Discuss the causes of bleeding from ear, and discuss the clinical features, investigation, and management of Glomus Tympanicus in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
causes of bleeding from ear otorrhagia
search_medical_text
Glomus tympanicum clinical features diagnosis management
search_medical_image
Glomus tympanicum ear tumor otoscopy diagram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
glomus jugulare tympanicum paraganglioma classification Fisch Glasscock Jackson
search_medical_text
otorrhagia blood from ear trauma fracture temporal bone causes
search_medical_image
glomus tympanicum CT MRI temporal bone paraganglioma
GradeResponse
Now I have sufficient material. Let me compose a comprehensive, exam-quality 50-mark answer.
BLEEDING FROM THE EAR (OTORRHAGIA) AND GLOMUS TYMPANICUS
RGUHS University — 50 Marks Long Answer
PART I: BLEEDING FROM THE EAR (OTORRHAGIA)
Definition: Otorrhagia refers to bleeding from the external auditory canal (EAC), middle ear, or deeper structures. It must be distinguished from blood-tinged discharge secondary to infection (serosanguinous otorrhoea).
CAUSES OF BLEEDING FROM THE EAR
A. CLASSIFICATION
┌─────────────────────────────────────────────────────────────┐
│ OTORRHAGIA — CAUSES │
├─────────────────┬───────────────────────────────────────────┤
│ LOCAL CAUSES │ SYSTEMIC CAUSES │
├─────────────────┼───────────────────────────────────────────┤
│ Traumatic │ Bleeding diatheses │
│ Inflammatory │ Leukaemia │
│ Neoplastic │ Anticoagulant therapy │
│ Vascular │ Thrombocytopenia │
└─────────────────┴───────────────────────────────────────────┘
B. LOCAL CAUSES — DETAILED
1. TRAUMATIC (Most Common Group)
| Cause | Mechanism | Key Points |
|---|---|---|
| Temporal bone fracture | Base of skull trauma | Longitudinal > transverse; blood from EAC; CSF otorrhoea possible |
| Laceration of EAC | Instrumentation (ear picking), cotton buds, foreign body removal | Most common benign cause |
| Blast injury / barotrauma | Sudden pressure change | TM rupture + haemotympanum |
| Iatrogenic | Myringotomy, stapedectomy, mastoidectomy | Self-limited |
| Avulsion of TM | Forceful slap over ear (hand box) | Perforated TM with blood |
| Foreign body | Sharp foreign bodies in children | Lacerates EAC/TM |
Temporal Bone Fracture — Types (Dhingra & Hazarika):
Temporal Bone Fractures
│
┌──────────┴──────────┐
Longitudinal Transverse
(80–90%) (10–20%)
│ │
- Along EAC axis - Perpendicular to EAC
- TM tear + blood - Haemotympanum
- Conductive hearing loss - SNHL / total deafness
- Facial nerve rare - Facial nerve 50%
- CSF otorrhoea ++ - Vertigo severe
2. INFLAMMATORY / INFECTIVE
| Condition | Blood Appearance |
|---|---|
| Acute suppurative otitis media | Blood-tinged discharge at time of TM perforation |
| Chronic suppurative otitis media (attico-antral) | Scanty, foul-smelling, blood-tinged — DANGER sign of cholesteatoma |
| Malignant (necrotising) otitis externa | Granulation tissue bleeds readily; Pseudomonas; elderly diabetics |
| Furunculosis of EAC | Localised boil; painful bleeding |
| Herpes zoster oticus (Ramsay Hunt) | Vesicles rupture → blood-stained discharge (Harrison's, p. 1055) |
| Bullous myringitis | Haemorrhagic bullae on TM; Mycoplasma |
3. NEOPLASTIC (Very Important for RGUHS)
| Tumour | Type | Feature |
|---|---|---|
