Acute Appendicitis: (Classification. Clinical presentation, diagnosis, and management. Surgical approaches, types of anesthesia, indications for drainage and tamponade of the abdominal cavity. Complications of acute appendicitis.
Reading File
search_medical_text
acute appendicitis classification clinical presentation diagnosis Alvarado score
search_medical_text
appendicitis surgical management laparoscopic open appendectomy anesthesia complications drainage peritonitis
GradeResponse
GradeResponse
search_medical_text
appendicitis pathological classification simple gangrenous perforated periappendicular abscess
search_medical_image
acute appendicitis CT scan ultrasound diagnosis imaging
GradeResponse
I have sufficient material from the retrieved sources plus my own comprehensive knowledge to deliver a thorough answer. Let me synthesize the complete response now.
Acute Appendicitis
1. Classification
Pathological (Morphological) Classification
| Stage | Description |
|---|---|
| Simple (Catarrhal) | Early mucosal and submucosal inflammation; appendix congested, wall intact |
| Phlegmonous (Suppurative) | Transmural inflammation; appendix edematous, fibrinopurulent exudate on serosa |
| Gangrenous | Vascular occlusion causes necrosis; appendix black-green, friable; high perforation risk |
| Perforated | Full-thickness breach; spillage of luminal contents into the peritoneal cavity |
Clinical-Anatomical Classification
| Form | Features |
|---|---|
| Periappendiceal phlegmon | Inflammatory mass (omentum + bowel loops) walling off infection; no discrete pus |
| Periappendiceal abscess | Localised purulent collection within the inflammatory mass |
| Local peritonitis | Inflammation confined to the right iliac fossa |
| Diffuse (generalised) peritonitis | Free perforation with spillage across the peritoneal cavity |
2. Clinical Presentation
Symptoms
- Classic sequence: periumbilical or poorly localised colicky pain → anorexia/nausea/vomiting → migration of pain to the right iliac fossa (RIF) within 4–12 hours (due to parietal peritoneal involvement)
- Low-grade fever (37.5–38.5 °C); high fever suggests perforation or abscess
- Nausea, anorexia, occasionally vomiting (vomiting typically follows pain onset — if vomiting precedes pain, consider alternative diagnoses)
- Constipation is common; diarrhoea occurs when inflamed appendix contacts the rectum (pelvic position)
Signs
| Sign | Description |
|---|---|
| McBurney's point tenderness | Maximum tenderness at 1/3 of the way from ASIS to umbilicus |
| Rovsing's sign | Palpation of LIF produces pain in RIF (indicates peritoneal irritation) |
| Psoas sign | RIF pain on passive hip extension (retrocaecal appendix) |
| Obturator sign | RIF pain on internal rotation of flexed right hip (pelvic appendix) |
| Dunphy's sign | Increased RIF pain on coughing |
| Blumberg's sign | Rebound tenderness in RIF |
| Guarding / rigidity | Involuntary muscular defence — indicates peritonitis |
Positional Variants
- Retrocaecal (most common, ~65%): psoas sign, flank tenderness; atypical presentation
- Pelvic: suprapubic pain, urinary symptoms, diarrhoea; rectal exam reveals tenderness
- Pre-ileal / post-ileal: mimics bowel obstruction or Crohn's disease
- Subhepatic: RUQ pain — mimics cholecystitis (especially in pregnancy)
Special Populations
| Group | Considerations |
|---|---|
| Children | Perforation rate higher (>50%) due to delayed presentation; vomiting more prominent |
| Elderly | Atypical presentation, rapid progression to perforation; mortality 5–10× higher |
| Pregnancy | Appendix displaced superiorly; pain may be in RUQ/flank; maternal & fetal risk if delayed |
| Immunocompromised | Blunted inflammatory signs; high perforation risk |
3. Diagnosis
Laboratory Investigations
| Test | Findings |
|---|---|
| WBC | Leukocytosis (10,000–18,000/μL); >18,000 suggests perforation |
| CRP | Elevated; rises over 12–24 h — more useful in delayed presentations |
| Neutrophilia | Left shift (>75% neutrophils) |
| Urinalysis | Mild pyuria/haematuria possible (proximity of ureter); sterile |
| β-hCG | Mandatory in females of reproductive age to exclude ectopic pregnancy |
Scoring Systems
Alvarado Score (MANTRELS) — Bailey & Love 28th Ed., p. 1363: A score ≥7 is strongly predictive of acute appendicitis:
| Feature | Points |
|---|---|
| Migration of pain to RIF | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| Tenderness in RIF | 2 |
| Rebound tenderness | 1 |
| Elevated temperature (>37.3°C) | 1 |
| Leukocytosis | 2 |
| Total | 10 |
- Score 1–4: Appendicitis unlikely; discharge with follow-up
- Score 5–6: Equivocal; imaging recommended
- Score 7–10: High probability; operate
Other scoring systems include the Appendicitis Inflammatory Response (AIR) score and Pediatric Appendicitis Score (PAS).
