Here is a comprehensive 50-mark answer structured according to RGUHS examination standards, drawing from Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, Stell & Maran's Head and Neck Surgery, Dhingra's Diseases of Ear Nose and Throat, Hazarika's Textbook of ENT, and Zakir Hussain's ENT, along with recent advances.
BLEEDING FROM THE EAR (OTORRHAGIA) AND GLOMUS TYMPANICUS
PART I: BLEEDING FROM THE EAR (OTORRHAGIA)
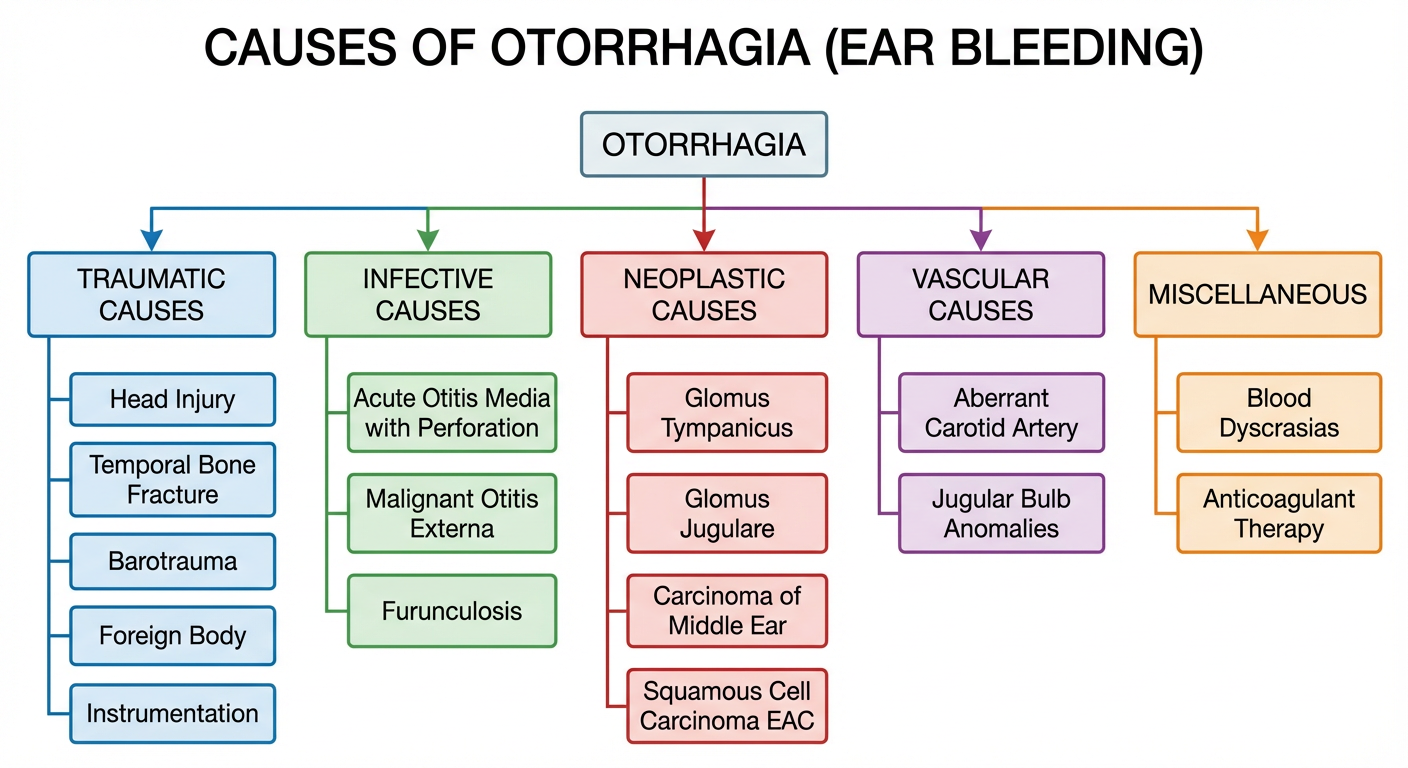
Definition (Dhingra, 7th ed.): Otorrhagia refers to bleeding from the external auditory canal (EAC), which may originate from the EAC itself, the tympanic membrane, or the middle ear, and occasionally from intracranial sources.
