Malformations of Musculoskeletal System in Children
musculoskeletal malformations congenital children types classification
congenital musculoskeletal malformations children skeletal deformities
Musculoskeletal Malformations in Children
Classification by Aetiology
| Category | Mechanism | Examples |
|---|---|---|
| Malformations | Primary structural defect during organogenesis | Clubfoot, polydactyly, limb aplasia |
| Deformations | Mechanical forces on normal tissue | Positional talipes, hip dysplasia |
| Disruptions | Breakdown of normally formed structures | Amniotic band syndrome |
| Dysplasias | Abnormal tissue organisation/growth | Osteogenesis imperfecta, achondroplasia |
Major Categories of Musculoskeletal Malformations
1. Limb Malformations
Upper Limb
- Polydactyly – supernumerary digits (pre-axial or post-axial)
- Syndactyly – fusion of digits (cutaneous or osseous)
- Brachydactyly – shortened digits
- Ectrodactyly (split hand) – absence of central digits
- Radial/ulnar clubhand – longitudinal deficiency of the radius or ulna
- Amelia – complete absence of a limb
- Phocomelia – intercalary limb deficiency (hand attached near shoulder); associated with thalidomide exposure
- Sprengel's deformity – congenitally elevated and hypoplastic scapula
Lower Limb
- Congenital Talipes Equinovarus (CTEV / Clubfoot) – foot held in equinus, varus, adduction, and cavus; incidence ~1–2 per 1,000 live births; treated by Ponseti method
- Congenital Vertical Talus (Rocker-bottom foot) – rigid flatfoot
- Metatarsus adductus – forefoot adduction, often self-correcting
- Proximal Focal Femoral Deficiency (PFFD) – partial absence/underdevelopment of the femur
- Tibial/fibular hemimelia – absence or hypoplasia of tibia or fibula
2. Spine Malformations
| Condition | Description |
|---|---|
| Spina bifida occulta | Posterior arch defect without neural involvement |
| Meningocele | Meninges herniate through vertebral defect |
| Myelomeningocele | Spinal cord + meninges herniate; causes neurological deficit |
| Scoliosis (congenital) | Due to hemivertebra, block vertebra, or rib fusion |
| Klippel-Feil syndrome | Fusion of cervical vertebrae; short neck, limited motion |
| Torticollis (congenital muscular) | Sternocleidomastoid fibrosis causing head tilt |
3. Hip Malformations
- Developmental Dysplasia of the Hip (DDH)
- Spectrum from mild acetabular dysplasia to frank dislocation
- Risk factors: female sex, breech presentation, positive family history, oligohydramnios
- Screening: Barlow & Ortolani tests in neonates; ultrasound in infants <6 months; X-ray >4–6 months
- Treatment: Pavlik harness (< 6 months), closed/open reduction, pelvic osteotomy
4. Skeletal Dysplasias (Osteochondrodysplasias)
| Condition | Gene/Mechanism | Features |
|---|---|---|
| Achondroplasia | FGFR3 gain-of-function | Rhizomelic short stature, macrocephaly, trident hands |
| Osteogenesis Imperfecta | COL1A1/COL1A2 mutations | Brittle bones, blue sclerae, recurrent fractures |
| Multiple Hereditary Exostoses | EXT1/EXT2 | Multiple osteochondromas; risk of sarcomatous change |
| Diastrophic Dysplasia | SLC26A2 (sulfate transporter) | Severe short stature, clubfoot, hitchhiker thumb |
| Thanatophoric Dysplasia | FGFR3 | Lethal; severe micromelia, cloverleaf skull |
5. Joint and Soft Tissue Malformations
- Congenital Dislocation of the Knee – hyperextension deformity at birth
- Arthrogryposis Multiplex Congenita – multiple joint contractures from reduced fetal movement; causes include neurological, muscular, or connective tissue disorders
- Larsen Syndrome – multiple joint dislocations + flat facies due to filamin B mutation
- Ehlers-Danlos Syndrome – joint hypermobility + skin/connective tissue fragility
6. Complex/Severe Malformations

Aetiology & Risk Factors
| Factor | Examples |
|---|---|
| Genetic | Single-gene mutations, chromosomal anomalies (trisomy 18, 21) |
| Teratogenic | Thalidomide (phocomelia), valproate (neural tube defects), alcohol |
| Mechanical | Oligohydramnios, amniotic bands, uterine constraint |
| Vascular | Interruptions causing limb reduction defects |
| Multifactorial | CTEV, DDH |
| Unknown | ~50% of isolated malformations |
Diagnostic Approach
-
Prenatal
- Routine anomaly ultrasound at 18–20 weeks (detects major limb/spine defects)
- Fetal MRI for complex cases
- Amniocentesis/CVS for chromosomal/genetic diagnosis
-
Postnatal
- Thorough physical exam at birth
- Radiographs (skeletal survey for dysplasias)
- Ultrasound (DDH screening)
- MRI (spinal cord involvement, soft tissues)
- Genetic karyotyping / molecular panels
Management Principles
| Approach | Used For |
|---|---|
| Conservative (casting/bracing) | Clubfoot (Ponseti), DDH (Pavlik harness), metatarsus adductus |
| Surgical correction | Osteotomies, tendon transfers, arthrodesis, amputation/prosthetics |
| Orthotics/prosthetics | Limb deficiencies, post-surgical support |
| Multidisciplinary team | Orthopaedics, physio, OT, genetics, neurosurgery |
| Gene/bisphosphonate therapy | Osteogenesis imperfecta (pamidronate/zoledronic acid) |
Prognosis
- Many minor malformations (e.g., polydactyly, syndactyly, positional talipes) respond well to early treatment with excellent functional outcomes.