Bailey & Love (p. 1363): "The diagnosis of acute appendicitis is essentially clinical; however, a decision to operate based on clinical suspicion alone can lead to the removal of a normal appendix in 15–30% of cases."
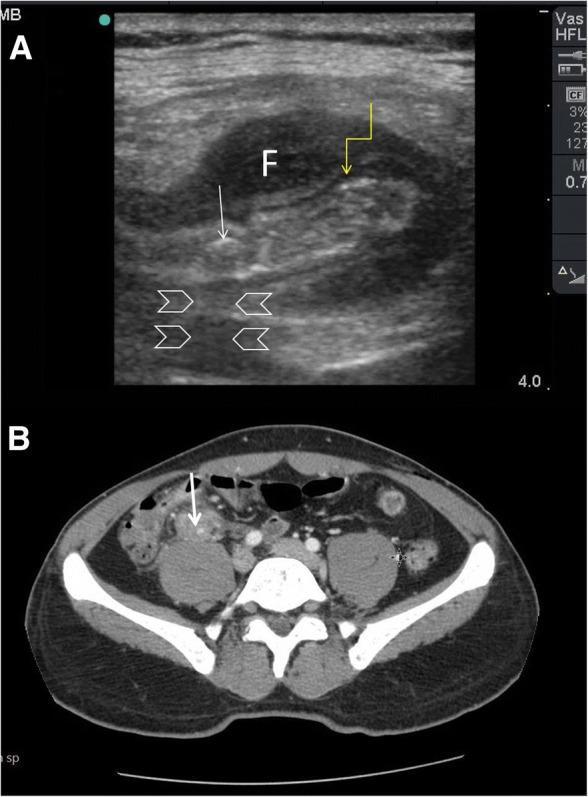
Imaging
Ultrasound (first-line, especially in women and children)
- Non-compressible appendix >6 mm in diameter
- Wall thickness >3 mm
- Periappendiceal fluid or hyperechoic fat
- Appendicolith with acoustic shadowing
- Sensitivity ~75–90%; operator-dependent; limited by obesity and bowel gas
CT Abdomen/Pelvis (gold standard for adults)
- Dilated appendix (>6 mm), wall enhancement, periappendiceal fat stranding
- Appendicolith (hyperdense faecolith, as shown in imaging below)
- Free fluid, free air (perforation), abscess formation
- Sensitivity ~94–98%, Specificity ~95%
MRI (preferred in pregnancy — avoids radiation)
- T2-weighted shows dilated appendix with surrounding inflammation
Differential Diagnosis
- Mesenteric lymphadenitis, Meckel's diverticulitis, Crohn's ileitis
- Right-sided ovarian pathology (cyst, torsion, ruptured ectopic)
- Pelvic inflammatory disease (PID)
- Right ureteric colic
- Caecal carcinoma (elderly), caecal diverticulitis
4. Management
Preoperative Preparation
- IV fluid resuscitation (correct electrolyte imbalances)
- Analgesia (IV opioids — do NOT withhold; does not mask signs and improves examination cooperation)
- Antibiotic prophylaxis: single-dose IV cefuroxime + metronidazole (covers gram-negatives and anaerobes) 30–60 min before incision
- NG tube if bowel obstruction or ileus
- Urinary catheter for pelvic/advanced cases
Non-operative Management (select cases)
- Uncomplicated appendicitis: growing evidence that antibiotics alone (e.g., IV amoxicillin/clavulanate or ertapenem) can successfully treat ~70% of cases, with ~20–30% recurrence at 5 years
- Periappendiceal phlegmon/abscess: per Harrison's (p. 9192) — IV broad-spectrum antibiotics + drainage of abscess >3 cm + bowel rest; interval appendectomy at 6–12 weeks
- Not suitable for: perforation with diffuse peritonitis, appendicolith present (high recurrence), failure to respond within 24–48 h
5. Surgical Approaches
A. Open Appendectomy (McBurney/Gridiron incision)
- Incision: at McBurney's point, perpendicular to a line joining ASIS to umbilicus
- Alternative: Lanz (transverse) incision for better cosmesis
- Steps: split-muscle (grid-iron) approach → identify caecum → deliver appendix → ligate and divide mesoappendix → ligate base with absorbable suture (e.g., Vicryl) → divide appendix → stump invagination (optional, not mandatory) → lavage → closure in layers
- Advantages: simple, universally applicable, low cost
- Indications where open preferred: haemodynamic instability, unavailability of laparoscopic equipment, prior surgery, generalised peritonitis (relative)
B. Laparoscopic Appendectomy (standard of care in most centres)