CAUSES OF BLEEDING FROM EAR
A. TRAUMATIC CAUSES (Most common overall)
| Cause | Mechanism | Key Features |
|---|
| Temporal bone fracture | RTA, blunt head trauma | Longitudinal (80%) → bloody otorrhagia + conductive hearing loss; Transverse → sensorineural HL |
| Barotrauma | Sudden pressure change (diving, flying) | Tympanic membrane rupture with haemotympanum |
| Foreign body | Sharp objects, insects | Laceration of EAC skin or TM |
| Blast injury | Explosions | TM perforation + haemotympanum |
| Instrumentation | Overzealous syringing, cotton buds | EAC lacerations |
| Slap injury / assault | Sudden compression of air column | Traumatic TM perforation |
Longitudinal temporal bone fracture is the most common cause of traumatic otorrhagia. Blood exits via a TM tear or EAC laceration. CSF otorrhoea may accompany it if the dura is torn — glucose testing distinguishes blood-stained CSF (Scott-Brown, 8th ed., Vol. 3, p. 3147).
B. INFECTIVE CAUSES
| Condition | Bleeding Mechanism |
|---|
| Acute Otitis Media (AOM) with spontaneous perforation | Hyperaemic, necrotic TM ruptures → serosanguinous discharge |
| Acute necrotising otitis media | Measles/scarlet fever → extensive TM necrosis → profuse bleeding |
| Malignant (necrotising) otitis externa | Pseudomonas aeruginosa in diabetics → granulation tissue at bone-cartilage junction → bleeding |
| Furunculosis of EAC | Staphylococcal abscess → haemorrhagic crusting |
| Herpes Zoster Oticus (Ramsay Hunt) | Vesicular haemorrhagic eruptions in EAC |
| Myringitis bullosa haemorrhagica | Viral haemorrhagic blebs on TM |
| Chronic Suppurative Otitis Media (CSOM) with granulations | Granulation tissue bleed |
C. NEOPLASTIC CAUSES (Clinically very important)
| Tumour | Features |
|---|
| Glomus Tympanicus | Pulsatile bleeding, pulsatile tinnitus, reddish mass on promontory |
| Glomus Jugulare | Extends from jugular fossa, more destructive, palsies of CN IX–XII |
| Squamous Cell Carcinoma of EAC/Middle Ear | Persistent bleeding, otalgia, facial nerve palsy |
| Carcinoma of middle ear cleft | Foul-smelling bloody discharge, deep otalgia |
| Haemangioma of EAC | Bright-red pulsatile bleeding |
| Ceruminoma/Adenocarcinoma | Rare, slow-growing with secondary haemorrhage |
D. VASCULAR CAUSES
- Aberrant internal carotid artery in middle ear — pulsatile bluish-red mass, catastrophic haemorrhage if traumatised
- High-riding jugular bulb — bluish mass in hypotympanum, mistaken for effusion
- Arteriovenous malformation (AVM) of temporal bone
- Aneurysm of petrous carotid artery (Cummings, 7th ed., p. 2094)
E. BLOOD DYSCRASIAS AND SYSTEMIC CAUSES
- Haemophilia, von Willebrand disease
- Thrombocytopenic purpura (ITP)
- Anticoagulant therapy (Warfarin, NOACs)
- Leukaemia (gingival and mucosal bleeds including ear)
- Osler-Weber-Rendu syndrome (hereditary haemorrhagic telangiectasia)
F. INTRACRANIAL / MISCELLANEOUS
- Encephalocele into middle ear — CSF otorrhoea may be haemorrhagic
- After mastoid surgery — reactionary or secondary haemorrhage
- Glomus tumour post-biopsy — catastrophic bleed
CLINICAL APPROACH TO OTORRHAGIA — DIAGNOSTIC FLOWCHART
BLEEDING FROM EAR
│
├── History: Trauma? Infection? Hearing loss? Pulsatile?
