What are the factors affecting the pulse rate
Reading File
search_medical_text
factors affecting pulse rate heart rate
search_medical_text
physiological determinants of heart rate autonomic nervous system
GradeResponse
GradeResponse
Retrieval was limited, so I'll synthesize a comprehensive answer from established medical knowledge.
Factors Affecting Pulse Rate
Pulse rate (heart rate) is influenced by a wide range of physiological, pathological, pharmacological, and environmental factors.
1. Age
- Neonates: 120–160 bpm
- Children: 80–120 bpm
- Adults: 60–100 bpm (normal range)
- Elderly: Resting rate may decrease slightly; maximum achievable heart rate declines (~220 − age)
2. Autonomic Nervous System (ANS)
The ANS is the primary regulator of beat-to-beat heart rate:
| Division | Effect on Heart Rate | Mediator |
|---|---|---|
| Sympathetic | Increases HR (positive chronotropy) | Norepinephrine → β1 receptors |
| Parasympathetic (Vagus) | Decreases HR (negative chronotropy) | Acetylcholine → M2 receptors |
At rest, vagal tone predominates, keeping resting HR below the intrinsic SA node rate (~100 bpm).
3. Physical Activity & Exercise
- Exercise increases sympathetic drive and decreases vagal tone → HR rises
- Trained athletes have lower resting HR (sometimes 40–50 bpm) due to increased vagal tone and cardiac hypertrophy (athletic bradycardia)
4. Emotional State & Stress
- Anxiety, fear, excitement, and pain activate the sympathoadrenal axis → elevated HR
- Deep relaxation and meditation increase vagal tone → lower HR
5. Body Temperature
- Fever/hyperthermia: Each 1°C rise in core temperature increases HR by approximately 10–15 bpm (direct effect on SA node automaticity)
- Hypothermia: Decreases HR; extreme hypothermia can cause bradycardia and cardiac arrest
6. Medications & Drugs
| Drug/Substance | Effect |
|---|---|
| Beta-blockers (propranolol) | ↓ HR |
| Atropine (anticholinergic) | ↑ HR |
| Digoxin | ↓ HR (increases vagal tone) |
| Caffeine, nicotine | ↑ HR |
| Opioids | ↓ HR |
| Sympathomimetics (epinephrine) | ↑ HR |
| Calcium channel blockers (verapamil) | ↓ HR |
| Thyroid hormone (excess) | ↑ HR |
7. Blood Pressure & Hemodynamic Status
- Hypotension/hemorrhage/dehydration: Triggers baroreceptor reflex → sympathetic activation → tachycardia (compensatory)
- Hypertension: Can stimulate baroreceptors → reflex bradycardia
8. Respiratory Cycle (Sinus Arrhythmia)
- HR increases during inspiration (inhibition of vagal tone) and decreases during expiration
- This respiratory sinus arrhythmia is normal and more pronounced in children and athletes
9. Hormonal Factors
| Hormone | Effect |