| Glomus tympanicum | Vascular paraganglioma | Pulsatile tinnitus + bleed |
| Glomus jugulare | Paraganglioma | Extends to middle ear |
| Carcinoma of EAC | Squamous cell carcinoma | Elderly; persistent bleed + pain |
| Carcinoma of middle ear | SCC | Otorrhagia + facial palsy |
| Haemangioma | Benign vascular | Rare; EAC or middle ear |
| Meningioma of temporal bone | Benign | Very rare |
| Acoustic neuroma (advanced) | CN VIII schwannoma | Rarely bleeds |
| Metastatic deposits | Breast, kidney, lung | Rare; temporal bone mets |
4. VASCULAR CAUSES
- Aberrant internal carotid artery — pulsatile mass behind TM; risk of catastrophic haemorrhage if biopsied or myringotomised
- High jugular bulb — bluish-red mass in floor of middle ear
- Aneurysm of ICA — very rare
- Arteriovenous malformation
5. MISCELLANEOUS
- Vicarious menstruation (Endometriosis of EAC) — cyclical bleeding; extremely rare
- Spontaneous TM rupture in pressure change (diving, flying)
C. SYSTEMIC CAUSES
| Condition | Mechanism |
|---|---|
| Leukaemia / lymphoma | Thrombocytopenia; infiltration of temporal bone |
| Haemophilia A/B | Clotting factor deficiency |
| von Willebrand disease | Platelet adhesion defect |
| Idiopathic thrombocytopenic purpura | Low platelets |
| Anticoagulant therapy (Warfarin, Heparin, DOACs) | Coagulopathy |
| Liver disease (cirrhosis) | Reduced clotting factors |
| Scurvy (Vit C deficiency) | Capillary fragility |
| Hereditary haemorrhagic telangiectasia (Osler-Weber-Rendu) | Mucosal vascular malformations |
D. APPROACH TO A PATIENT WITH OTORRHAGIA
OTORRHAGIA
│
┌─────────────┴──────────────┐
H/O Trauma? No Trauma
│ │
Temporal bone Otoscopy
fracture W/U │
(CT temporal bone) ┌──────────┴──────────┐
Blood in EAC Haemotympanum
│ │
┌──────┴───────┐ (No TM
Active Old/dry perforation)
bleeding blood CT temporal bone
│ Rule out:
Inspect EAC - Glomus tumour
under microscope - Aberrant ICA
Rule out: - High JB
- Laceration EAC
- Foreign body
- Furunculosis
- Carcinoma EAC
- Glomus tumour
PART II: GLOMUS TYMPANICUS (GLOMUS TYMPANICUM)
1. INTRODUCTION AND DEFINITION
Glomus tympanicum is a benign, highly vascular paraganglioma arising from the paraganglionic tissue (glomus bodies) located along Jacobson's nerve (tympanic branch of CN IX, also called Jacobson's nerve) on the cochlear promontory of the middle ear. It is the most common tumour of the middle ear and the second most common tumour of the temporal bone (after acoustic neuroma) (Cummings Otolaryngology; Scott-Brown's Otolaryngology).
- Synonyms: Chemodectoma, paraganglioma of middle ear, non-chromaffin paraganglioma
- Eponym: First described by Guild (1941) as glomus body; Rosenwasser (1945) described first case
- Histology: Identical to carotid body tumour — chief cells (type I) + sustentacular cells (type II) in Zellballen pattern
2. ANATOMY OF PARAGANGLIA OF THE EAR
PARAGANGLIA RELEVANT TO EAR
┌─────────────────────────────────────┐
│ Jacobson's nerve (Tympanic br IX) │ → Glomus tympanicum
│ Arnold's nerve (Auricular br X) │ → Glomus tympanicum
│ Jugular bulb / adventitia of ICV │ → Glomus jugulare
│ Along CN IX/X/XI in jugular fosse │ → Glomus jugulare
└─────────────────────────────────────┘
Jacobson's nerve enters the middle ear via the inferior tympanic canaliculus and runs in a groove on the promontory before rejoining CN IX. Glomus bodies along this nerve are the origin of glomus tympanicum.