│
├── Traumatic → Otoscopy → TM tear? → Audiogram + HRCT Temporal Bone
│ → Exclude CSF with β2-transferrin test
│
├── Infective → Otoscopy → EAC/TM pathology → Culture + Sensitivity
│ → Treat accordingly
│
├── Pulsatile bleeding → Glomus tumour / Vascular anomaly
│ → Pneumatic otoscopy (Brown's sign)
│ → HRCT + MRI + MRA/DSA
│
└── No obvious cause + Persistent → Biopsy after imaging
→ Exclude carcinoma
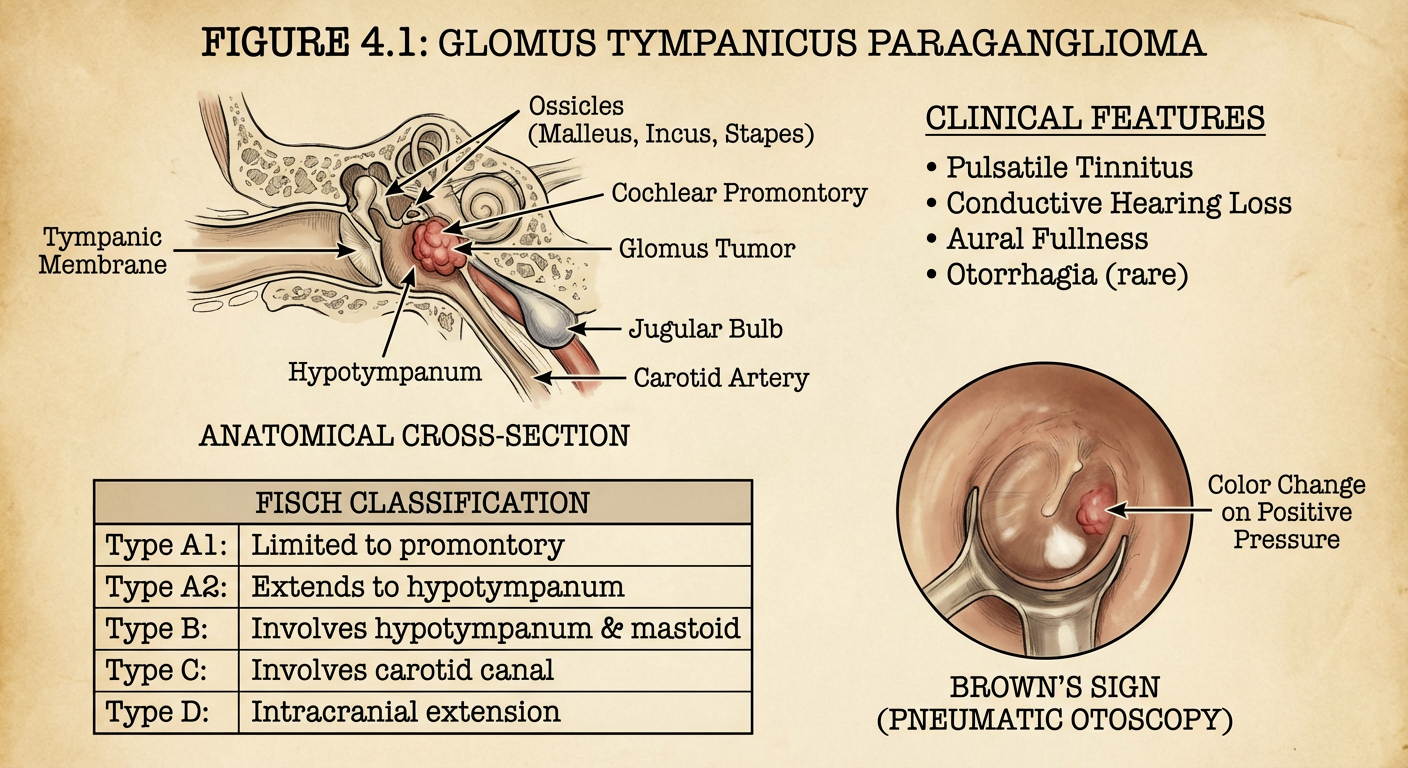
PART II: GLOMUS TYMPANICUS
INTRODUCTION AND HISTORICAL BACKGROUND
Glomus tumours of the ear are the most common benign tumours of the middle ear and the second most common tumours of the temporal bone (after acoustic neuroma). They are paragangliomas — highly vascular, slow-growing neoplasms arising from paraganglion cells (chemoreceptor cells) derived from neural crest tissue.
- Rosenwasser (1945) first described the jugulotympanic glomus body.
- Guild (1953) described the tympanic plexus (glomus tympanicum) and jugular adventitia (glomus jugulare) as the sites of origin.
- Glomus Tympanicus arises from the Jacobson's nerve (tympanic branch of CN IX) along the cochlear promontory (Scott-Brown, 8th ed.).
- Glomus Jugulare arises from the jugular fossa/adventitia of the jugular bulb.
Zakir Hussain's ENT classifies tympanojugular paragangliomas separately as they represent a continuum of the same pathological entity.