- DDH diagnosed and treated before 6 months has near-normal outcomes; delayed treatment risks avascular necrosis and early arthritis.
- Skeletal dysplasias are lifelong conditions but compatible with a productive life in most forms (except lethal dysplasias).
- Complex multi-system malformations (LBWC, arthrogryposis) require intensive multidisciplinary care.
Name of surgery and conditions
surgical procedures names congenital musculoskeletal malformations children operations
orthopedic surgery techniques clubfoot DDH scoliosis pediatric
Surgical Procedures in Pediatric Musculoskeletal Malformations
Foot & Ankle
| Surgery | Condition |
|---|---|
| Ponseti Method (serial casting + percutaneous Achilles tenotomy) | Congenital Talipes Equinovarus (Clubfoot) |
| Posteromedial Release (PMR) | Resistant/recurrent clubfoot |
| Tibialis Anterior Tendon Transfer (TATT) | Dynamic supination relapse in clubfoot |
| Cincinnati incision / soft tissue release | Severe clubfoot |
| Dorsal closing wedge osteotomy | Congenital vertical talus (rocker-bottom foot) |
| Reverse Ponseti (casting) + surgical release | Congenital vertical talus |
| Metatarsal osteotomy | Persistent metatarsus adductus |
Hip
| Surgery | Condition |
|---|---|
| Closed Reduction + Spica Cast | Developmental Dysplasia of the Hip (DDH) — early |
| Open Reduction (medial or anterior approach) | DDH — failed closed reduction |
| Salter Innominate Osteotomy | DDH — acetabular dysplasia (age 18 months–6 years) |
| Pemberton Osteotomy | DDH — incomplete triradiate cartilage closure |
| Dega Osteotomy | DDH with neuromuscular involvement (e.g., cerebral palsy) |
| Femoral Varus Derotation Osteotomy (VDRO) | DDH — excessive femoral anteversion |
| Triple Pelvic Osteotomy (Steel/Tönnis) | Older children/adolescents with residual DDH |
| Periacetabular Osteotomy (PAO / Ganz) | Adolescents/young adults with acetabular dysplasia |
Spine
| Surgery | Condition |
|---|---|
| Posterior Spinal Fusion (PSF) | Congenital/idiopathic scoliosis |
| Anterior Spinal Fusion (ASF) | Thoracolumbar scoliosis |
| Hemivertebra Excision | Congenital scoliosis due to hemivertebra |
| Growing Rods (single/dual) | Early-onset scoliosis in young children |
| VEPTR (Vertical Expandable Prosthetic Titanium Rib) | Thoracic insufficiency syndrome + scoliosis |
| MAGEC Rods (magnetically controlled growing rods) | Early-onset scoliosis |
| Posterior Cervical Fusion | Klippel-Feil syndrome with instability |
| Laminectomy / Spinal Cord Detethering | Tethered cord, myelomeningocele |
| Meningocele / Myelomeningocele Repair | Spina bifida |
Limb Deficiencies & Digits
| Surgery | Condition |
|---|---|
| Pollicisation (index finger converted to thumb) | Thumb aplasia / hypoplasia (radial clubhand) |
| Centralisation / Radialisation | Radial clubhand |
| Syndactyly Release (with/without skin grafting) | Syndactyly |
| Polydactyly Excision | Polydactyly |
| Web Deepening / Z-plasty | Congenital constriction band syndrome |
| Syme Amputation | Fibular hemimelia — unsalvageable limb |
| Van Nes Rotationplasty | Proximal Focal Femoral Deficiency (PFFD) |
| Limb Lengthening (Ilizarov / PRECICE nail) | Leg length discrepancy, fibular/tibial hemimelia |
Knee
| Surgery | Condition |
|---|---|
| Quadriceps lengthening + posterior capsulotomy | Congenital dislocation of the knee |
| Soft tissue release + osteotomy | Arthrogryposis multiplex congenita — knee contracture |
Scapula & Shoulder
| Surgery | Condition |
|---|---|
| Woodward Procedure (scapular repositioning) | Sprengel's deformity |
| Green Procedure | Sprengel's deformity — alternative approach |
| Omovertebral Bar Excision | Sprengel's deformity — bony bar removal |
Neck
| Surgery | Condition |
|---|---|
| Sternocleidomastoid Release / Myotomy | Congenital muscular torticollis — refractory cases |
Skeletal Dysplasias
| Surgery | Condition |
|---|---|
| Foramen Magnum Decompression | Achondroplasia — cervicomedullary compression |
| Limb Lengthening (bilateral) | Achondroplasia — stature correction |
| Intramedullary Rodding (Fassier-Duval / Rush rods) | Osteogenesis imperfecta — recurrent fractures |
| Spinal Fusion | Osteogenesis imperfecta / skeletal dysplasia with instability |
| Osteochondroma Excision | Multiple Hereditary Exostoses |
Key Principle
The timing of surgery is critical. Most conditions are best corrected in early childhood when bone is malleable, remodelling capacity is high, and neurological plasticity is greatest. Delayed intervention (e.g., DDH diagnosed after age 2) leads to more complex surgery and worse outcomes.