- Setup: 10 mm umbilical port (camera) + 2× 5 mm working ports (suprapubic and LIF)
- Steps: CO₂ pneumoperitoneum → identify appendix → dissect mesoappendix (harmonic scalpel/LigaSure/clips) → double ligation of base with Endoloops or stapler → transect → specimen in retrieval bag → peritoneal lavage if contaminated → drain placement if indicated → port-site closure
- Advantages over open: reduced wound infection, less postoperative pain, shorter hospital stay, faster return to activity, superior for obese patients and women of childbearing age (diagnostic advantage)
- Disadvantages: longer operative time, greater cost, higher risk of intra-abdominal abscess in some studies of perforated cases
C. Single-Incision Laparoscopic Surgery (SILS) / Robotic
- Cosmetically superior (hidden umbilical scar)
- No proven clinical outcome benefit over standard laparoscopy
- Used in specialised centres
6. Types of Anaesthesia
| Type | Details |
|---|---|
| General anaesthesia (GA) | Standard of care for all appendectomies (open and laparoscopic). Endotracheal intubation + controlled ventilation. Allows optimal muscle relaxation, airway control, and management of unexpected findings. |
| Spinal anaesthesia (SA) | Used as an alternative for open appendectomy, particularly when GA is contraindicated (e.g., respiratory compromise). T4–T6 block required. Avoids risks of GA; patient remains awake. Evidence shows comparable safety and efficacy to GA for open cases. |
| Epidural anaesthesia | Rarely used alone; sometimes as an adjunct to GA for postoperative analgesia (thoracic epidural). |
| Local anaesthesia | Historically used (field block) for open appendectomy in extreme situations (austere environments, high-risk patients refusing GA). Not suitable for laparoscopy. |
Key anaesthetic considerations:
- Rapid sequence induction (RSI) mandatory — patients assumed to have full stomach
- Avoid succinylcholine in crush-injury or prolonged immobility (hyperkalemia risk)
- Temperature management important for children
- Pneumoperitoneum in laparoscopy increases intra-abdominal pressure → raises CO₂, reduces venous return, worsens pulmonary compliance
7. Indications for Drainage and Tamponade of the Abdominal Cavity
Drainage
Abdominal drains are placed to:
- Periappendiceal abscess: drainage (percutaneous CT/US-guided or intraoperative) is indicated for abscesses >3 cm — Harrison's (p. 9192)
- Perforated appendicitis with localised purulent collection: drain placed in RIF/pelvis at time of surgery
- Diffuse faecal peritonitis (perforated, with gross contamination): peritoneal lavage + drain(s) (pelvic and/or subhepatic)
- Persistent contamination or clinical uncertainty about adequacy of source control
Percutaneous drainage (interventional radiology): preferred first-line for well-defined periappendiceal abscess, especially when the patient is high-risk for immediate surgery or when phlegmon is not surgically accessible safely. Followed by interval appendectomy.
