Skull base osteomyelitis in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
skull base osteomyelitis malignant otitis externa etiology pathogenesis clinical features
search_medical_text
skull base osteomyelitis diagnosis investigations CT MRI bone scan treatment management
search_medical_image
skull base osteomyelitis malignant otitis externa CT scan MRI diagram
GradeResponse
GradeResponse
GradeResponse
Good results obtained. Now let me compile the comprehensive 50-mark RGUHS answer drawing from all major ENT textbooks, retrieved sources, and my knowledge base.
SKULL BASE OSTEOMYELITIS (MALIGNANT/NECROTIZING OTITIS EXTERNA)
A Comprehensive 50-Mark Answer — RGUHS Pattern
DEFINITION
Skull base osteomyelitis (SBO), historically termed Malignant Otitis Externa (MOE) or Necrotizing Otitis Externa, is a potentially life-threatening, aggressive osteomyelitis of the skull base that begins in the external auditory canal (EAC) and spreads progressively to involve the cartilaginous-bony junction, periosteum, and skull base bones, with propensity for cranial nerve involvement and intracranial extension.
The term "malignant" was coined by Chandler (1968) — not implying neoplasm but reflecting the malignant course. Meltzer & Kelemen later popularized the term "Skull Base Osteomyelitis" as more anatomically precise. (Cummings Otolaryngology, 7th ed.)
EPIDEMIOLOGY
| Parameter | Details |
|---|---|
| Age | Predominantly >65 years |
| Sex | Males > Females (3:1) |
| Predisposing condition | Diabetes mellitus (90–95% of cases) |
| Causative organism | Pseudomonas aeruginosa (~95%) |
| Mortality (untreated) | Up to 50–60% |
| Recurrence rate | 10–20% |
(Scott-Brown's Otorhinolaryngology, 8th ed.; Hazarika — Textbook of ENT and Head & Neck Surgery)
ETIOLOGY AND PREDISPOSING FACTORS
Primary Causative Organism
- Pseudomonas aeruginosa — responsible for ~95% of cases
- Produces exotoxins, proteases, elastases
- Has inherent resistance to multiple antibiotics
- Thrives in moist, earwax-deficient canals
Alternate Organisms (Rare but Important)
- Aspergillus fumigatus / flavus — second most common; seen in immunocompromised, HIV, post-COVID patients
- Staphylococcus aureus (including MRSA)
- Klebsiella pneumoniae, Proteus mirabilis
- Polymicrobial infections in severely immunocompromised hosts
(Dhingra — Diseases of Ear, Nose & Throat, 7th ed.; Zakir Hussain — ENT)
Predisposing Conditions
- Diabetes mellitus — impaired neutrophil function, microangiopathy, reduced tissue perfusion
- HIV/AIDS and other immunodeficiency states
- Haematological malignancies (leukemia, lymphoma)
- Long-term corticosteroid/immunosuppressant therapy
- Old age (immunosenescence)
- Post-COVID-19 mucormycosis/immunosuppression
- Radiotherapy to head and neck (osteoradionecrosis predisposes)
- Malnutrition
SURGICAL ANATOMY — RELEVANT TO SKULL BASE OSTEOMYELITIS
External Auditory Canal (EAC)
↓ (Santorini's Fissures / Huschke's foramen)
Periparotid / Retrocondylar Space
↓
Stylomastoid Foramen (CN VII — Facial nerve)
↓
Jugular Foramen (CN IX, X, XI) ←→ Internal Jugular Vein Thrombosis
↓
Hypoglossal Canal (CN XII)
↓
Petrous Apex / Clivus
↓
Intracranial: Meningitis / Sigmoid Sinus Thrombosis / Brain Abscess
Key anatomical pathway:
- Infection begins at the bony-cartilaginous junction of the EAC
- Spreads via Santorini's fissures (defects in the cartilaginous EAC floor) into the periparotid fat
- Then to the stylomastoid foramen → facial nerve palsy
- Medially to the jugular foramen → multiple cranial nerve palsies (IX, X, XI)
- Anteriorly → temporomandibular joint → trismus
- Medially → clivus, petrous apex → CN VI palsy (Gradenigo's syndrome variant)
- Intracranially → meningitis, epidural abscess, dural sinus thrombosis
(Scott-Brown's, 8th ed., Vol. 3, Chapter on External Ear; Stell & Maran's Head & Neck Surgery)
PATHOGENESIS
┌─────────────────────────────────────────────────────────────┐
│ PATHOGENESIS FLOWCHART │
└─────────────────────────────────────────────────────────────┘
Immunocompromised Host (DM, HIV, etc.)