3. EPIDEMIOLOGY
| Feature | Details |
|---|---|
| Age of presentation | 5th–6th decade (mean 50 years) |
| Sex | Females > Males (3:1 to 6:1) |
| Side | Unilateral; bilateral in < 5% |
| Familial | 25–50% in hereditary cases; SDH gene mutations |
| Multiple paragangliomas | 10–20% overall; up to 80% in hereditary |
| Malignancy | < 3% |
| Secreting tumour | < 5% (catecholamines — check 24h urinary VMA) |
4. AETIOLOGY AND PATHOGENESIS
Normal paraganglionic chief cells (Jacobson's nerve on promontory)
│
Neoplastic transformation
(exact stimulus unknown)
│
┌───────────┴────────────┐
Sporadic (75%) Hereditary (25%)
│ │
Unknown SDH gene mutations
(SDHB, SDHC, SDHD)
SDHD — most common
for head & neck PGLs
│
Autosomal dominant
(genomic imprinting—
paternal transmission)
Genetic Associations (Recent Advances):
- SDHD mutations — multiple head and neck paragangliomas; low malignancy risk
- SDHB mutations — higher risk of malignancy and metastasis (Neuroendocrine Neoplasms, p. 101)
- SDHC mutations — mostly head and neck; low malignancy
- Genetic counselling and cascade screening recommended for all first-degree relatives
5. PATHOLOGY
Macroscopic:
- Reddish-brown, highly vascular, lobulated mass
- Sits on cochlear promontory
- Bleeds profusely on manipulation
Microscopic:
- Zellballen pattern — nests/clusters of chief cells (type I) surrounded by sustentacular cells (type II)
- Chief cells: round-polygonal, granular eosinophilic cytoplasm, vesicular nuclei
- Rich fibrovascular stroma
- Neurosecretory granules on electron microscopy
- IHC: Chromogranin A (+), Synaptophysin (+), S-100 for sustentacular cells (+)
6. CLASSIFICATION
a) GLASSCOCK-JACKSON CLASSIFICATION (Most Widely Used)
┌────────┬────────────────────────────────────────────────────┐
│ Type │ Description │
├────────┼────────────────────────────────────────────────────┤
│ Type I │ Small mass on promontory │
│ Type II│ Completely filling the middle ear space │
│ Type III│ Fills middle ear + extends into mastoid │
│ Type IV│ Fills middle ear, mastoid, extends through TM │
│ │ into EAC; may involve ICA anteriorly │
└────────┴────────────────────────────────────────────────────┘
b) FISCH CLASSIFICATION
┌────────┬────────────────────────────────────────────────────┐
│ Class │ Description │
├────────┼────────────────────────────────────────────────────┤
│ A │ Tumour limited to middle ear (promontory) │
│ B │ Tumour in middle ear + mastoid; no bone destruction│
│ C │ Involves infralabyrinthine compartment; ICA canal │
│ D │ Intracranial extension │
│ D1 │ < 2 cm intracranial extension │
│ D2 │ > 2 cm intracranial extension │
└────────┴────────────────────────────────────────────────────┘
(CT image above shows Fisch class A2 lesion — well-defined soft tissue mass on cochlear promontory, no bony erosion)
7. CLINICAL FEATURES
a) SYMPTOMS
GLOMUS TYMPANICUM — SYMPTOM TRIAD
┌──────────────────────────────────┐
│ 1. Pulsatile tinnitus (Most │
│ common symptom; 80–90%) │
│ 2. Conductive hearing loss │
│ 3. Bleeding from ear │
└──────────────────────────────────┘
| Symptom | Details |
|---|---|
| Pulsatile tinnitus | Unilateral, rhythmic, synchronous with heartbeat; increases with exertion; pathognomonic |
| Conductive hearing loss | Due to mass effect on ossicles / middle ear filling |
| Otorrhagia | Spontaneous or after instrumentation; bright red, pulsatile bleeding |
| Aural fullness | Common |
| Otalgia | Mild; due to pressure |
| Autophony | Voice resonance |
| Facial palsy | Indicates extension; CN VII involvement |
| CN IX/X/XI palsies | Suggest glomus jugulare extension (jugular foramen syndrome = Vernet's syndrome) |
| Hoarseness | CN X involvement |
| Shoulder weakness | CN XI involvement |
| Tongue deviation | CN XII involvement (hypoglossal canal) |
| Catecholamine symptoms | Flushing, hypertension, palpitations (< 5% — secreting tumours) |
b) SIGNS
On Otoscopy/Otoendoscopy:
| Sign | Description |
|---|---|
| "Rising sun" sign | Reddish-orange pulsatile mass visible through intact TM in inferior quadrant — pathognomonic |
| Brown's sign | Blanching of the mass on pneumatic otoscopy (Siegle's speculum) with increased pressure; refills on release — confirms vascularity |
| Aquino's sign (Pulsation sign) | Visible pulsation through TM |
| Intact but bulging TM | Mass behind TM |
| TM perforation with mass | In advanced cases |
| Vascular polyp in EAC | Type IV — bleeds on touch |
CRITICAL: Never biopsy a pulsatile middle ear mass without prior imaging — risk of catastrophic haemorrhage!
