Give me a detailed brief on SDH so that I don't look dumb infront of the neurosurgeon
Reading File
search_medical_text
subdural hematoma pathophysiology classification acute chronic
search_medical_text
subdural hematoma clinical presentation diagnosis CT imaging management surgery
search_medical_image
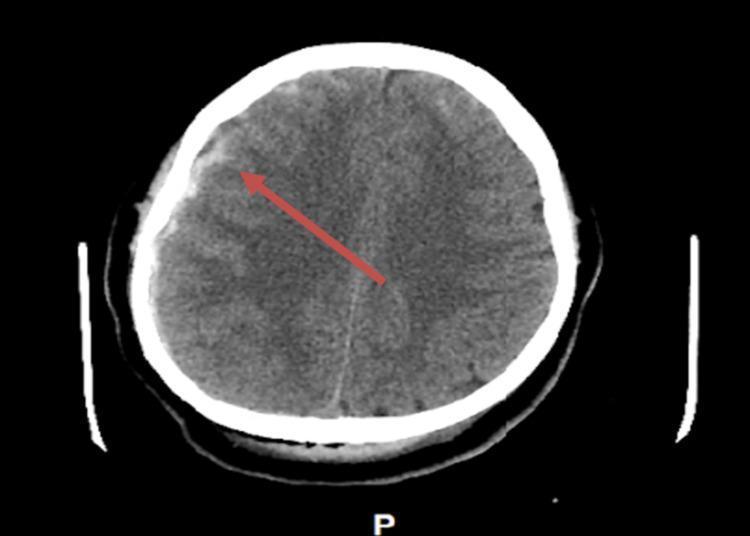
subdural hematoma CT scan crescent hyperdense
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive brief on Subdural Hematoma (SDH) that will hold up in front of a neurosurgeon.
Subdural Hematoma (SDH) — Clinical Brief
What Is It?
A subdural hematoma is a collection of blood in the subdural space — between the dura mater and the arachnoid mater. It is not within the brain parenchyma itself, but the mass effect it exerts on the underlying brain is what makes it dangerous.
Pathophysiology
The classic mechanism involves tearing of bridging veins that run from the cortical surface across the subdural space to the dural sinuses. When the brain moves relative to the skull (acceleration-deceleration), these veins shear. Because venous pressure is low, bleeding is slower than in an epidural hematoma — but it accumulates in a potentially large crescent-shaped space.
Key points:
- No direct trauma required in the elderly or anticoagulated patients — acceleration forces alone (e.g., whiplash) can be sufficient
- Elderly and cerebral atrophy: the brain shrinks away from the skull, stretching bridging veins further and making them more susceptible to minor trauma
- Anticoagulants / antiplatelets: dramatically increase risk and severity
Classification by Time Course
| Type | Time from Injury | CT Appearance | Key Features |
|---|---|---|---|
| Acute | 0–3 days | Hyperdense (bright white) crescent | Most symptomatic; high mortality |
| Subacute | 3–21 days | Isodense (can be hard to see) | May be missed on CT |
| Chronic | >21 days | Hypodense (dark) crescent | Often elderly, trivial/no recalled trauma |
The blood evolves: fresh clot is hyperdense → proteins lyse → becomes isodense → liquefies to hypodense. This is critical for dating the injury.
Clinical Presentation
Acute SDH
- Most patients are drowsy or comatose from the moment of injury
- Up to one-third have a lucid interval (minutes to hours) before deterioration
- Unilateral headache on the side of the hematoma
- Ipsilateral pupil dilation (CN III compression from uncal herniation)
- Contralateral hemiparesis (or ipsilateral if Kernohan's notch phenomenon)
- Stupor, coma, and bilateral pupillary changes = late/impending herniation
Subacute SDH
- Gradual neurological decline over days
- Headache, confusion, personality change
Chronic SDH
- Often presents insidiously: mild cognitive decline, gait disturbance, headache
- Easily mistaken for dementia, stroke, or normal pressure hydrocephalus
- Patient (or family) may not recall a trauma — "minor fall a few weeks ago"
Imaging
CT Head (Non-Contrast) — First-Line
The workhorse of SDH diagnosis. Fast, widely available, no contrast needed.