Hernias: hernias of the anterior abdominal wall, inguinal hernias-D
hernias anterior abdominal wall types classification umbilical epigastric incisional
inguinal hernia anatomy types direct indirect diagnosis management surgery
inguinal hernia direct indirect difference Hesselbach triangle deep ring anatomy
ventral hernia umbilical paraumbilical epigastric Spigelian lumbar hernia features treatment
Hernias of the Anterior Abdominal Wall
Definition
- Sac – peritoneal covering
- Neck – constriction at the defect
- Body/fundus – the sac proper
- Contents – omentum, bowel (small/large), bladder, ovary, etc.
Ventral (Anterior Abdominal Wall) Hernias
European Hernia Society (EHS) Classification (2009)
| Category | Types |
|---|---|
| Primary Ventral Hernias | Epigastric, Umbilical, Paraumbilical, Spigelian |
| Incisional Hernias | Through a previous surgical scar |
| Parastomal Hernias | Adjacent to a stoma site |
Types of Anterior Abdominal Wall Hernias
1. Umbilical Hernia
- In children: Due to failure of the umbilical ring to close after birth; common in premature and Afro-Caribbean infants
- Most close spontaneously by age 3–4 years
- Surgery indicated if persists beyond age 4, symptomatic, or ring > 1.5 cm
- In adults: Acquired; associated with obesity, ascites, multiple pregnancies, raised intra-abdominal pressure
- Risk of strangulation is higher in adults → early repair recommended
- Repair: Mayo's "vest-over-pants" technique (overlap repair) or mesh repair
2. Paraumbilical Hernia
- Protrudes just above or below the umbilicus through the linea alba
- Almost exclusively in adults; more common in obese, multiparous women
- Higher risk of strangulation than true umbilical hernia
- Contents: omentum, transverse colon, small bowel
- Repair: Mayo's repair or mesh (mesh preferred for defects > 3 cm)
3. Epigastric Hernia
- Through defects in the linea alba between xiphoid and umbilicus
- Often contains extraperitoneal fat (not a true peritoneal sac initially)
- Small but can be painful; may be multiple
- More common in males
- Repair: Simple fascial closure; mesh for larger defects
4. Incisional Hernia
- Occurs through a previous surgical scar (any site)
- Incidence: 10–15% after midline laparotomy
- Risk factors: wound infection, obesity, malnutrition, steroid use, poor surgical technique
- May contain large amounts of bowel ("loss of domain")
- Repair: Open (Rives-Stoppa retromuscular mesh) or laparoscopic (IPOM – Intraperitoneal Onlay Mesh)
5. Spigelian Hernia
- Through the Spigelian fascia (lateral edge of rectus abdominis, at the level of the arcuate line)
- Interparietal – lies between layers of abdominal wall; therefore often not visible
- Difficult to diagnose clinically → CT/ultrasound essential
- High risk of strangulation
- Repair: Open or laparoscopic mesh repair
6. Lumbar Hernia
- Through the superior lumbar triangle (Grynfeltt) or inferior lumbar triangle (Petit)
- Rare; may be congenital or acquired (post-trauma, post-surgery)
- Repair: Mesh repair (open or laparoscopic)
7. Parastomal Hernia
- Adjacent to a colostomy or ileostomy site
- Very common (up to 50% of stomas)
- Management: relocation of stoma or mesh repair (Sugarbaker or keyhole technique)
Summary Table — Anterior Abdominal Wall Hernias
| Hernia | Site | Common in | Key Feature | Repair |
|---|---|---|---|---|
| Umbilical (child) | Umbilical ring | Infants | Often self-resolving | Conservative → surgery if persists |
| Umbilical (adult) | Umbilical ring | Obese adults | Risk of strangulation | Mayo / mesh |
| Paraumbilical | Just above/below umbilicus | Obese women | High strangulation risk | Mayo / mesh |
| Epigastric | Linea alba, epigastrium | Males | Contains fat, painful | Fascial closure / mesh |
| Incisional | Previous scar | Post-op patients | Large, complex | Rives-Stoppa / IPOM |