ANATOMY OF THE GLOMUS BODY
The normal glomus body (chemoreceptor tissue) in the middle ear is located:
- Along the tympanic branch of CN IX (Jacobson's nerve) on the cochlear promontory → gives rise to Glomus Tympanicus
- Along the auricular branch of CN X (Arnold's nerve) in the jugular fossa → gives rise to Glomus Jugulare
These cells are type-1 (chief) cells surrounded by sustentacular cells, richly supplied by the ascending pharyngeal artery, and capable of secreting catecholamines (10% of tumours are functional).
PATHOLOGY
- Gross: Reddish-brown, lobulated, highly vascular mass
- Microscopy: Nests of epithelioid chief cells (Zellballen pattern) in a richly vascular fibrous stroma; surrounded by sustentacular (S100+) cells
- Immunohistochemistry: Chief cells positive for chromogranin A, synaptophysin, NSE; sustentacular cells positive for S-100
- Malignancy: Rare (<5%); diagnosed by metastasis (to lymph nodes, lung, liver) NOT by histology alone (Cummings, 7th ed., Chapter 120)
- Genetics: 30% are hereditary; mutations in succinate dehydrogenase (SDH) genes — SDHB, SDHC, SDHD (Recent advances)
CLASSIFICATION
FISCH CLASSIFICATION (Most widely used — Hazarika, Dhingra, Cummings)
| Class | Description |
|---|
| Type A | Tumour limited to middle ear cleft (Glomus Tympanicus) |
| Type B | Tumour limited to tympanomastoid compartment, no infralabyrinthine compartment involvement |
| Type C | Tumour involving infralabyrinthine compartment; subdivided by carotid involvement: C1 (no carotid involvement), C2 (vertical carotid involvement), C3 (horizontal carotid involvement) |
| Type D | Intracranial extension: D1 (<2 cm), D2 (>2 cm) |
GLASSCOCK-JACKSON CLASSIFICATION (for Glomus Tympanicus specifically)
| Type | Extent |
|---|
| I | Small mass limited to promontory |
| II | Tumour completely filling middle ear |
| III | Tumour filling middle ear + extending into mastoid |
| IV | Tumour filling middle ear, mastoid, extending through TM into EAC ± anterior middle ear, jugular bulb involvement |
Glomus Tympanicus = Fisch Type A / Glasscock-Jackson Type I or II, confined to the middle ear, best prognosis (Scott-Brown, 8th ed., p. 3278).
EPIDEMIOLOGY
| Parameter | Data |
|---|
| Incidence | ~1 per 300,000 population |
| Age | Peak 5th–6th decade |
| Sex | Female predominance (F:M = 3:1 to 6:1) |
| Side | Unilateral; rarely bilateral (hereditary cases) |
| Hereditary | 10–30%; autosomal dominant with genomic imprinting |
| Multicentric | 10% sporadic; up to 40% hereditary |
| Functional | ~1–3% secrete catecholamines (hypertension crises possible) |
CLINICAL FEATURES
SYMPTOMS (Dhingra, 7th ed.; Hazarika; Stell & Maran)
1. Pulsatile Tinnitus (Most common presenting symptom — >80%)
- Rhythmic, synchronous with pulse
- Low-frequency, roaring quality
- Aggravated by exertion, relieved by carotid compression ipsilaterally (reduces arterial pressure) — Aquino's sign
- May cease with jugular vein compression — Branham's sign (more specific for AV fistula but noted)
2. Conductive Hearing Loss
- Progressive, unilateral
- Due to mass effect on ossicular chain or filling middle ear cavity
- Rarely sensorineural if cochlea is invaded (Fisch C/D)
3. Bleeding from the Ear (Otorrhagia)
- Spontaneous haemorrhagic discharge
- Brisk, pulsatile
- May occur after attempted biopsy → catastrophic haemorrhage if biopsy is taken without prior imaging (Zakir Hussain's ENT — strong caution against biopsy)
4. Aural Fullness
- Sensation of blockage in the ear
5. Otalgia
- Mild; deep-seated if erosion of bone present
6. Cranial Nerve Palsies (more Glomus Jugulare; rarely Tympanicus)
- CN VII (facial palsy) — indicates temporal bone extension
- CN IX, X, XI, XII — Jugular foramen syndrome (Vernet's syndrome) in advanced Glomus Jugulare
7. Catecholamine secretion (Functional Paraganglioma — 1–3%)
- Episodic hypertension, palpitations, sweating, headache
- Must be excluded before surgery or embolisation
SIGNS
1. Otoscopic Findings — Classical
- Reddish-blue or cherry-red pulsatile mass seen through the intact tympanic membrane in the anterior-inferior quadrant (over the cochlear promontory / hypotympanum)
- The mass may be visible as a vascular blush or complete tympanic filling
2. Brown's Sign (Pathognomonic)
On pneumatic otoscopy: Applying positive pressure causes blanching (pallor) of the reddish mass as blood is squeezed out; on releasing pressure, it re-flushes red (pulsatile). This blanching and pulsation with pneumatic pressure = Brown's sign (Stell & Maran, 5th ed.; Hazarika, 4th ed.).