Key CT findings to know:
- Shape: crescent/concave (follows brain contour) — contrast with epidural which is lenticular/biconvex
- Location: crosses suture lines (epidurals do not)
- Midline shift: measured at the level of the septum pellucidum/foramen of Monro
- Sulcal effacement: compression of cortical gyri
- Subfalcine herniation: cingulate gyrus shifts under the falx
- Uncal herniation: medial temporal lobe herniates over the tentorium
MRI
- Superior for subacute/isodense SDH where CT may miss it
- Better for detecting underlying cortical contusions or diffuse axonal injury
Differentiating SDH from EDH
| Feature | SDH | EDH (Epidural) |
|---|---|---|
| Source | Bridging veins (venous) | Middle meningeal artery (arterial) |
| Shape on CT | Crescent (concave) | Lens/biconvex |
| Crosses sutures? | Yes | No |
| Lucid interval | Possible | Classic (more reliable) |
| Associated skull fracture | Less common | Very common (temporal) |
| Age group | Elderly common | Young adults |
| Urgency | High | Extremely high (arterial) |
Management
Medical (Conservative) Indications
- Small SDH, neurologically intact, no significant midline shift
- Chronic SDH in asymptomatic patients
- Key interventions:
- Reverse anticoagulation immediately (Vitamin K, FFP, PCC, or idarucizumab depending on agent)
- ICP management: HOB 30°, osmotherapy (mannitol or hypertonic saline), avoid hypoxia/hypotension
- Seizure prophylaxis (especially acute SDH — Levetiracetam or Phenytoin)
- Serial CT monitoring
Surgical Indications (Neurosurgeon's Domain)
Operate when:
- Clot thickness >10 mm
- Midline shift >5 mm
- ICP >20 mmHg refractory to medical management
- Neurological deterioration regardless of clot size
- GCS drop of ≥2 points from injury
Surgical options:
| Procedure | Use Case |
|---|---|
| Burr hole craniotomy | Chronic/subacute liquefied SDH — bedside or OR |
| Craniotomy with evacuation | Acute SDH with solid clot — definitive |
| Decompressive craniectomy | Refractory ICP, severe brain swelling |
For chronic SDH, burr hole drainage is preferred — less invasive, often done under local anesthesia even in elderly patients. Recurrence rate ~10–20% and may require repeat drainage or a subdural drain.
Prognosis
- Acute SDH: mortality 40–60% in large series; survivors often have significant disability. Outcomes correlate with GCS at presentation, age, and time to surgery.
- Chronic SDH: generally good prognosis with drainage; most elderly patients return to baseline.
- Poor prognostic signs: bilateral fixed dilated pupils, GCS 3, age >65, significant cerebral atrophy, coagulopathy, midline shift >10 mm.
Things That Will Impress a Neurosurgeon
- Know the 4-5-10 rule for surgical criteria: clot >10 mm or shift >5 mm = operate; GCS drop >2 = operate regardless.
- Ask about membrane formation in chronic SDH — the outer and inner membranes that form around the collection are vascularized and contribute to re-accumulation (hence recurrence risk).
- Mention Markwalder grading scale — a 0–4 neurological grading scale for SDH severity.
- Recognize that isodense SDH on CT can be bilateral and the midline may appear deceptively normal because the shift cancels out — but sulci will still be effaced.
- Ask about the role of dexamethasone in chronic SDH — controversial, used in some centers to reduce membrane inflammation and aid resorption in non-surgical cases.
Sources: Harrison's Principles of Internal Medicine, 21st Edition (pp. 12565–12566); supplemented with established neurosurgical principles.
This is a shared conversation. Sign in to Orris to start your own chat.