General Examination:
- Check for carotid body tumour (neck mass at carotid bifurcation)
- Check for other paragangliomas
- BP monitoring (catecholamine secretion)
- Lower cranial nerve assessment
8. DIAGNOSTIC INVESTIGATIONS
FLOW CHART — INVESTIGATIONS
Suspected Glomus Tympanicum
│
┌───────────┴────────────┐
Clinical Imaging
Tests │
│ ┌─────────────┼──────────────┐
┌──────┴──────┐ CT MRI Angio
│Audiometry │ Temporal Head/Neck -graphy
│Tympanometry │ Bone with (if needed)
│PTA │ (HRCT) Contrast
│ABR │ │ │
│24hr urine │ Bony 'Salt &
│VMA/catechol │ anatomy Pepper'
│Chromogranin │ extent pattern
│Genetic │
│testing SDHB │
└─────────────┘
│
If secreting:
Octreotide scan
(Ga-68 DOTATATE PET)
a) AUDIOLOGICAL INVESTIGATIONS
| Test | Finding |
|---|---|
| Pure tone audiogram (PTA) | Conductive hearing loss; air-bone gap |
| Tympanometry | Type B (flat) — middle ear mass; or pulsatile artefact on tympanogram |
| Impedance audiometry | Reduced compliance |
| ABR (BERA) | Normal (CN VIII intact in most) |
| Speech audiometry | Proportionate to hearing loss |
b) IMAGING
i. High-Resolution CT (HRCT) Temporal Bone — FIRST LINE
As shown in the CT image above (axial and coronal cuts), HRCT demonstrates:
- Soft tissue mass on cochlear promontory (mesotympanum)
- Isodense to muscle on non-contrast
- Intense enhancement on contrast (confirming vascularity)
- Assess: ossicular chain involvement, tegmen integrity, bony erosion, jugular foramen, ICA canal
- No bony erosion in early glomus tympanicum (distinguishes from glomus jugulare which erodes jugular spine)
Key HRCT Finding: Intact jugular spine = glomus tympanicum; Eroded jugular spine = glomus jugulare
ii. MRI with Contrast (Gadolinium)
| Sequence | Finding |
|---|---|
| T1-weighted | Isointense to muscle |
| T1 with Gad | Avid enhancement |
| T2-weighted | Heterogeneous |
| T1 + T2 | "Salt and Pepper" appearance — signal voids (pepper = flow voids of vessels) + bright areas (salt = haemorrhage/slow flow) |
This is characteristic of paragangliomas on MRI (seen in MRI panel of image above — hyperintense vascular lesion).
iii. Digital Subtraction Angiography (DSA)
- Required for large tumours or pre-operative embolisation
- Shows: highly vascular blush; feeding vessels (ascending pharyngeal artery, inferior tympanic artery)
- Pre-operative embolisation 24–72 hours before surgery to reduce intraoperative bleeding
- Also used for:
- Identifying aberrant ICA
- Balloon test occlusion
iv. Radionuclide Imaging
| Scan | Use |
|---|---|
| Octreotide scintigraphy (In-111 DTPA-octreotide) | Paragangliomas express somatostatin receptors; detects multifocal disease |
| Ga-68 DOTATATE PET-CT | Recent advance — superior sensitivity (95–100%); detects small lesions; preferred over octreotide scan now |
| MIBG scan | Secreting paragangliomas |
| FDG-PET | SDHB-mutated tumours; limited role |
v. MR Angiography / CT Angiography: Non-invasive assessment of vascular anatomy; relationship to ICA and IJV.