3. Rising Sun Sign
- In hypotympanic tumour, a reddish glow visible below the annulus — like a rising sun — as the mass pushes up from below (Cummings, 7th ed.)
4. Aquino's Sign
- Pulsatile tinnitus decreases / ceases on compressing the ipsilateral carotid artery
5. Conductive Hearing Loss on tuning fork tests (Rinne negative, Weber lateralised to affected ear)
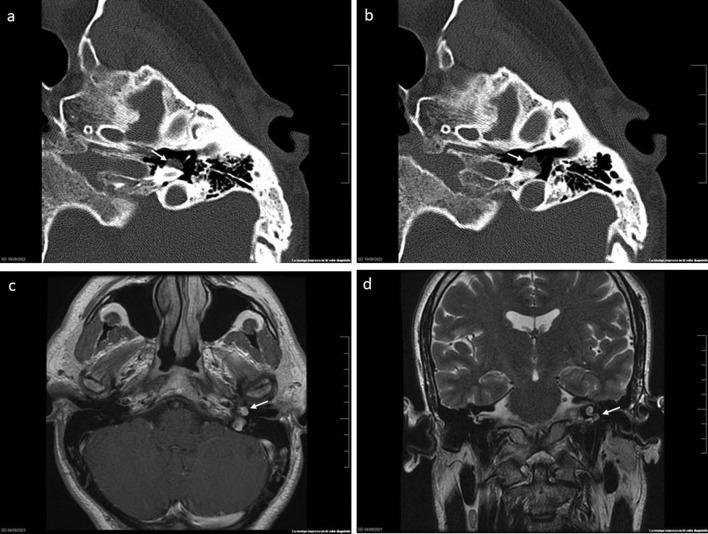
IMAGING OF GLOMUS TYMPANICUS
Multi-modal imaging: (a,b) Axial HRCT bone window — well-defined soft tissue mass on cochlear promontory with no bony erosion; (c) T1 MRI with contrast — hyperintense vascular lesion; (d) Coronal T2 MRI — relationship to tegmen tympani. Consistent with Fisch Type A2 Glomus Tympanicum.
INVESTIGATIONS
FLOWCHART OF INVESTIGATIONS
SUSPECTED GLOMUS TYMPANICUS
(Pulsatile tinnitus + reddish middle ear mass + Brown's sign)
│
├─── AUDIOMETRY
│ ├── Pure Tone Audiogram → Conductive hearing loss
│ └── Tympanometry → Pulsatile movements on tympanogram (Type B/As)
│
├─── IMAGING (Mandatory BEFORE biopsy)
│ ├── HRCT Temporal Bone (First line)
│ │ └── Soft tissue mass on promontory
│ │ No bony erosion in Tympanicus
│ │ Bony erosion suggests Jugulare
│ │
│ ├── MRI + Gadolinium (Second line)
│ │ ├── "Salt and pepper" appearance on T1 (large tumours)
│ │ │ [Flow voids = pepper; haemorrhage = salt]
│ │ └── Intense enhancement with contrast
│ │
│ └── MRA / DSA (if vascular anatomy needed pre-op)
│ └── Identifies feeding vessels
│ Permits pre-operative embolisation
│
├─── BIOCHEMICAL (Exclude functional tumour)
│ ├── 24-hour urine: VMA, metanephrines, catecholamines
│ └── Plasma metanephrines (more sensitive — Recent advances)
│
├─── NUCLEAR MEDICINE
│ ├── Octreotide scan (In-111 DTPA octreotide)
│ │ Paragangliomas express somatostatin receptors
│ └── 68-Ga DOTATATE PET-CT (Recent — Gold Standard)
│ Superior sensitivity for multicentric/metastatic disease
│
├─── GENETIC TESTING (Hereditary cases)
│ └── SDH gene mutations: SDHB, SDHC, SDHD
│ (Indicated in: young patients, bilateral, multicentric, FH)
│
└─── BIOPSY
CONTRAINDICATED without prior imaging
Only after vascular lesion excluded
AUDIOLOGICAL INVESTIGATIONS (in detail)
| Test | Finding in Glomus Tympanicus |
|---|
| Pure Tone Audiogram | Mild–moderate conductive hearing loss |
| Speech Audiogram | Reduced speech discrimination in advanced cases |
| Tympanometry | Type B (flat) or pulsatile Type As; pulsatile variation in compliance visible |
| OAE | Absent on affected side if conductive loss severe |
| BERA | Useful to exclude sensorineural component |
IMAGING CHARACTERISTICS
| Modality | Finding |
|---|
| HRCT Temporal Bone | Soft tissue mass on cochlear promontory; in Tympanicus — no bony erosion; irregular "moth-eaten" bone erosion = Jugulare |
| MRI T1 plain | Isointense to muscle; "salt-and-pepper" in large tumours (Jugulare) |
| MRI T1 Gad | Intense, homogeneous enhancement |
| MRI T2 | Hyperintense; flow voids in large tumours |
| DSA / Angiography | Vascular blush from ascending pharyngeal / inferior tympanic artery; used for embolisation planning |