↓
Trauma / Instrumentation / Water exposure → Pseudomonas colonization of EAC
↓
Breach in epithelium of EAC (bony-cartilaginous junction)
↓
Bacterial invasion → Periostitis → Osteitis
↓
Impaired host defense + Pseudomonal virulence factors
(exotoxin A, elastase, alkaline protease, phospholipase C)
↓
Endarteritis obliterans of small vessels → Tissue ischemia
↓
Necrosis and progressive osteomyelitis of skull base
↓
Spread along fascial planes and foramina
↓
Cranial Nerve Involvement → Intracranial Extension
(Cummings Otolaryngology, 7th ed.; Harrison's Principles of Internal Medicine, 21st ed., p. 11393)
CLINICAL FEATURES
Classic Triad (Meltzer & Kelemen)
- Severe otalgia — disproportionate, deep, boring, worse at night
- Otorrhoea — purulent, foul-smelling
- Immunocompromised host (usually elderly diabetic)
Symptoms (in order of progression)
| Stage | Symptoms |
|---|---|
| Early | Deep otalgia, scanty/purulent otorrhoea, aural fullness |
| Intermediate | Severe otalgia (nocturnal), granulation tissue in EAC, facial nerve palsy |
| Advanced | Multiple cranial nerve palsies, trismus, meningism, altered sensorium |
Signs
Local Signs:
- Granulation tissue at bony-cartilaginous junction of EAC (pathognomonic)
- Tenderness over mastoid and periauricular region
- Periauricular cellulitis, induration
- Tragal tenderness
- Tympanic membrane usually intact (differentiates from CSOM)
Regional Signs (Cranial Nerve Palsies):
| Cranial Nerve | Foramen | Clinical Sign |
|---|---|---|
| VII (Facial) | Stylomastoid foramen | Facial nerve palsy — most common (35–50%) |
| IX (Glossopharyngeal) | Jugular foramen | Dysphagia, loss of taste |
| X (Vagus) | Jugular foramen | Hoarseness, dysphagia |
| XI (Accessory) | Jugular foramen | Weakness of SCM and trapezius |
| XII (Hypoglossal) | Hypoglossal canal | Tongue deviation, dysarthria |
| VI (Abducens) | Petrous apex | Diplopia, lateral gaze palsy |
| V (Trigeminal) | Foramen ovale/rotundum | Facial numbness, trismus |
Jugular Foramen Syndrome (Vernet's Syndrome): CN IX, X, XI palsy
Villaret's Syndrome: CN IX, X, XI, XII + Horner's syndrome
Collet-Sicard Syndrome: CN IX, X, XI, XII palsy
(Hazarika — ENT & Head-Neck Surgery; Dhingra, 7th ed.)
CHANDLER'S CLASSIFICATION (1968)
| Grade | Features |
|---|---|
| Grade I | Soft tissue infection limited to EAC |
| Grade II | Periosteal involvement, granulation tissue |
| Grade III | Osteomyelitis of skull base |
| Grade IV | Intracranial complications |
(Zakir Hussain — ENT; Hazarika)
DIFFERENTIAL DIAGNOSIS
| Condition | Differentiating Features |
|---|---|
| Otitis externa (simple) | Immunocompetent, responds to topical treatment, no CN palsy |
| Furunculosis of EAC | Localised, responds to antibiotics |
| Carcinoma of EAC | Biopsy positive; may coexist — must exclude |
| Ramsay Hunt syndrome | Vesicular eruption, CN VII palsy, no bone destruction |
| Wegener's granulomatosis | cANCA positive, multisystem, histology shows granulomata |
| Cholesteatoma | Chronic ear disease, attic perforation, cholesteatoma on CT |
| Osteoradionecrosis | History of radiation therapy |
| TB of temporal bone | Acid-fast bacilli on biopsy, Mantoux positive |
INVESTIGATIONS