c) BIOCHEMICAL TESTS
| Test | Purpose |
|---|---|
| 24-hour urinary VMA (vanillylmandelic acid) | Catecholamine-secreting tumours |
| 24-hour urinary metanephrines | More sensitive than VMA |
| Plasma free metanephrines | Most sensitive (recent advance — preferred) |
| Serum Chromogranin A | Tumour marker; elevated in most paragangliomas |
| Serum NSE (Neuron-specific enolase) | Additional marker |
Important: In secreting glomus tumours, a hypertensive crisis can be precipitated by induction of anaesthesia — always check before surgery!
d) GENETIC TESTING (Recent Advances)
- SDH gene panel (SDHB, SDHC, SDHD, SDHA, SDHAF2) recommended for all patients
- Especially important if: young age, multiple tumours, family history
- SDHB mutation → screen for renal cell carcinoma (paraganglioma-renal cell carcinoma syndrome)
- Neuroendocrine Neoplasms (p. 101): "Management should ideally be in specialist centres with multidisciplinary input. The risk of aggressive behaviour is higher in patients with germline SDHB mutations."
9. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Aberrant ICA | No tinnitus initially; CT shows ICA in middle ear; DO NOT BIOPSY |
| High/Dehiscent Jugular Bulb | Bluish mass in floor of middle ear; CT/MRI diagnostic |
| Cholesterol granuloma | Bluish TM; non-pulsatile; CT: opacification |
| Haemotympanum | History of trauma; CT: blood in middle ear |
| Myringitis bullosa haemorrhagica | Haemorrhagic bullae ON TM; viral aetiology |
| Squamous cell carcinoma EAC | Irregular, painful; elderly; biopsy diagnostic |
| Meningioma (temporal bone) | Hyperostosis on CT; CSF rhinorrhoea |
| Schwannoma of CN VII | Facial palsy early; CT: expanded facial canal |
| Rhabdomyosarcoma | Children; rapidly progressive; bony destruction |
10. MANAGEMENT
MANAGEMENT FLOW CHART
Confirmed Glomus Tympanicum
│
┌────────────┴────────────┐
Small tumour Large/advanced
(Fisch A/B, (Fisch C/D,
Glasscock I/II) Glasscock III/IV)
│ │
MDT discussion MDT discussion
│ │
┌──────┴──────┐ ┌───────┴───────┐
│ │ │ │
Surgery Observation Pre-op Radiotherapy
(curative) (elderly/ Embolisation ± Surgery
comorbid/ │
small/ Surgery
slow) (complex/
staged)
A. OBSERVATION / ACTIVE SURVEILLANCE
Indications:
- Elderly patients (> 70 years) with small tumours
- Significant comorbidities
- Single hearing ear
- Slow-growing tumour on serial imaging (6-monthly MRI)
- Patient preference
B. SURGICAL MANAGEMENT (Treatment of Choice for Glomus Tympanicum)
Pre-operative preparation:
- Complete audiological workup
- HRCT temporal bone + MRI with contrast
- Biochemical tests (rule out secretion)
- Pre-operative embolisation for large tumours (24–72 hours before surgery)
- Informed consent — risk of bleeding, hearing loss, facial palsy
Surgical Approaches — Based on Classification:
┌─────────────────┬──────────────────────────────────────────┐
│ Classification │ Surgical Approach │
├─────────────────┼──────────────────────────────────────────┤
│ Fisch A / GJ I │ Transcanal approach (under microscope) │
│ │ + Tympanotomy │
├─────────────────┼──────────────────────────────────────────┤