| 68Ga-DOTATATE PET | Highly sensitive; identifies multicentric disease (Recent advance — Cummings 7th ed. update) |
DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|
| Aberrant ICA | Bluish (not red), no Brown's sign; catastrophic if biopsied; CT shows absent bony covering of carotid canal |
| High jugular bulb | Bluish-white mass in postero-inferior TM; no pulsation on otoscopy |
| Haemangioma of middle ear | Less pulsatile; CT — honeycomb bony pattern |
| Cholesterol granuloma | Bluish mass; non-pulsatile; CT — expansion of petrous apex |
| Secretory otitis media (Glue ear) | Amber/bluish TM; no pulsation; no Brown's sign |
| Carcinoma of middle ear | Irregular growth; bone destruction on CT; biopsy confirmatory |
| Meningioma | CT/MRI characteristics differ; no Brown's sign |
Zakir Hussain's ENT specifically emphasises that aberrant ICA must always be excluded before any middle ear exploration or biopsy.
MANAGEMENT OF GLOMUS TYMPANICUS
TREATMENT ALGORITHM
CONFIRMED GLOMUS TYMPANICUS (Fisch Type A / G-J Type I–IV)
│
┌─────────┴──────────┐
Functional? Non-functional
(catecholamine (majority)
secreting) │
│ │
Alpha-blocker Assess:
preoperatively - Age/fitness
(Phenoxybenzamine - Tumour size/extent
10–14 days) - Hearing status
- Patient preference
│
┌─────────────────┼──────────────┐
Type I/II Type III/IV Poor surgical
(Small/Medium) (Extended) candidate/elderly
│ │ │
SURGICAL SURGICAL + RADIOTHERAPY
(Transcanal/ Pre-op (Primary or
Tympanotomy) Embolisation adjuvant)
│ → Infratemporal
│ fossa approach
│ (Fisch Type A/B)
│
COMPLETE EXCISION → CURE
SURGICAL MANAGEMENT (Mainstay of Treatment)
PRE-OPERATIVE PREPARATION
- Exclude functional tumour — 24-hr urine VMA + plasma metanephrines
- If positive: Phenoxybenzamine (alpha-blocker) 10–14 days preoperatively
- Beta-blocker NEVER given first (risk of hypertensive crisis)
- Pre-operative embolisation (24–72 hours before surgery)
- Reduces intraoperative blood loss by 40–60%
- Via ascending pharyngeal artery (main feeder)
- Technique: Seldinger approach, superselective catheterisation, PVA particles / coils (Cummings, 7th ed., p. 2099)
- Cross-matching blood, ICU availability
- Audiometric baseline
- Facial nerve monitoring setup intraoperatively
SURGICAL APPROACHES (Based on Fisch Classification)
| Fisch Type | Approach | Key Steps |
|---|
| Type A (Glomus Tympanicus) | Transcanal tympanotomy (most cases) / Endaural | Elevation of tympanomeatal flap → tumour visualisation on promontory → bipolar coagulation → sharp dissection and removal |
| Type B | Extended tympanotomy + mastoidectomy | Canal wall up mastoidectomy → extended facial recess opening → tumour removal |
| Type C | Infratemporal fossa approach Type A (Fisch) | Preauricular extended incision; subtotal petrosectomy; ICA dissection; inferior petrous sinus ligation |
| Type D (intracranial) | Combined neurosurgical + skull base approach | Team: ENT skull base + neurosurgery |
TRANSCANAL APPROACH (Glomus Tympanicus — Step by Step)
(Hazarika, 4th ed.; Scott-Brown 8th ed.)