| Spigelian | Lateral rectus edge | Middle-aged | Interparietal, occult | CT → mesh repair |
| Lumbar | Lumbar triangles | Adults | Rare, dorsolateral | Mesh |
| Parastomal | Around stoma | Stoma patients | Very common | Stoma relocation / mesh |
Inguinal Hernias
Definition
Anatomy of the Inguinal Canal
| Feature | Details |
|---|---|
| Length | ~4 cm in adults |
| Direction | Downward, medially, and forward |
| Deep (internal) ring | Defect in transversalis fascia, lateral to inferior epigastric vessels |
| Superficial (external) ring | Defect in external oblique aponeurosis, above pubic tubercle |
| Anterior wall | External oblique aponeurosis (+ internal oblique laterally) |
| Posterior wall | Transversalis fascia (+ conjoint tendon medially) |
| Roof | Internal oblique + transversus abdominis (arching fibres) |
| Floor | Inguinal ligament (Poupart's) |
| Contents (male) | Spermatic cord, ilioinguinal nerve, genital branch of genitofemoral nerve |
| Contents (female) | Round ligament of uterus, ilioinguinal nerve |
- Medial border: Lateral edge of rectus abdominis
- Lateral border: Inferior epigastric vessels
- Inferior border: Inguinal ligament
Types of Inguinal Hernia
| Feature | Indirect (Lateral/Oblique) | Direct (Medial) |
|---|---|---|
| Origin | Through deep inguinal ring (lateral to inferior epigastric vessels) | Through Hesselbach's triangle (medial to inferior epigastric vessels) |
| Cause | Congenital (patent processus vaginalis) or acquired | Acquired — weakness of posterior wall |
| Age | All ages; most common in children and young adults | Older adults (> 40 years) |
| Sex | M >> F | Males predominantly |
| Sac | Has a true peritoneal sac | May lack a true sac |
| Relationship to epigastric vessels | Lateral | Medial |
| Scrotal descent | Common | Uncommon |
| Strangulation risk | Higher (narrow neck) | Lower (wide neck) |
| Bilateral | Less common | More commonly bilateral |
| Zieman's test | Middle finger (ring at deep ring) feels impulse | Index finger (over Hesselbach's) feels impulse |
Aetiology & Risk Factors
- Congenital: Patent processus vaginalis (indirect)
- Raised intra-abdominal pressure: Chronic cough (COPD), constipation, BPH, ascites, heavy lifting
- Weakness of abdominal wall: Age, obesity, malnutrition, previous surgery
- Male sex: Inguinal canal wider, processus vaginalis present longer
- Prematurity: Incomplete obliteration of processus vaginalis
Clinical Features
- Reducible hernia: Swelling in groin/scrotum; appears on standing/straining; reduces on lying down
- Irreducible hernia: Cannot be pushed back — may be due to omental adhesions or loop of bowel
- Obstructed hernia: Bowel within sac is obstructed but NOT yet ischemic
- Strangulated hernia: Blood supply cut off → ischemia, gangrene → surgical emergency
- Signs: Severe pain, tender, tense, irreducible; systemic sepsis in late presentation
Diagnosis
- Primarily clinical — history + physical examination
- Patient examined standing and asked to cough
- Distinguish from: femoral hernia, lymphadenopathy, hydrocele, varicocele, undescended testis, lipoma of cord
| Investigation | Indication |
|---|---|
| Ultrasound | Occult hernia, unclear diagnosis |
| CT scan | Complex cases, recurrent hernia, pre-op planning |
| Herniography | Rarely used today |
| MRI | Sportsman's hernia / groin pain |
Management
Conservative
- Watchful waiting: Acceptable for asymptomatic or minimally symptomatic hernias in fit patients
- Truss: Only palliative; not curative; used in unfit patients
Surgical (Definitive Treatment)
Open Repairs
| Procedure | Description |
|---|---|
| Lichtenstein Tension-Free Mesh Repair | Gold standard for adults; polypropylene mesh placed in inguinal canal; low recurrence (< 1%) |
| Bassini Repair | Tension repair — conjoint tendon sutured to inguinal ligament; largely historical |
| Shouldice Repair | 4-layer continuous suture of posterior wall; excellent results in specialist centres |