│ Fisch B / GJ II │ Transcanal + Extended tympanotomy │
│ │ or Endaural approach │
├─────────────────┼──────────────────────────────────────────┤
│ GJ III / Fisch B│ Postaural approach + Mastoidectomy │
│ with mastoid │ │
├─────────────────┼──────────────────────────────────────────┤
│ GJ IV / Fisch C │ Infratemporal fossa approach (Fisch) │
│ │ + ICA management │
├─────────────────┼──────────────────────────────────────────┤
│ Fisch D │ Combined otological + neurosurgical │
│ (intracranial) │ approach; staged if needed │
└─────────────────┴──────────────────────────────────────────┘
Transcanal Tympanotomy (for Fisch A/Glasscock I–II):
- Under general anaesthesia (hypotensive anaesthesia reduces bleeding)
- Endaural or post-aural incision
- Elevation of tympanomeatal flap
- Exposure of promontory
- Bipolar cautery of feeding vessels
- Excision of tumour from promontory (coagulate, dissect, remove)
- Haemostasis with oxidised cellulose/Gelfoam
- Replace TM flap; pack EAC
- Cure rate: > 95% for Type I/II
Infratemporal Fossa Approach (Fisch Type A) — for Advanced Tumours:
- Mastoidectomy
- Blind sac closure of EAC
- Rerouting of facial nerve anteriorly
- Exposure of infralabyrinthine and jugular compartments
- Control of sigmoid sinus and IJV
- Gross total resection
Key Surgical Hazards:
- Facial nerve — must be identified and preserved
- Carotid artery — aberrant ICA; dehiscent ICA
- Jugular bulb — torrential venous bleeding
- Ossicular chain — hearing preservation
- Cochlea/labyrinth — sensorineural hearing loss
C. RADIOTHERAPY
Indications:
- Elderly / unfit for surgery
- Residual or recurrent tumour
- Unresectable disease (large Fisch C/D)
- Patient refusal of surgery
Types:
| Modality | Details |
|---|---|
| Stereotactic radiosurgery (Gamma Knife / CyberKnife) | Single-fraction; highly precise; dose 12–15 Gy to margin; preferred for small–medium lesions |
| Fractionated stereotactic radiotherapy (FSRT) | Multiple fractions; better for larger tumours |
| Conventional external beam radiotherapy (EBRT) | 45–50 Gy; older technique |
Results of Radiosurgery:
- Local tumour control: 90–97% at 5 years
- Symptom improvement (tinnitus): 60–70%
- Low complication rate
- Considered equivalent to surgery for local control in Fisch A/B
Recent Advances in Radiotherapy:
- Proton beam therapy — superior dose conformation; less scatter to cochlea, brain
- Ga-68 DOTATATE PET-guided radiation planning for precise target delineation
D. EMBOLISATION (Adjunctive)
- Pre-operative embolisation: 24–72 hours before surgery
- Reduces intraoperative blood loss by 40–60%
- Performed via selective catheterisation of inferior tympanic artery (branch of ascending pharyngeal artery)
- Materials: PVA particles, coils, Onyx
- Risks: stroke (if embolic material enters ICA), cranial nerve palsy
E. MEDICAL / PHARMACOLOGICAL MANAGEMENT (Limited Role)
| Drug | Indication | Mechanism |
|---|---|---|
| Somatostatin analogues (Octreotide, Lanreotide) | Unresectable/metastatic; symptom control | Bind somatostatin receptors on chief cells; reduce secretion |