- General anaesthesia (hypotensive preferred — MAP 60–65 mmHg)
- Injection of 1% Lignocaine with 1:100,000 adrenaline — EAC infiltration
- Tympanomeatal flap elevation — posteriorly based, 6 o'clock to 12 o'clock
- Middle ear exploration — identify tumour on cochlear promontory
- Bipolar diathermy to coagulate feeding vessels (inferior tympanic artery = Jacobson's artery)
- Tumour dissection from the promontory — suction dissection + microsurgical technique
- Ossicular chain assessment and preservation where possible
- Haemostasis with Surgicel/Gelfoam
- TM flap repositioning + canal packing
Key surgical principle: Glomus Tympanicus is usually completely resectable with transcanal approach alone, with cure rates >95% (Cummings, 7th ed.; Stell & Maran).
RADIOTHERAPY
Indications:
- Elderly/medically unfit patients
- Residual/recurrent tumour post-surgery
- Unresectable disease (Fisch C3/D)
- Patient refusal for surgery
- Bilateral tumours (preserve hearing on better side)
Technique:
- Conventional external beam RT: 45–50 Gy in 25 fractions
- Stereotactic Radiosurgery (SRS) — Gamma Knife / CyberKnife (Recent advance)
- Marginal dose: 12–15 Gy to 50% isodose line
- Local control: 90–95% at 5 years
- Cranial nerve preservation superior to surgery
- Preferred for Fisch C/D tumours and elderly patients (Cummings, 7th ed., p. 2105)
Mechanism:
RT does NOT kill tumour cells directly; it causes obliterative endarteritis → fibrous replacement → tumour devascularisation and growth arrest (tumour is NOT cured by RT; it is controlled).
WATCHFUL WAITING (Observation)
- Elderly patients with small, asymptomatic Fisch Type A tumours
- Serial HRCT/MRI every 1–2 years
- Tumours are slow-growing (mean growth rate 0.8 mm/year)
- Re-evaluate if symptoms progress (Hazarika, 4th ed.)
COMPLICATIONS OF SURGERY
| Complication | Comment |
|---|
| Intraoperative haemorrhage | Most feared; pre-op embolisation reduces risk |
| Facial nerve injury | Requires meticulous monitoring; incidence 5–10% major surgery |
| Sensorineural hearing loss | From inner ear violation; uncommon in Tympanicus |
| Conductive hearing loss | From ossicular disruption |
| CSF leak | Tegmen or dural violation |
| Tumour recurrence | 5–10% long-term; surveillance MRI required |
| Lower cranial nerve palsies | Dysphagia (CN X), shoulder weakness (CN XI) — Glomus Jugulare |
| Hypertensive crisis | Functional paraganglioma — inadequate preoperative alpha-blockade |
PROGNOSIS
| Tumour Type | 5-year Control Rate |
|---|
| Glomus Tympanicus (Fisch A) | >95% cure with surgery |
| Glomus Jugulare (Fisch B/C) | 85–90% control |
| Fisch D (intracranial) | 60–75% control |
| Malignant paraganglioma | Poor; chemotherapy (temozolomide/sunitinib) experimental |
RECENT ADVANCES (Important for RGUHS)
1. Genetics and Hereditary Paraganglioma Syndromes
- SDH gene mutations (SDHB, SDHC, SDHD) identified in 25–35% of cases
- SDHB mutations associated with malignancy (sympathetic paraganglioma)
- Genetic counselling + testing of first-degree relatives now recommended (Cummings 7th ed.; Baysal et al., NEJM 2000)
2. 68-Ga DOTATATE PET-CT
- Gold standard for imaging paragangliomas (sensitivity >95%)
- Identifies multicentric disease (up to 40% in hereditary)
- Replaces Octreotide scintigraphy (Timmers et al., JCEM 2012)
3. Stereotactic Radiosurgery (SRS) / Gamma Knife
- Local control 92–97% at 5 years for Glomus Tympanicus/Jugulare
- Cranial nerve preservation significantly better than open surgery for C/D
- Increasingly preferred as primary treatment for Fisch C/D (Cummings 7th ed.; Liscak et al., 2016)
4. Endoscopic Ear Surgery (EES) for Glomus Tympanicus
- Fully endoscopic transcanal approach (4 mm, 0° and 30° rigid endoscopes)