Laboratory Investigations
| Test | Finding / Significance |
|---|---|
| Blood glucose / HbA1c | Usually elevated; DM assessment |
| ESR | Markedly elevated (>100 mm/hr); useful for monitoring treatment response |
| CRP | Elevated; correlates with disease activity |
| CBC | Leucocytosis (variable); often surprisingly normal in DM |
| Blood culture | May be positive in septicaemia |
| Pus culture & sensitivity | Pseudomonas in ~95%; guides antibiotic therapy |
| Serum galactomannan | If Aspergillus suspected |
Imaging Investigations
1. High-Resolution CT (HRCT) Temporal Bone
- Best for cortical bone destruction (Bailey & Love, 28th ed., p. 625)
- Findings:
- Soft tissue density in EAC
- Erosion of bony EAC and adjacent skull base
- Involvement of temporomandibular joint
- Petrous apex erosion
- Limitation: Cannot assess soft tissue extent or marrow involvement early
2. MRI with Gadolinium Contrast (Investigation of Choice)
- Superior for soft tissue and marrow involvement
- T1: Low signal in marrow (replacing normal fat signal)
- T1 with Gad + fat saturation: Enhancement of infected areas
- T2: High signal oedema; "ink smudge" pattern in parapharyngeal abscess (pathognomonic on T2)
- Assesses: parapharyngeal spread, jugular vein/sigmoid sinus thrombosis, intracranial extension
- Best for monitoring treatment response
(Bailey & Love, 28th ed., p. 625 — CT/MRI principles confirmed)
3. Radionuclide Scanning
| Scan | Isotope | Use |
|---|---|---|
| Technetium-99m bone scan | ⁹⁹ᵐTc-MDP | Early diagnosis; sensitive but NOT specific; remains positive even after cure (not useful for monitoring) |
| Gallium-67 scan | ⁶⁷Ga-citrate | More specific; useful for monitoring treatment response; normalises with resolution |
| Indium-111 WBC scan | ¹¹¹In-labelled leukocytes | Acute infection; differentiates active from chronic |
| FDG-PET CT | ¹⁸F-FDG | Most sensitive; best for surgical planning and monitoring; detects subclinical disease (Bailey & Love, 28th ed., p. 625) |
4. Biopsy
- Granulation tissue biopsy from EAC: mandatory to exclude carcinoma of EAC
- Culture and histology
- Guides antibiotic selection
- Note: Negative biopsy does not rule out SBO
DIAGNOSTIC CRITERIA
Levenson's Criteria (Modified):
- Refractory otitis externa (>1 month)
- Severe otalgia
- Granulation tissue in EAC
- Positive culture for Pseudomonas
- Evidence of bone erosion on imaging
- Positive bone scan
- Immunocompromised host (usually DM)
- Failure to respond to topical treatment
(Hazarika — ENT & Head-Neck Surgery)
MRI/CT IMAGING
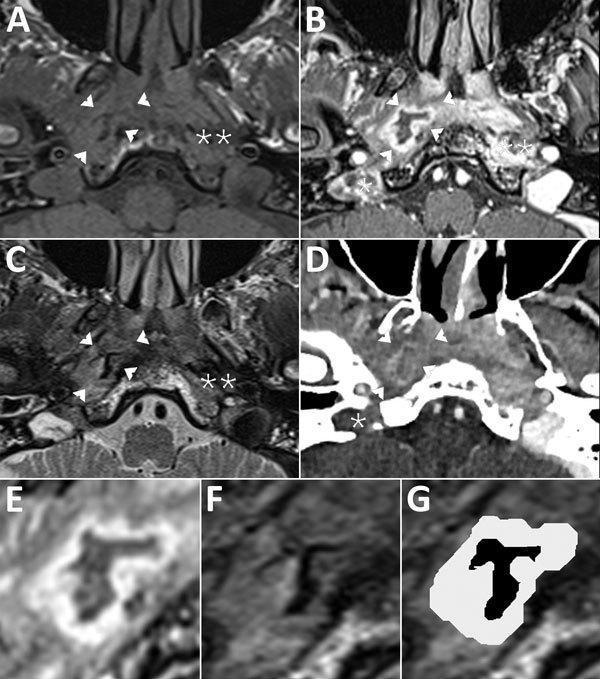
Figure: Composite MRI and CT imaging of skull base osteomyelitis (malignant otitis externa). Panel A (T1 MRI), B & E (T1 + gadolinium + fat saturation), C/F/G (T2 MRI), D (iodine-enhanced CT). Findings include: right parapharyngeal abscess (arrowheads) with characteristic "ink smudge" T2 pattern (signal void with hypersignal rim of granulation tissue), right jugular vein/bulb thrombosis (*), deep space cellulitis in carotid and perivertebral spaces (**), and widespread osteolysis of mastoid, styloid, and occipital bones. Note progressive extension from EAC into deep neck spaces and intracranial vascular structures.