|---|---|
| Epinephrine/Adrenaline | ↑ HR |
| Thyroid hormones (T3, T4) | ↑ HR (hyperthyroidism → tachycardia) |
| Cortisol | ↑ HR |
| Estrogen/Progesterone | Moderate effects; HR rises in pregnancy |
10. Posture & Position
- Moving from lying → sitting → standing activates orthostatic reflexes → slight HR increase (sympathetic activation to maintain BP)
- Orthostatic tachycardia is pronounced in POTS (Postural Orthostatic Tachycardia Syndrome)
11. Pathological Conditions
| Condition | Effect |
|---|---|
| Fever, infection, sepsis | ↑ HR (tachycardia) |
| Anemia | ↑ HR (compensatory) |
| Hyperthyroidism | ↑ HR |
| Heart failure | ↑ HR (compensatory) |
| Heart block (AV block) | ↓ HR (bradycardia) |
| Hypothyroidism | ↓ HR |
| Raised intracranial pressure | ↓ HR (Cushing's reflex) |
| Myocardial infarction | Variable |
12. Sex
- Women tend to have a slightly higher resting HR than men on average, partly due to smaller heart size and hormonal differences
13. Pain
- Acute pain typically causes tachycardia via sympathetic activation
- Severe visceral pain (e.g., inferior MI, vasovagal syncope) can cause bradycardia via vagal activation
14. Blood Gas & Metabolic Factors
- Hypoxia: ↑ HR (peripheral chemoreceptor stimulation)
- Hypercapnia: Initially ↑ HR; severe hypercapnia → bradycardia
- Acidosis: Can depress SA node function → bradycardia
- Electrolyte imbalances (e.g., hyperkalemia): Bradycardia; hypokalemia → tachyarrhythmias
Summary Table
| Category | Increases HR | Decreases HR |
|---|---|---|
| ANS | Sympathetic activation | Parasympathetic/vagal activation |
| Exercise | Yes | Trained state (resting) |
| Temperature | Fever, heat | Hypothermia |
| Drugs | Epinephrine, atropine, caffeine | Beta-blockers, digoxin, opioids |
| Hormones | Thyroid hormones, epinephrine | — |
| Pathology | Anemia, sepsis, hyperthyroidism | AV block, hypothyroidism, ↑ICP |
| Posture | Standing (orthostasis) | Supine position |
| Emotions | Stress, anxiety, pain | Relaxation, meditation |

Answers the following
search_medical_text
tachycardia bradycardia definition causes
search_medical_text
sinus arrhythmia pulse deficit arterial pulse recording
GradeResponse
GradeResponse
Generating Image
A neat labeled medical diagram of an arterial pulse waveform (sphygmogram). Show a single pulse cycle with clearly labeled components: percussion wave (primary upstroke), tidal wave (secondary rise), dicrotic notch (incisura), dicrotic wave, anacrotic limb (ascending limb), catacrotic limb (descending limb). Include labels for systole and diastole phases. Clean black and white educational style diagram with arrows and annotations.