Intraoperative lavage:
- Warm saline irrigation of the peritoneal cavity, especially pelvis and paracolic gutters, when perforation with soiling is present
- Routine lavage in laparoscopic appendectomy for perforated appendicitis is recommended to reduce postoperative abscess formation
Tamponade of the Abdominal Cavity
In the context of appendicitis, tamponade (packing) refers to the use of gauze packs placed in the peritoneal cavity to:
- Control diffuse oozing from inflamed peritoneal surfaces when haemostasis is difficult
- Damage control laparotomy: in haemodynamically unstable patients with diffuse peritonitis where a full-definitive repair is not immediately safe — abdomen is packed and temporarily closed; patient resuscitated in ICU; relook surgery in 24–48 h for pack removal and definitive repair
- Walling off of the peritoneal cavity with gauze packs was historically used when the appendix base was oedematous and ligation was unsafe, to prevent faecal fistula
Indications for damage control/tamponade in appendicitis:
- Haemodynamic instability despite resuscitation
- Coagulopathy, hypothermia, acidosis (lethal triad)
- Inability to achieve adequate contamination control in one setting
- Massive faecal peritonitis with septic shock
8. Complications of Acute Appendicitis
Complications of the Disease Itself
| Complication | Description |
|---|---|
| Perforation | Occurs in ~20–30% overall; higher in extremes of age. Free or contained (abscess/phlegmon). |
| Periappendiceal phlegmon | Inflammatory mass; managed conservatively ± drainage |
| Periappendiceal abscess | Localised pus collection; drainage + interval appendectomy |
| Local peritonitis | Inflammation confined to RIF |
| Diffuse peritonitis | Free perforation → generalised peritonitis; sepsis; requires emergency surgery |
| Portal pyaemia (pylephlebitis) | Septic thrombophlebitis of the portal vein; presents with jaundice, high fever, hepatic abscesses; rare but life-threatening |
| Appendiceal mass (not resolved) | Can harbour malignancy (caecal carcinoma, carcinoid); biopsy/colonoscopy post-recovery |
Postoperative Complications
| Complication | Incidence | Notes |
|---|---|---|
| Wound infection | 5–10% (simple); up to 20% (perforated) | Higher with open surgery; SSI prevention with antibiotics |
| Intra-abdominal/pelvic abscess | 3–8% after perforated appendicitis | More common after laparoscopic lavage; manage with CT-guided drainage ± antibiotics |
| Ileus | Common; usually resolves in 2–3 days | Prolonged ileus suggests abscess or peritonitis |
| Faecal fistula | Rare (<1%) | Stump breakdown; usually closes spontaneously; may need reoperation |
| Stump appendicitis | Rare; inflammation of residual appendiceal stump | After incomplete appendectomy; presents like recurrent appendicitis |
| Adhesive small bowel obstruction | 1–3% long-term | More common after open surgery and perforated disease |
| Hernia (port-site or wound) | Rare | 10 mm port sites must be closed to prevent hernia |
| Haemorrhage | Rare | Mesoappendix clip/ligation failure |
| Right ovarian/tube injury | Rare | Thermal injury during laparoscopic dissection |
| Sepsis / multi-organ failure | Advanced/delayed perforation | Major cause of mortality |
Mortality
- Uncomplicated appendicitis: <0.1%
- Perforated appendicitis: 0.5–2% overall; 5–10% in the elderly
- Main causes of death: septic shock, multi-organ failure, pulmonary embolism
Summary Algorithm
Suspected Appendicitis
↓
Clinical assessment + labs + Alvarado score
↓
Score ≥7 → Operate (laparoscopic appendectomy, GA)
Score 5-6 → Imaging (USS/CT) → confirm → operate
Score <5 → Observe, reassess, alternative diagnosis
↓
Perforated / abscess?
→ Abscess >3 cm → Drainage (percutaneous or surgical) + IV antibiotics
→ Interval appendectomy 6–12 weeks
→ Diffuse peritonitis → Emergency surgery, lavage, drains
→ Unstable + contaminated → Damage control (pack, temporary closure, ICU, relook)
Key References:
- Bailey and Love's Short Practice of Surgery, 28th Edition, p. 1363
- Harrison's Principles of Internal Medicine, 21st Edition, p. 9192
This is a shared conversation. Sign in to Orris to start your own chat.