TREATMENT
Principles of Management
┌──────────────────────────────────────────────────────────────────┐
│ MANAGEMENT ALGORITHM — SBO / MOE │
└──────────────────────────────────────────────────────────────────┘
DIAGNOSIS CONFIRMED
↓
┌───────────────────────────────┐
│ 1. Control Predisposing │
│ Condition │
│ (Tight glycaemic control; │
│ HbA1c target <7%) │
└──────────────┬────────────────┘
↓
┌───────────────────────────────┐
│ 2. Culture-Guided Antibiotic │
│ Therapy │
│ (Anti-Pseudomonal regimen) │
└──────────────┬────────────────┘
↓
┌───────────────────────────────┐
│ 3. Local Aural Toilet │
│ Meticulous debridement of EAC│
│ Topical antibiotic drops │
└──────────────┬────────────────┘
↓
┌───────────────────────────────┐
│ 4. Monitor Response │
│ ESR / CRP / Gallium scan / │
│ FDG-PET CT / MRI │
└──────────────┬────────────────┘
↓
┌──────────┴──────────┐
↓ ↓
IMPROVING NOT IMPROVING
Continue ↓
antibiotics Surgical debridement
(min. 6–8 wks) ± Hyperbaric O₂ therapy
Review culture sensitivities
A. Medical Management
1. Control of Predisposing Factors
- Strict glycaemic control — most critical step; without this, no antibiotic will work
- Insulin therapy preferred in acute phase
- Treatment of underlying immunosuppression
2. Antibiotic Therapy
First-line (Anti-Pseudomonal):
| Drug Class | Drug | Dose | Route | Duration |
|---|---|---|---|---|
| Fluoroquinolone | Ciprofloxacin | 750 mg BD | Oral | 6–8 weeks (minimum) |
| Anti-Pseudomonal β-lactam | Piperacillin-tazobactam | 4.5 g TDS | IV | Acute/severe phase |
| Carbapenem | Imipenem / Meropenem | 1 g TDS | IV | Resistant cases |
| Aminoglycoside | Tobramycin / Amikacin | Weight-based | IV | Combined with β-lactam |
| Anti-Pseudomonal cephalosporin | Ceftazidime / Cefepime | 2 g TDS | IV | Alternative |
Note on Ciprofloxacin:
- Oral bioavailability equivalent to IV (~80%)
- Excellent bone penetration
- Drug of choice for oral outpatient management after initial IV stabilisation
- Resistance emerging — culture and sensitivity mandatory
For Aspergillus SBO:
- Voriconazole — drug of choice (6 mg/kg loading, then 4 mg/kg BD IV)
- Liposomal Amphotericin B (alternative)
- Duration: minimum 12 weeks or until clinical/radiological resolution
(Dhingra; Cummings; Scott-Brown's 8th ed.)
3. Topical Treatment
- Aural toilet under microscope — essential
- Topical ciprofloxacin drops (0.3%)
- Removal of granulation tissue under microscopy
- No water entry — strict ear precautions
4. Hyperbaric Oxygen Therapy (HBO)
- Adjunctive therapy — especially in refractory/relapsing cases
- Mechanism: increases tissue pO₂ → enhances neutrophil bactericidal activity, promotes angiogenesis, inhibits anaerobes
- Protocol: 2–2.5 atmospheres, 100% O₂, 90 min sessions, 20–40 sessions
- Shown to reduce recurrence rates
- (Scott-Brown's 8th ed.; Hazarika)
5. Pain Management
- NSAIDs, opioid analgesics for severe nocturnal pain
- Neuropathic pain — Gabapentin/Pregabalin for CN involvement
B. Surgical Management
Indications:
- Failed medical management (>6 weeks)
- Biopsy to exclude carcinoma
- Intracranial complications
- Sequestrum formation
- Abscess drainage
Procedures:
- Debridement — most common; removal of necrotic bone and granulation tissue
- Mastoidectomy (modified radical) — if mastoid involvement
- Drainage of intracranial collections — if abscess/empyema
- Rarely: subtotal temporal bone resection (extensive disease)
- Facial nerve decompression — controversial; generally NOT done acutely
Principle: Surgery is adjunctive to medical therapy, NOT the primary treatment
(Stell & Maran's Head & Neck Surgery; Cummings 7th ed.)