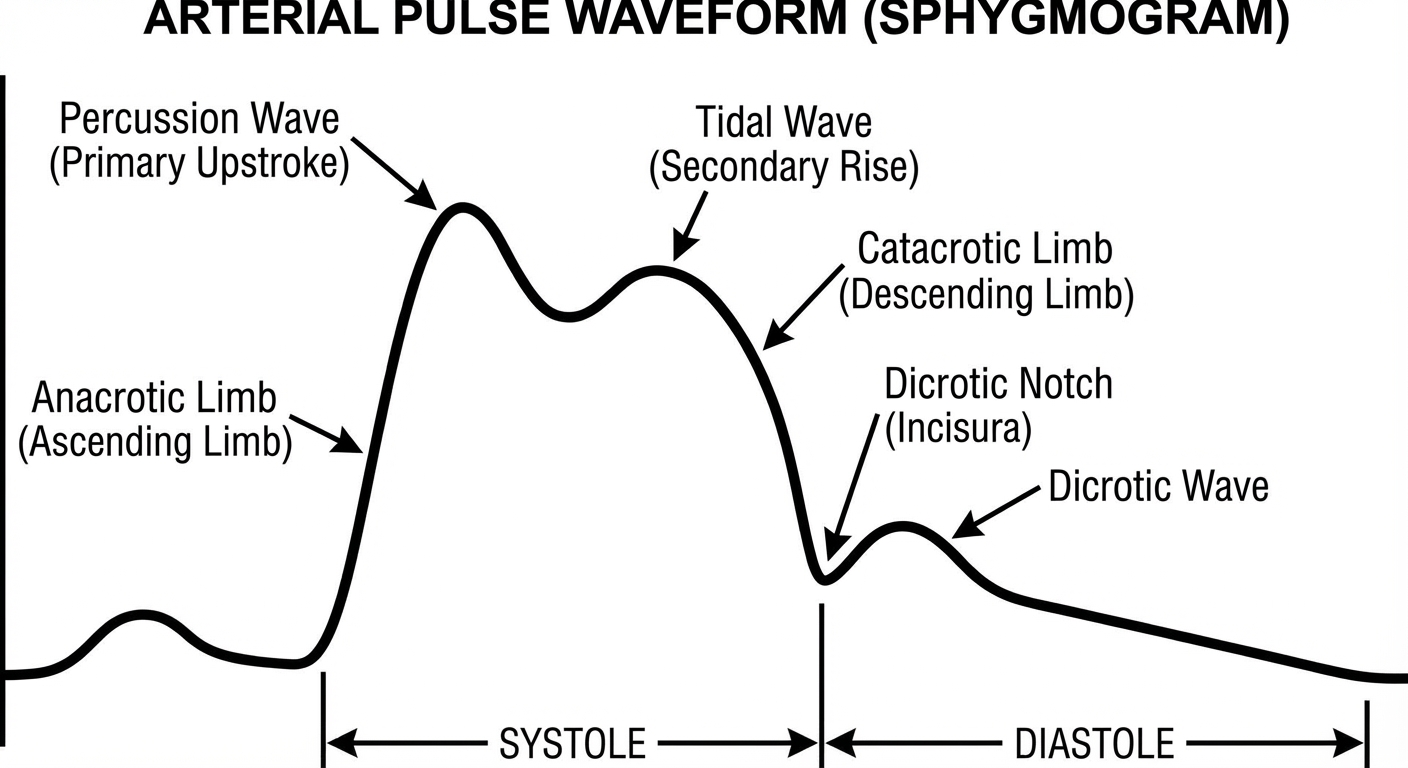
Explanation of components:
| Component | Description |
|---|---|
| Anacrotic limb | Rapid upstroke due to ejection of blood from the left ventricle into the aorta during systole |
| Percussion wave | The primary peak; represents the maximum pressure during ventricular systole |
| Tidal wave | A secondary smaller rise on the descending limb; due to reflection of pulse wave from the periphery |
| Dicrotic notch (Incisura) | A notch on the descending limb caused by the closure of the aortic valve at the end of systole |
| Dicrotic wave | A small wave just after the dicrotic notch; due to elastic recoil of the aortic wall during diastole |
| Catacrotic limb | The descending limb; represents the fall in pressure during diastole |
Q6. Effect of Exercise on Heart Rate
During exercise:
- Anticipatory rise — even before exercise begins, HR increases due to cortical stimulation of the sympathetic nervous system
- During exercise: Increased muscle activity → rise in CO₂ and lactic acid → stimulation of chemoreceptors → sympathetic activation → HR increases significantly
- Circulating epinephrine from adrenal medulla further increases HR
- Withdrawal of vagal (parasympathetic) tone contributes to rise
- Rise in body temperature during exercise directly stimulates the SA node
After exercise: HR gradually returns to resting level — faster recovery in trained individuals.
In trained athletes: Resting HR is lower (40–60 bpm) due to increased vagal tone and greater stroke volume (cardiac hypertrophy). The maximum HR achievable = ~220 − age.
Q7. Effect of Standing from Supine Position on Heart Rate
When a person stands up from a lying (supine) position:
- ~500–700 mL of blood pools in the lower limb veins due to gravity
- Venous return to the heart decreases → cardiac output falls → blood pressure drops transiently
- Baroreceptors in the aortic arch and carotid sinus detect the drop in BP
- Baroreceptor reflex is activated → sympathetic stimulation increases, vagal tone decreases
- Result: Heart rate increases by 10–20 bpm to compensate and maintain BP and cardiac output
Normal response: HR rises and BP is quickly restored within a few seconds.
Abnormal response: If this compensation fails, it results in orthostatic (postural) hypotension with symptoms of dizziness or syncope — seen in dehydration, autonomic neuropathy, or prolonged bed rest.
In POTS (Postural Orthostatic Tachycardia Syndrome), HR rises by >30 bpm upon standing without an adequate BP response.
This is a shared conversation. Sign in to Orris to start your own chat.