| Herniotomy | Sac ligation only — standard in children (no mesh needed) |
| Herniorraphy | Repair of posterior wall without mesh |
| Hernioplasty | Repair with mesh reinforcement |
Laparoscopic / Minimally Invasive Repairs
| Procedure | Description |
|---|---|
| TEP (Totally Extraperitoneal) | Mesh placed in pre-peritoneal space without entering peritoneum; preferred laparoscopic technique |
| TAPP (Transabdominal Preperitoneal) | Transperitoneal access; mesh placed behind inguinal floor; peritoneum closed over mesh |
| RARP (Robot-Assisted) | Robotic version of TAPP; emerging technique |
Complications of Inguinal Hernia Surgery
| Complication | Notes |
|---|---|
| Haematoma / seroma | Most common early complication |
| Wound infection | ~1–2% with mesh |
| Chronic groin pain | Most significant long-term issue (~10–12%); due to nerve injury (ilioinguinal, iliohypogastric, genitofemoral) |
| Recurrence | < 1% with Lichtenstein; higher with tissue repairs |
| Vas deferens injury | Rare; can cause infertility |
| Testicular atrophy | Due to damage to testicular artery |
| Mesh complications | Infection, migration, shrinkage, fistula |
Special Situations
| Situation | Management |
|---|---|
| Children | Herniotomy (sac ligation); no mesh; day-case surgery |
| Bilateral hernia | Laparoscopic (TEP/TAPP) preferred — both sides repaired in one procedure |
| Recurrent hernia | Laparoscopic approach preferred to avoid scarred tissue plane |
| Strangulated hernia | Emergency surgery; bowel resection if necrotic; mesh use controversial |
| Incarcerated hernia | Gentle taxis attempt → if fails, emergency surgery |
Key Distinctions to Remember
| Indirect | Direct | |
|---|---|---|
| Relationship to inferior epigastric vessels | Lateral | Medial |
| Exits via | Deep inguinal ring | Posterior wall weakness |
| Covered by internal spermatic fascia | Yes | No |
| Strangulation risk | Higher | Lower |
| More common in | Young; congenital | Elderly; acquired |
Bottom line (Bailey & Love, p. 1086): Inguinal hernias are classified as indirect (lateral/oblique) or direct (medial), may be congenital or acquired, are diagnosed clinically (radiologically in special cases), and are repaired by open or minimally invasive (laparoscopic/robotic) surgery.
Symptoms treatment with method names surgery names
inguinal hernia symptoms clinical presentation reducible irreducible strangulated obstructed
inguinal hernia anterior abdominal wall hernia clinical presentation surgery repair
Symptoms of Hernias
General Symptoms (All Hernias)
| Symptom | Details |
|---|---|
| Swelling / lump | Appears on standing, straining, coughing; disappears on lying down (if reducible) |
| Dragging / aching pain | Due to tension on peritoneum and surrounding structures |
| Cough impulse | Characteristic — swelling expands on coughing |
| Discomfort on exertion | Worsens with heavy lifting, straining |
| Gurgling sensation | If bowel is in the sac |
Symptoms by Hernia State
| State | Symptoms | Key Features |
|---|---|---|
| Reducible | Soft lump, mild ache, reduces spontaneously or manually | Non-tender; no systemic upset |
| Irreducible | Persistent lump that cannot be pushed back | Discomfort; no ischaemia yet |
| Obstructed | Colicky abdominal pain, vomiting, constipation, abdominal distension | Bowel trapped, obstructed but not yet ischaemic |
| Incarcerated | Irreducible + signs of developing strangulation | Increasing pain, tenderness |
| Strangulated | Severe constant pain, tender, tense, non-reducible lump; nausea/vomiting; fever; signs of peritonitis/sepsis | Arterial supply cut off → ischaemia → gangrene → surgical emergency |
As Bailey & Love states: "If pressure rises sufficiently, arterial blood cannot enter the hernia and the contents become ischaemic and may infarct — the hernia is then said to have strangulated."