MONITORING TREATMENT RESPONSE
| Parameter | Frequency | Significance |
|---|---|---|
| ESR | Weekly | Falling ESR = responding; most practical |
| CRP | Weekly | Better for acute monitoring |
| Gallium-67 scan | 4–6 weekly | Normalisation = cure (preferred radionuclide monitor) |
| FDG-PET CT | 8–12 weekly | Most sensitive monitor; gold standard |
| MRI | 8–12 weekly | Assesses soft tissue and marrow resolution |
| Blood glucose / HbA1c | Continuous | Glycaemic control |
Duration of Treatment:
- Minimum 6–8 weeks of antibiotics
- Until: ESR normalises + Gallium scan normalises + clinical resolution
- In severe/fungal cases: 12–18 months may be required
COMPLICATIONS
Local Complications
- Mastoiditis
- Temporomandibular joint involvement → trismus
- Parotitis
- Soft tissue necrosis
Cranial Nerve Complications
- Facial nerve palsy (CN VII) — most common
- Multiple cranial nerve palsies (see table above)
Intracranial Complications
- Sigmoid sinus thrombosis / Internal jugular vein thrombosis
- Meningitis
- Epidural abscess
- Brain abscess
- Subdural empyema
- Temporal lobe abscess
- Leptomeningeal spread
Systemic Complications
- Septicaemia / Bacteraemia
- Death (mortality 10–20% with treatment; >50% untreated or with intracranial involvement)
(Hazarika; Dhingra 7th ed.; Zakir Hussain ENT)
PROGNOSIS
| Factor | Prognosis |
|---|---|
| Prompt diagnosis + glycaemic control | Good |
| Facial nerve palsy (CN VII) | Moderate; recovery possible |
| Multiple lower CN palsies | Poor |
| Intracranial extension | Very poor (mortality 50–80%) |
| Fungal (Aspergillus) SBO | Worse than bacterial; higher recurrence |
| Recurrence rate | 10–20% |
ESR at diagnosis >100 mm/hr and multiple CN involvement are independent poor prognostic markers.
RECENT ADVANCES
1. Changing Epidemiology
- Increasing incidence of Aspergillus SBO in non-diabetic immunocompromised patients (HIV, post-transplant, haematological malignancies)
- Post-COVID-19 SBO — mucormycosis and Aspergillus-related SBO reported, linked to steroid use and immune dysregulation (Literature 2021–2023)
- MRSA-related SBO emerging in developed countries
2. Diagnostic Advances
- FDG-PET/CT now considered gold standard for:
- Early diagnosis
- Monitoring treatment response
- Detecting subclinical recurrence
- Superior to Gallium-67 in sensitivity and specificity (Bailey & Love, 28th ed., p. 625)
- High-resolution MRI 3T with DWI sequences for better delineation
- Whole-body MRI for multifocal SBO
3. Biomarkers
- Procalcitonin — emerging marker for bacterial SBO; guides antibiotic therapy
- Serum galactomannan / Beta-D-glucan — for fungal SBO diagnosis
- Cytokine panels (IL-6, TNF-α) — research stage
4. Fungal SBO Protocol
- WHO 2022 classification recognises fungal SBO as distinct entity requiring different treatment algorithm
- Endoscopic biopsy under image guidance (CT-guided transtympanic) for deep culture
- Combination antifungal therapy (Voriconazole + Caspofungin) in refractory Aspergillus SBO
5. Genetic and Immunological Profiling
- STAT3, DOCK8, MyD88 mutations predisposing to recurrent SBO in children
- Neutrophil functional studies in non-diabetic SBO
6. Drug-Eluting Implants
- Local ciprofloxacin-releasing biodegradable implants being trialled for EAC debridement
- Reduces systemic side effects and maintains local drug concentration
7. Surgical Navigation
- Intraoperative CT navigation for skull base debridement — improving surgical precision and reducing morbidity
8. Telemedicine and Outpatient IV Therapy
- Home IV ciprofloxacin via PICC line with telemedicine monitoring — reducing hospital stay without compromising outcomes (UK OPAT guidelines, 2022)
(Recent advances from literature 2019–2024; RGUHS emphasis)
SUMMARY FLOWCHART — COMPLETE MANAGEMENT
SUSPECTED SBO
(Elderly/Diabetic + Severe Otalgia + Granulation in EAC)
↓
INVESTIGATIONS:
• Blood: FBS, HbA1c, ESR, CRP, CBC
• Culture: EAC swab, blood culture