- Advantages: Superior visualisation of hypotympanum, no external incision
- Growing evidence for Glasscock-Jackson Type I–III (Marchioni et al., Otolaryngol Head Neck Surg, 2017)
5. PRRT (Peptide Receptor Radionuclide Therapy)
- 177Lu-DOTATATE for malignant/metastatic paraganglioma
- Targets somatostatin receptor subtype 2 (SSTR2)
- Approved for neuroendocrine tumours; trials ongoing for head and neck paragangliomas (Strosberg et al., NEJM 2017)
6. Targeted Systemic Therapy
- Sunitinib, Cabozantinib (VEGFR inhibitors) — phase II trials
- For metastatic SDHB-mutated paragangliomas
- Temozolomide-based chemotherapy for rapidly progressive disease
7. Intraoperative Neuromonitoring
- Continuous facial nerve EMG monitoring now standard for all skull base surgery
- Reduces permanent facial palsy rates significantly
SUMMARY TABLE: GLOMUS TYMPANICUS vs GLOMUS JUGULARE
| Feature | Glomus Tympanicus | Glomus Jugulare |
|---|
| Origin | Jacobson's nerve (CN IX) on promontory | Jugular fossa adventitia (CN X) |
| Fisch Class | Type A | Type B/C/D |
| Location | Middle ear | Jugular fossa → temporal bone |
| Main symptom | Pulsatile tinnitus + CHL | Pulsatile tinnitus + CN IX–XII palsies |
| Otoscopy | Red mass on promontory | Large mass filling middle ear + EAC |
| Brown's sign | Present | Present |
| Bone erosion on CT | Absent / minimal | Moth-eaten jugular fossa + petrous |
| MRI | Focal enhancing mass on promontory | "Salt-and-pepper"; jugular fossa mass |
| Surgery | Transcanal tympanotomy | Infratemporal fossa (Fisch Type A) |
| Prognosis | Excellent (>95% cure) | Good (85–90% control) |
| CN palsies | Rare | Common (Vernet's syndrome) |
KEY EXAMINATION POINTS FOR RGUHS
- Brown's sign is pathognomonic of glomus tumour of the middle ear
- Never biopsy a pulsatile reddish middle ear mass without prior imaging (HRCT + MRI)
- Aberrant ICA must be excluded before any middle ear procedure
- Fisch classification is the most used globally; Glasscock-Jackson for tympanicus specifically
- Pre-operative alpha-blockade (Phenoxybenzamine) is mandatory for functional paragangliomas
- Pre-operative embolisation 24–72 hrs before surgery reduces blood loss
- Treatment of choice for Glomus Tympanicus is transcanal surgical excision
- Stereotactic radiosurgery is preferred for elderly/unfit and Fisch C/D
- SDH gene mutations — hereditary; genetic counselling recommended
- 68-Ga DOTATATE PET-CT is the modern gold standard for staging/multicentricity
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, 8th ed. — Gleeson et al. — Chapter on Paragangliomas of the temporal bone
- Cummings Otolaryngology Head and Neck Surgery, 7th ed. — Flint et al. — Chapter 120: Paragangliomas of the Head and Neck
- Stell & Maran's Head and Neck Surgery, 5th ed. — Watkinson & Gilbert — Temporal bone tumours
- Diseases of Ear, Nose and Throat, 7th ed. — P.L. Dhingra — Chapter on Tumours of the Ear
- Textbook of ENT and Head & Neck Surgery, 4th ed. — Hazarika et al. — Glomus tumours
- ENT — Zakir Hussain — Practical ENT examination guide
- Baysal et al. (2000) — Mutations in SDHD, a mitochondrial complex II gene, in hereditary paraganglioma — Science, 287:848
- Timmers et al. (2012) — Comparison of 18F-DOPA, 18F-FDG, and 18F-FDA PET/CT — J Clin Endocrinol Metab
- Marchioni et al. (2017) — Endoscopic management of glomus tympanicum — Otolaryngol Head Neck Surg
- Liscak et al. (2016) — Gamma knife radiosurgery of glomus jugulare tumours — Stereotact Funct Neurosurg
This answer covers etiology, clinical features, investigations with flowcharts, full surgical and non-surgical management, classification systems, differential diagnosis, complications, prognosis, and recent advances appropriate for a 50-mark RGUHS long essay question in ENT.