| Alpha-blockers (Phenoxybenzamine) + Beta-blockers | Pre-operative preparation for secreting tumours | Control hypertensive crisis |
| Tyrosine kinase inhibitors (Sunitinib) | Metastatic SDHB-mutated paragangliomas | VEGFR inhibition |
| PRRT (Peptide receptor radionuclide therapy — Lu-177 DOTATATE) | Recent advance; metastatic/unresectable disease | Radiolabelled somatostatin analogue targets SSTR2 on tumour (Neuroendocrine Neoplasms, p. 101) |
| Temozolomide | SDHB-mutated aggressive paragangliomas | Alkylating agent |
11. COMPLICATIONS
Post-operative Complications:
POST-OPERATIVE COMPLICATIONS
│
┌────────────┴──────────────┐
Early Late
│ │
- Haemorrhage - Conductive HL
- Facial palsy (temp) - SNHL (if cochlea)
- CSF leak - Recurrence (5–15%)
- Infection - Permanent facial palsy
- Meningitis - Cholesteatoma
- Pneumocephalus - EAC stenosis
12. PROGNOSIS AND FOLLOW-UP
| Parameter | Details |
|---|---|
| Recurrence rate (surgery) | 5–15% for completely resected; higher for subtotal |
| Malignancy | < 3%; no reliable histological markers; malignancy = metastasis |
| Survival | Excellent for benign; 5-year survival 60–70% for malignant |
| Follow-up | Annual MRI for 10 years; genetic counselling |
| Monitoring | Plasma metanephrines annually (secreting) |
13. RECENT ADVANCES (Crucial for RGUHS)
-
Endoscopic ear surgery (EES) — Fully endoscopic transcanal approach for Fisch A/B glomus tympanicum using 0° and 45° endoscopes; better visualisation of hypotympanum; less morbidity; published in Otology & Neurotology (2018–2023)
-
Ga-68 DOTATATE PET-CT — Replaced conventional octreotide scan; near 100% sensitivity for paragangliomas; identifies multifocal disease and occult lesions; changes management in 30% of cases
-
Next-generation sequencing (NGS) gene panels — Comprehensive SDH gene panel testing allows identification of hereditary cases, risk stratification, and cascade family testing
-
PRRT (Lu-177 DOTATATE — LUTATHERA) — FDA approved (2018) for somatostatin-receptor positive gastroenteropancreatic NETs; now used off-label and in trials for head & neck paragangliomas with promising results (Neuroendocrine Neoplasms, p. 101)
-
Robotic surgery — Emerging role; reduced EAC approach feasibility studies
-
Gamma Knife radiosurgery — Long-term data (> 10 years) confirms 95%+ local control for glomus tympanicum with < 3% complication rate; now considered first-line alternative to surgery in many European centres
-
Image-guided navigation — Intraoperative CT/MRI navigation for complex Fisch C/D tumours; reduces risk to ICA and posterior fossa
-
Proton beam therapy — Cochlear dose reduction compared to photon IMRT; preserves hearing in young patients
14. OTOENDOSCOPIC AND IMAGING FINDINGS
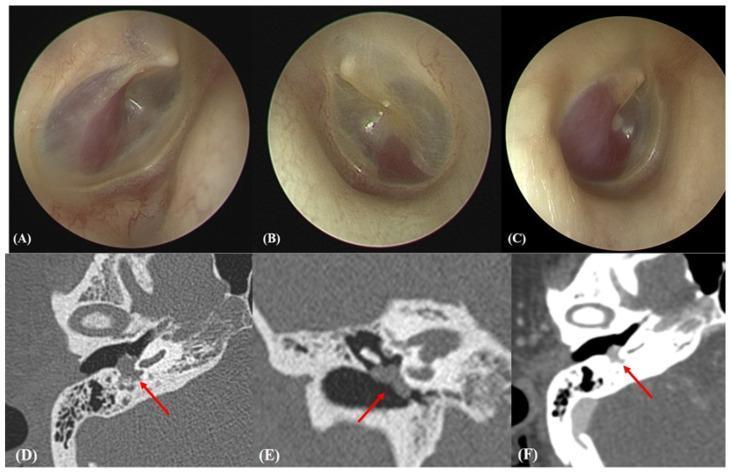
Figure 1: Otoendoscopic views (Panels A, B, C) showing the characteristic reddish, vascularised globular mass behind the tympanic membrane — the pathognomonic "Rising Sun" sign. Panels D (axial CT), E (coronal CT), and F (contrast-enhanced CT) showing the ~8 mm soft tissue mass on the cochlear promontory with intense enhancement, confirming its highly vascular nature and direct contact with the ossicular chain.