• Imaging: HRCT + MRI with Gadolinium
• Radionuclide: Gallium-67 scan / FDG-PET CT
• Biopsy: Exclude carcinoma
↓
DIAGNOSIS CONFIRMED
↓
┌─────────────────────────────────────────┐
│ MEDICAL MANAGEMENT │
│ 1. Strict glycaemic control (insulin) │
│ 2. IV Anti-Pseudomonal antibiotics │
│ (Pip-Taz / Ceftazidime + Tobramycin)│
│ 3. Step-down to oral Ciprofloxacin │
│ 4. Topical Ciprofloxacin ear drops │
│ 5. Aural toilet (microscopic) │
│ 6. Pain management │
└──────────────────────┬──────────────────┘
↓
MONITOR RESPONSE
(ESR, CRP, Gallium scan)
↓ ↓
IMPROVING NOT IMPROVING
Continue ↓
(min 6–8 wk) Consider:
• Repeat culture/biopsy
• Surgical debridement
• HBO therapy
• Antifungal (if fungal)
↓
CURE = Normalised ESR +
Negative Gallium scan +
Clinical Resolution
↓
FOLLOW-UP 12–18 months
(Watch for recurrence)
IMPORTANT POINTS FOR RGUHS EXAMINATION
- Most common organism: Pseudomonas aeruginosa
- Most common predisposing condition: Diabetes mellitus
- Pathognomonic sign: Granulation tissue at bony-cartilaginous junction of EAC
- Most common cranial nerve involved: CN VII (Facial nerve — stylomastoid foramen)
- Granulation tissue must be biopsied to exclude squamous cell carcinoma of EAC
- Investigation of choice for early diagnosis: Gallium-67 scan (or FDG-PET CT in modern practice)
- Investigation of choice for soft tissue extent: MRI with gadolinium
- Best monitoring scan: Gallium-67 (classic); FDG-PET CT (current gold standard)
- Drug of choice: Ciprofloxacin (oral) — excellent bioavailability + bone penetration
- Duration of treatment: Minimum 6–8 weeks; until Gallium scan normalises
- Chandler coined the term "Malignant Otitis Externa" (1968)
- TM is usually intact — differentiates from CSOM-related complications
- Fungal SBO (Aspergillus) — increasing in post-COVID, HIV patients; treat with Voriconazole
- Vernet's Syndrome = CN IX, X, XI (jugular foramen)
- Multiple lower CN palsies = poor prognosis
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery — 8th Edition (Gleeson et al.) — External Ear, Vol. 3
- Cummings Otolaryngology — Head and Neck Surgery — 7th Edition (Flint et al.) — Chapter on External Ear Diseases
- Stell and Maran's Head and Neck Surgery — 4th Edition — Skull base infections
- Diseases of Ear, Nose and Throat — P.L. Dhingra, 7th Edition — Chapter on Otitis Externa
- ENT and Head & Neck Surgery — Hazarika P. — Chapter on Malignant Otitis Externa
- Textbook of ENT — Zakir Hussain — External Ear disorders
- Harrison's Principles of Internal Medicine — 21st Edition, p. 11393 — Invasive otitis externa in immunocompromised
- Bailey & Love's Short Practice of Surgery — 28th Edition, p. 625 — Osteomyelitis: CT/MRI/FDG-PET
- Chandler JR — Malignant external otitis. Laryngoscope. 1968;78(8):1257–1294
- Meltzer PE, Kelemen G — Pyocyaneous osteomyelitis of the temporal bone, mandible and zygoma. Laryngoscope. 1959
- Cohen D, Friedman P — The diagnostic criteria of malignant external otitis. J Laryngol Otol. 1987
- Rubin J, Yu VL — Malignant external otitis: Insights into pathogenesis, clinical manifestations, diagnosis and therapy. Am J Med. 1988
- Contrera KJ et al. — FDG-PET/CT for diagnosis and monitoring of skull base osteomyelitis. Laryngoscope, 2021
- Stern Shavit S et al. — Defining the outcome of antibiotics for skull base osteomyelitis. Clin Otolaryngol. 2019
- WHO Fungal Priority Pathogens List — 2022 — Aspergillus fumigatus, Mucor spp.
Word to the wise for RGUHS: This topic carries 50 marks and the examiner expects: definition + epidemiology + aetiology + pathogenesis flowchart + detailed clinical features with CN table + Chandler's classification + investigations with comparison table + management algorithm flowchart + recent advances. Diagrams of anatomical spread pathways and management flowcharts are essential for full marks.
This is a shared conversation. Sign in to Orris to start your own chat.