Site-Specific Symptoms
| Hernia Type | Specific Symptoms |
|---|---|
| Umbilical / Paraumbilical | Central abdominal lump at/near umbilicus; pain worse after meals if omentum/bowel involved |
| Epigastric | Small, tender lump in upper midline; pain often out of proportion to size (extraperitoneal fat trapped) |
| Inguinal (indirect) | Groin swelling extending into scrotum/labia; impulse on coughing; may mimic testicular swelling |
| Inguinal (direct) | Medial groin bulge; does not usually descend into scrotum; reduces easily |
| Incisional | Bulge along old scar; visible on straining; may cause bowel obstruction |
| Spigelian | Lateral abdominal wall pain without obvious external bulge (interparietal); easily missed |
| Parastomal | Bulge around stoma; difficulty fitting stoma appliance; obstruction risk |
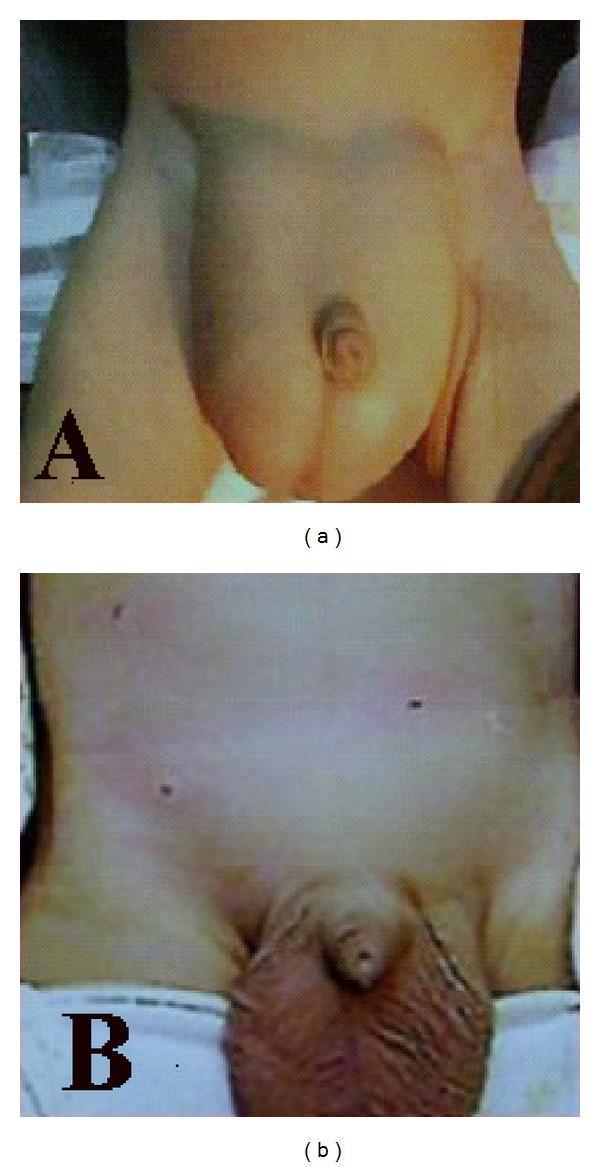
Clinical Image — Bilateral Inguinal Hernia (Pre and Post-op)
Surgical Treatments — Method Names & Surgery Names
A. Inguinal Hernia Surgeries
Open (Non-Laparoscopic) Methods
| Surgery Name | Method | Used For |
|---|---|---|
| Herniotomy | Sac is dissected, ligated at neck, and excised — no repair of posterior wall | Children (standard); no mesh needed |
| Herniorraphy | Sac ligation + repair of posterior wall with sutures (no mesh) | Simple repairs, low-resource settings |
| Hernioplasty | Sac ligation + reinforcement with mesh | Adults; standard modern practice |
| Lichtenstein Tension-Free Mesh Repair | Flat polypropylene mesh sutured to inguinal ligament and conjoint tendon, covering the posterior wall | Gold standard for adults; < 1% recurrence |
| Bassini Repair | Conjoint tendon sutured to inguinal ligament behind spermatic cord (tension repair) | Historical; largely abandoned |
| Shouldice Repair | 4-layer continuous suture repair of posterior wall using transversalis fascia | Best tension repair; used in specialist Shouldice centres |
| McVay (Cooper's Ligament) Repair | Conjoint tendon sutured to Cooper's ligament | Femoral + inguinal hernias; tension repair |
| Desarda Repair | Strip of external oblique aponeurosis used to reinforce posterior wall (no mesh) | Mesh-free alternative |
Laparoscopic / Minimally Invasive Methods
| Surgery Name | Method | Advantages |
|---|---|---|
| TEP (Totally Extraperitoneal Repair) | Balloon dissection creates pre-peritoneal space; mesh placed behind inguinal floor without entering peritoneum | No peritoneal entry; faster recovery; preferred technique |
| TAPP (Transabdominal Preperitoneal Repair) | Peritoneal cavity entered; peritoneum incised; mesh placed in pre-peritoneal space; peritoneum closed over mesh | Better visualisation; useful in complex cases |
| IPOM (Intraperitoneal Onlay Mesh) | Mesh placed directly inside peritoneum | Less used for inguinal; more for ventral hernias |
| Robotic-Assisted Repair (RARP) | Robotic platform (e.g., Da Vinci) performing TAPP or TEP | Precise dissection; used in complex/bilateral/recurrent cases |
B. Anterior Abdominal Wall Hernia Surgeries
Umbilical & Paraumbilical
| Surgery Name | Method | Used For |
|---|---|---|
| Mayo's "Vest-Over-Pants" Repair | Overlapping layers of the linea alba/fascia sutured in 2 layers (no mesh) | Small umbilical/paraumbilical hernias |
| Primary Sutured Repair | Direct closure of defect | Defects < 2 cm |
| Open Mesh Repair (Onlay/Sublay) | Mesh placed on top of (onlay) or beneath (sublay/retromuscular) the fascia | Defects > 2–3 cm; reduces recurrence |
| Laparoscopic IPOM | Mesh deployed intraperitoneally via laparoscope | Large umbilical/paraumbilical hernias |
Incisional Hernia
| Surgery Name | Method | Notes |
|---|---|---|
| Rives-Stoppa Repair | Mesh placed in retromuscular (sublay) space between posterior rectus sheath and rectus muscle | Gold standard open repair; low recurrence |
| Components Separation Technique (CST) | External oblique released + rectus mobilised to close large midline defects | "Loss of domain" hernias; large defects |