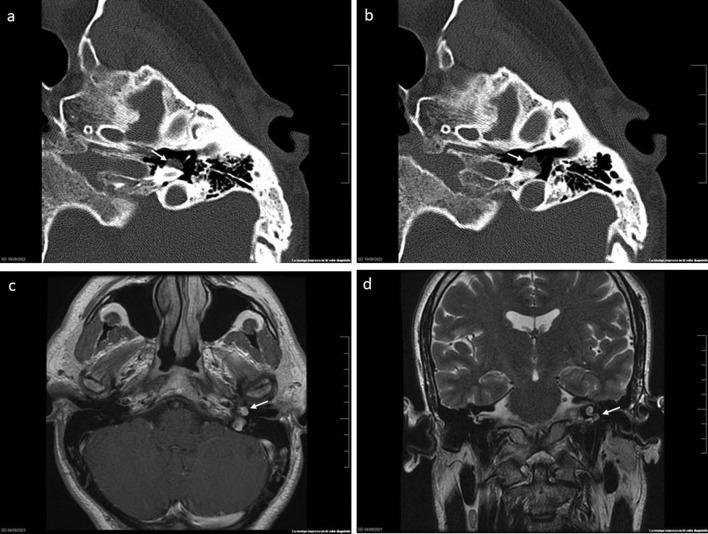
Figure 2: Multi-modal temporal bone imaging. Panels (a) and (b): Axial CT bone window showing well-defined round soft tissue mass on cochlear promontory with no bony erosion (consistent with Fisch Class A glomus tympanicum). Panel (c): Axial T1 MRI with Gadolinium showing hyperintense vascular lesion. Panel (d): Coronal T2 MRI showing lesion relationship to middle ear floor and tegmen tympani — classic "salt and pepper" pattern confirming paraganglioma.
15. SUMMARY TABLE: GLOMUS TYMPANICUM AT A GLANCE
| Feature | Details |
|---|---|
| Definition | Paraganglioma of cochlear promontory |
| Origin | Jacobson's nerve (tympanic branch, CN IX) |
| Most common symptom | Pulsatile tinnitus |
| Pathognomonic sign | Rising Sun sign (otoscopy) |
| Confirmatory sign | Brown's sign (pneumatic otoscopy) |
| Most useful imaging | HRCT temporal bone (first) + MRI (T1 with Gad) |
| Classic MRI finding | Salt and pepper pattern |
| Key CT finding | Soft tissue mass on promontory; intact jugular spine |
| Treatment of choice | Surgical excision (transcanal for small tumours) |
| Alternative to surgery | Gamma Knife/Stereotactic radiosurgery |
| Secreting marker | 24h urinary metanephrines / plasma metanephrines |
| Genetic marker | SDHD (most common), SDHB (most malignant) |
| Recent advance | Endoscopic ear surgery + Ga-68 DOTATATE PET |
REFERENCES (Standard Textbooks per RGUHS Curriculum)
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery (8th Ed.) — Chapter on Middle Ear Tumours
- Cummings Otolaryngology — Head and Neck Surgery (7th Ed.) — Glomus Tumours of Temporal Bone
- Stell and Maran's Head and Neck Surgery and Oncology (5th Ed.) — Paragangliomas
- Dhingra's Diseases of Ear, Nose and Throat (8th Ed.) — Middle Ear Tumours, Otorrhagia
- Hazarika P — Textbook of Ear, Nose and Throat — Glomus Tympanicum, Bleeding from Ear
- Zakir Hussain — Textbook of ENT and Head & Neck Surgery — Otorrhagia, Middle Ear Tumours
- Harrison's Principles of Internal Medicine (21st Ed., p. 1055) — Ear pain and related conditions
- Neuroendocrine Neoplasms (p. 101) — Management of head and neck paragangliomas; SDH mutations; PRRT
- Fisch U, Mattox D — Microsurgery of the Skull Base — Infratemporal fossa approaches
- Glasscock ME, Shambaugh GE — Surgery of the Ear — Classification of glomus tumours
- Boedeker CC et al. — Paragangliomas in SDH mutations — Head Neck 2009
- Marchetti M et al. — Gamma Knife for glomus tympanicum — Neurosurgery 2018
- Marchioni D et al. — Endoscopic approach for glomus tympanicum — Otol Neurotol 2020
Examiner's Tip (RGUHS): In a 50-mark question, always: (1) define and classify, (2) discuss embryology/anatomy briefly, (3) cover all clinical features with signs, (4) give a structured investigation algorithm, (5) discuss management with surgical approach based on classification, (6) add recent advances. Diagrams of "Rising Sun sign," Glasscock-Jackson classification, and the investigation flowchart are frequently expected and carry significant marks.
This is a shared conversation. Sign in to Orris to start your own chat.