Intravascular hemolysis
Reading File
search_medical_text
intravascular hemolysis pathophysiology mechanisms causes
search_medical_text
intravascular hemolysis laboratory findings diagnosis management
search_medical_image
intravascular hemolysis red blood cell destruction peripheral smear
GradeResponse
GradeResponse
GradeResponse
Intravascular Hemolysis
Definition
Intravascular hemolysis refers to the destruction of red blood cells within the bloodstream (inside blood vessels), releasing hemoglobin directly into the plasma. This is distinct from extravascular hemolysis, which occurs in the reticuloendothelial system (spleen, liver, bone marrow).
Pathophysiology
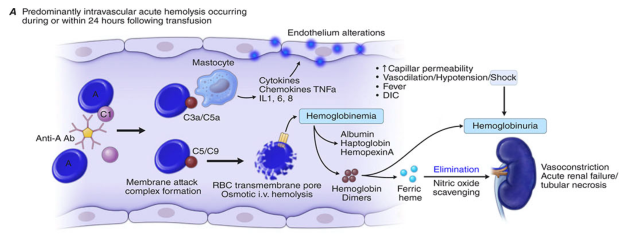
RBC lysis within vessels releases free hemoglobin into the plasma. The sequence of events:
- Free hemoglobin in plasma → dimers form and are initially scavenged by haptoglobin
- When haptoglobin is saturated → free hemoglobin dimers are filtered by the glomerulus → hemoglobinuria
- Tubular reabsorption of hemoglobin leads to iron deposition in tubular cells → hemosiderinuria (appears days later)
- Heme that escapes haptoglobin is bound by hemopexin, then metabolized by the liver
- Free heme/hemoglobin scavenges nitric oxide (NO) → vasoconstriction, smooth muscle dystonias, platelet aggregation
- Systemic inflammation via complement fragments (C3a, C5a), cytokines (TNF-α, IL-1, IL-6, IL-8), and endothelial activation
Causes
| Category | Examples |
|---|---|
| Immune-mediated | ABO-incompatible transfusion, warm/cold autoimmune hemolytic anemia (IgM-mediated), drug-induced |
| Complement-mediated | Paroxysmal nocturnal hemoglobinuria (PNH), cold agglutinin disease |
| Microangiopathic (MAHA) | TTP, HUS, DIC, malignant hypertension, eclampsia |
| Mechanical | Prosthetic heart valves, extracorporeal circulation (ECMO, bypass), march hemoglobinuria |
| Infectious | Malaria (P. falciparum — "blackwater fever"), Clostridium septicemia, Babesiosis |
| Osmotic/toxic | Freshwater drowning, snake/spider venom, certain drugs (dapsone, arsine gas) |
| Metabolic | G6PD deficiency (oxidative stress trigger) |
PNH — Classic Complement-Mediated Intravascular Hemolysis
In PNH, a somatic mutation in PIG-A causes deficiency of GPI-anchored proteins, most critically CD59 (which normally inhibits the membrane attack complex, C5b-9). Without CD59, the MAC inserts freely into RBC membranes → chronic intravascular hemolysis exacerbated by infections, surgery, or thrombosis (Harrison's, p. 3024).
Clinical Features
- Acute presentation: fever, chills, back/flank pain, dark (port-wine/cola-colored) urine
- Chronic presentation: fatigue, anemia, jaundice, splenomegaly (less prominent than extravascular)
- Complications: acute kidney injury (hemoglobin cast nephropathy), thrombosis (NO depletion → platelet activation), pulmonary hypertension (PNH), DIC
Laboratory Findings
The hallmark findings distinguish intravascular from extravascular hemolysis (Harrison's, p. 2981):
| Test | Intravascular Hemolysis | Extravascular Hemolysis |
|---|---|---|
| Plasma hemoglobin | ↑↑ (hemoglobinemia) | Normal/trace |
| Haptoglobin | ↓↓ (consumed) | ↓ (mildly) |
| LDH | ↑↑↑ | ↑ |
| Unconjugated bilirubin | Normal or mildly ↑ | ↑↑ |
| Urinalysis | Hemoglobinuria (red-brown) | Normal or urobilinogen ↑ |
| Hemosiderinuria | ✔ (days later) | ✗ |
| Direct Coombs (DAT) | Positive (if immune) | Positive (if immune) |
| Reticulocytes | ↑ | ↑ |
| Peripheral smear | Schistocytes (MAHA), spherocytes, parasites | Spherocytes, target cells |
Key distinguishing feature: Hemoglobinuria (dark urine positive for heme on dipstick but absent RBCs on microscopy) is the telltale sign of significant intravascular hemolysis.
Diagnosis Approach
- CBC + reticulocyte count — confirm hemolytic anemia
- Peripheral blood smear — identify morphology (schistocytes → MAHA; spherocytes → immune; parasites → malaria/babesiosis)
- LDH, haptoglobin, unconjugated bilirubin — confirm hemolysis and its severity
- Urinalysis — hemoglobinuria, hemosiderinuria
- Direct Antiglobulin Test (DAT/Coombs) — distinguish immune vs. non-immune
- Flow cytometry (CD55/CD59) — if PNH suspected
- ADAMTS13 activity — if TTP suspected
- Blood cultures, thick/thin smears — if infectious etiology
Management
Management is directed at the underlying cause:
| Cause | Key Treatment |
|---|---|
| ABO transfusion reaction | Stop transfusion immediately; IV fluids, maintain urine output; treat AKI |
| PNH | Eculizumab (anti-C5 monoclonal Ab); ravulizumab; consider SCT |
| TTP | Plasma exchange (PLEX) ± caplacizumab, steroids |
| Autoimmune HA (warm) | Corticosteroids, rituximab, IVIG, splenectomy |
| Cold agglutinin disease | Rituximab, avoid cold exposure |
| G6PD deficiency | Remove oxidant trigger; transfuse if severe |
| Malaria | Antimalarials (artemisinin-based) ± exchange transfusion if severe |
| Mechanical valve hemolysis | Valve repair/replacement if severe |
Supportive care: IV fluid resuscitation (maintain urine output ≥1 mL/kg/hr to prevent renal tubular obstruction), folic acid supplementation, transfusion if hemodynamically compromised.
Intravascular vs. Extravascular — Summary
| Feature | Intravascular | Extravascular |
|---|---|---|
| Site | Blood vessels | Spleen, liver, marrow |
| Hemoglobinuria | Yes | No |
| Haptoglobin depletion | Rapid, severe | Slower |
| Splenomegaly | Less prominent | More prominent |
| Examples | PNH, TTP, ABO mismatch | Hereditary spherocytosis, sickle cell, warm AIHA |
This is a shared conversation. Sign in to Orris to start your own chat.