| Transversus Abdominis Release (TAR) | Posterior component separation; transversus released to create large retromuscular space | Very large/complex hernias |
| Laparoscopic IPOM | Intraperitoneal mesh with tackers/sutures | Minimally invasive; good for moderate defects |
| eTEP (Extended TEP) | Extended extraperitoneal dissection for retromuscular mesh placement laparoscopically | Emerging; avoids peritoneal entry |
| Onlay Mesh Repair | Mesh placed superficial to fascial repair | Simple; higher infection risk |
Epigastric Hernia
| Surgery Name | Method |
|---|---|
| Simple Fascial Closure | Direct suture for small defects (< 1–2 cm) |
| Open Mesh Repair | For larger defects or recurrent cases |
Spigelian Hernia
| Surgery Name | Method |
|---|---|
| Open Preperitoneal Mesh Repair | Mesh in preperitoneal space via transverse incision |
| Laparoscopic Repair (TAPP / IPOM) | Preferred; avoids difficult anatomy; allows inspection of defect |
Summary Table — Surgical Methods at a Glance
| Surgery Name | Type | Key Principle |
|---|---|---|
| Herniotomy | Open | Sac ligation only (children) |
| Lichtenstein | Open | Tension-free flat mesh |
| Shouldice | Open | 4-layer suture, no mesh |
| Bassini | Open | Tension suture (historical) |
| McVay | Open | Cooper's ligament repair |
| Desarda | Open | Mesh-free aponeurosis flap |
| TEP | Laparoscopic | Extraperitoneal mesh, no peritoneal entry |
| TAPP | Laparoscopic | Transperitoneal, preperitoneal mesh |
| Robotic (RARP) | Robotic | Precise TEP/TAPP |
| Mayo's Repair | Open | Vest-over-pants fascial overlap |
| Rives-Stoppa | Open | Retromuscular sublay mesh |
| Components Separation (CST) | Open | Fascial release for large defects |
| TAR | Open | Posterior component separation |
| Laparoscopic IPOM | Laparoscopic | Intraperitoneal onlay mesh |
| eTEP | Laparoscopic | Extended extraperitoneal retromuscular mesh |
Key Principle: The choice of surgery depends on hernia type, size, patient fitness, recurrence risk, and surgeon experience. Tension-free mesh repair (open Lichtenstein or laparoscopic TEP/TAPP) is the modern standard for inguinal hernias, while Rives-Stoppa / retromuscular sublay is preferred for incisional hernias.
Differnce between in males and females
inguinal hernia differences males females anatomy incidence gender
inguinal hernia male female anatomy comparison inguinal canal
Hernias in Males vs. Females — Key Differences
1. Incidence
| Males | Females | |
|---|---|---|
| Inguinal hernia | Extremely common — most common hernia in men | ~10 times less common (Bailey & Love, p. 1086) |
| Femoral hernia | Rare | More common in females (wider pelvis, broader femoral canal) |
| Umbilical / Paraumbilical | Moderate | More common (pregnancy, multiparity) |
| Incisional hernia | Comparable | Comparable |
2. Anatomical Differences — Inguinal Canal
| Feature | Male | Female |
|---|---|---|
| Canal width | Wider (transmits spermatic cord) | Narrower (transmits only round ligament) |
| Canal contents | Spermatic cord, ilioinguinal nerve, genital branch of genitofemoral nerve | Round ligament of uterus, ilioinguinal nerve |
| Deep inguinal ring | Larger | Smaller |
| Processus vaginalis | Descends with testis into scrotum → remains patent longer → indirect hernia | Nuck's canal (equivalent) — obliterates early; rarely remains patent |
| Posterior wall | Weaker in older males due to muscle atrophy | Relatively stronger |
3. Intraoperative Anatomy — Female Inguinal Hernia (TAPP View)
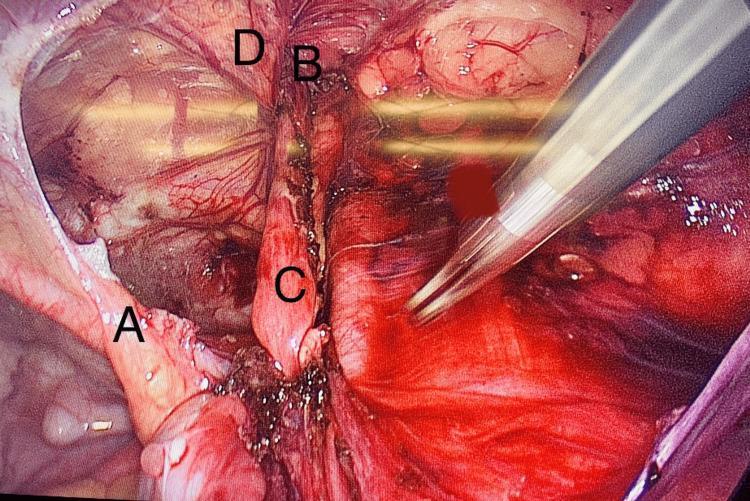
- (A) Medial umbilical ligament
- (B) Deep inguinal ring — site of herniation
- (C) Round ligament of uterus entering the inguinal canal
- (D) Inferior epigastric vessels (medial boundary of indirect hernia)
In females, the round ligament replaces the spermatic cord. During repair, it may be divided or preserved — division does not cause significant clinical problems.
