pacing (diaphragm pacing)
- Used in high cervical spinal cord injuries (C1–C2) where phrenic nucleus is intact but input is lost
- Electrodes placed on the phrenic nerve surgically or laparoscopically
Key Comparative Summary
| Feature | Vagus Nerve (CN X) | Phrenic Nerve (C3–C5) |
|---|---|---|
| Origin | Brainstem (medulla) | Cervical plexus |
| Primary motor target | Pharynx, larynx, viscera | Diaphragm |
| Primary autonomic role | Parasympathetic (thorax/abdomen) | None (somatic) |
| Key clinical test | Gag reflex, uvula deviation | Sniff test (fluoroscopy/US) |
| Referred pain | — | Shoulder tip (C3–C5) |
| Surgical risk | Thyroidectomy (RLN), carotid surgery | Cardiac surgery, AF ablation |
| Stimulation therapy | VNS (epilepsy, depression) | Diaphragm pacing (SCI) |
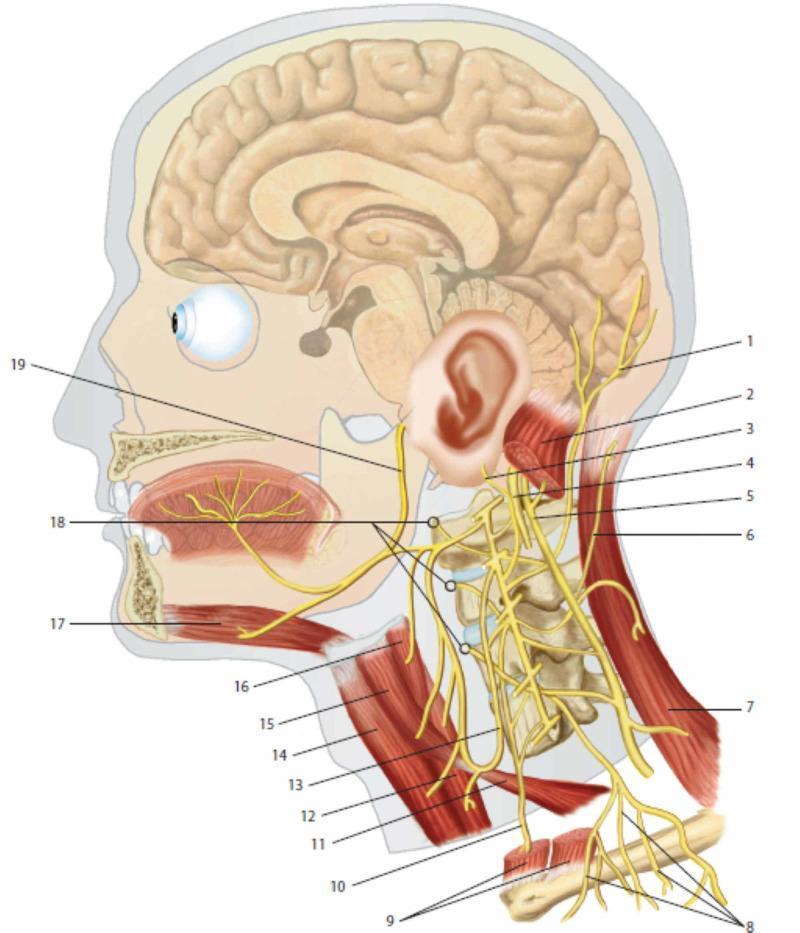
Anatomical Diagram
Key clinical mnemonics:
- "C3, 4, 5 keeps the diaphragm alive" — phrenic nerve origin
- Uvula deviates AWAY from the lesion in unilateral vagal palsy (palate pulled by intact side)
- Left RLN palsy without neck pathology → chest imaging mandatory (aortic arch, mediastinum)
- Kehr's sign = left shoulder pain from subphrenic/splenic blood/fluid irritating the phrenic nerve
This is a shared conversation. Sign in to Orris to start your own chat.