4. Type of Hernia Predominance
| Hernia Type | Males | Females |
|---|---|---|
| Indirect inguinal | Very common (patent processus vaginalis) | Less common; via Nuck's canal |
| Direct inguinal | Common in older men (posterior wall weakness) | Rare |
| Femoral | Rare | Relatively more frequent |
| Umbilical | Present | More common (due to pregnancy) |
| Paraumbilical | Present | More common (obesity, multiparity) |
5. Hernia Contents — Sex-Specific Differences
| Sex | Possible Hernia Contents |
|---|---|
| Male | Omentum, small bowel, rarely bladder; testis may be involved (inguinoscrotal hernia) |
| Female | Omentum, small bowel; ovary and fallopian tube (especially in children — "sliding hernia" of ovary); uterine fibroids (rare); round ligament |
Ovarian herniation is particularly important in female infants and children — an irreducible lump in the groin may represent a herniated ovary and requires prompt surgical attention to avoid torsion and infarction.
6. Presentation Differences
| Feature | Males | Females |
|---|---|---|
| Visible / palpable lump | Groin → may extend into scrotum | Groin lump; may extend into labium majus |
| Scrotal / labial swelling | Inguinoscrotal hernia — easily visible | Labial swelling — may be confused with cyst of canal of Nuck or lymphadenopathy |
| Misdiagnosis | Rare — anatomy straightforward | More common — femoral hernia and lymph nodes may mimic inguinal hernia |
| Ovarian hernia (children) | N/A | Firm, irreducible lump — often mistaken for lymph node |
7. Surgical Considerations
| Aspect | Males | Females |
|---|---|---|
| Standard repair | Lichtenstein / TEP / TAPP | Same — Lichtenstein / TEP / TAPP |
| Herniotomy (children) | Standard; easy sac ligation | Standard; round ligament may need to be preserved |
| Round ligament | Not present | May be divided during repair (no significant consequence) |
| Risk to reproductive structures | Vas deferens and testicular artery at risk → infertility, testicular atrophy | Fallopian tube and ovary at risk in sac (especially in children) |
| Nuck's canal cyst | N/A | May coexist with hernia; needs excision |
| Laparoscopic anatomy | Triangle of doom (external iliac vessels), triangle of pain (lateral cutaneous + femoral nerve) | Same triangles apply — critical to avoid |
| Recurrence | Slightly higher (larger defect, higher activity) | Slightly lower overall |
8. Summary Comparison Table
| Feature | Male | Female |
|---|---|---|
| Inguinal hernia frequency | Very common (~10× more) | Uncommon |
| Femoral hernia frequency | Rare | Relatively more common |
| Inguinal canal width | Wider | Narrower |
| Canal contents | Spermatic cord | Round ligament |
| Processus vaginalis | Persists longer → indirect hernia | Nuck's canal — obliterates early |
| Hernia descends into | Scrotum | Labium majus |
| Special contents risk | Testis, vas deferens | Ovary, fallopian tube |
| Diagnosis difficulty | Easier | Harder (femoral hernia often missed) |
| Complication: infertility | Yes (vas/testicular artery injury) | Less relevant |
| Umbilical/paraumbilical | Present | More common (pregnancy-related) |
Clinical Pearl: In females, femoral hernia must always be excluded when a groin lump is found — it is proportionally more common and has a higher strangulation risk than inguinal hernia due to the rigid femoral ring. In female infants, a groin lump is a herniated ovary until proven otherwise.