Malformations of the musculoskeletal system in children. muscular torticollis
Reading File
search_medical_text
muscular torticollis children congenital etiology diagnosis treatment
search_medical_image
muscular torticollis child neck deformity sternocleidomastoid
GradeResponse
GradeResponse
Muscular Torticollis in Children
Definition
Congenital Muscular Torticollis (CMT) is a postural deformity of the neck characterized by unilateral contracture of the sternocleidomastoid (SCM) muscle, resulting in lateral head tilt toward the affected side and rotation of the chin toward the opposite side.
Etiology and Pathogenesis
The exact cause remains debated, but the leading theories include:
- Intrauterine moulding — abnormal fetal positioning in the uterus leads to compartment syndrome-like ischemia of the SCM, followed by fibrosis (Bailey & Love, p. 651)
- Birth trauma — difficult deliveries (breech presentation, forceps use) may cause SCM injury with subsequent hematoma and fibrous replacement
- Venous occlusion theory — venous obstruction during labor causes edema and muscle necrosis
- Intrauterine crowding — associated with other positional deformities (hip dysplasia, metatarsus adductus)
The fibrotic process within the SCM leads to a fibromuscular mass ("SCM tumor" or pseudotumor) palpable in the neonatal period, which gradually resolves or persists as a contracture.
Classification
| Type | Features |
|---|---|
| Postural torticollis | No SCM mass or tightness; purely positional; most benign |
| Muscular torticollis | Tight SCM without discrete mass |
| SCM tumor/mass type | Palpable fibrous mass within SCM; highest risk of persistent deformity |
Clinical Presentation
Neonatal period:
- Palpable firm, non-tender mass within the SCM (fibrous pseudotumor), typically appearing at 2–4 weeks of age
- Head tilts to the ipsilateral side (toward the shortened muscle)
- Chin rotates to the contralateral side
- Restricted passive cervical rotation
Infants and older children (if untreated):
- Plagiocephaly — flattening of the skull ipsilateral to the tilt
- Facial asymmetry (hemihypoplasia) — the face on the affected side appears flattened and smaller; develops progressively after 3–6 months
- Compensatory "C-curve" of the trunk and spine
- Oblique pelvic tilt (global postural adaptation)

Diagnosis
Clinical (primary):
- Asymmetric head position, restricted cervical range of motion
- Palpable SCM mass or tightness
- Measure passive rotation and lateral flexion deficit
Ultrasound (first-line imaging):
- Shows thickening and increased echogenicity of the SCM
- Confirms fibrous mass, rules out vascular anomalies
- Non-invasive, no radiation — ideal for infants
Radiography (cervical spine X-ray):
- Excludes bony causes (atlanto-axial instability, Klippel-Feil syndrome, hemivertebrae)
MRI/CT: reserved for atypical cases or when cervical spine anomaly is suspected
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Osseous torticollis (Klippel-Feil, atlanto-axial instability) | Bony abnormalities on X-ray/CT |
| Ocular torticollis | Head tilt corrects with eyes closed; ophthalmologic exam abnormal |
| Neurogenic torticollis | Posterior fossa tumor, syringomyelia — MRI required |
| Spasmodic torticollis | Older children; dystonic, intermittent movements |
| Cervical lymphadenitis / abscess | Tender, warm mass; fever; acute onset |
| Sandifer syndrome | Associated with gastroesophageal reflux; episodic |
Management
Conservative (First-line, initiated early)
Physiotherapy / stretching exercises — mainstay of treatment:
- Passive and active SCM stretching
- Lateral cervical flexion and rotation exercises
- Should begin within the first weeks of life
- Success rate: ~90–95% if started before 3 months of age
Positioning and handling:
- Visual and auditory stimuli placed on the contralateral side to encourage active correction
- "Tummy time" to promote symmetric muscle use
Botulinum toxin (Botox) injection:
- Used as an adjunct in refractory cases before surgery
- Temporarily reduces SCM tension, augments physiotherapy
Surgical (Second-line)
Indicated when:
- Conservative treatment fails after 6–12 months
- Significant residual deficit after 12–18 months of age
- Progressive facial asymmetry (Bailey & Love, p. 651)
Procedure — SCM release (tenotomy/myotomy):
- Distal release (sternal and/or clavicular head) — most common
- Bipolar release (origin + insertion) — for severe contractures
- Post-operative physiotherapy and neck orthosis essential
Outcomes: Best results when surgery is performed before 5 years of age. Facial asymmetry partially remodels after surgery in younger children but may be permanent if delayed.
Complications of Untreated Torticollis
- Permanent facial asymmetry / hemihypoplasia
- Plagiocephaly
- Cervical scoliosis and compensatory thoracic scoliosis
- Visual disturbances (from chronic head tilt)
- Psychological impact (cosmetic deformity)
Prognosis
| Factor | Outcome |
|---|---|
| Early diagnosis + physiotherapy (<3 months) | Excellent; ~90–95% resolution |
| SCM mass type | Poorer conservative prognosis; more likely to need surgery |
| Treatment started after 1 year | Higher surgical rate |
| Surgery before age 5 | Good functional and cosmetic outcome |
| Surgery after age 5 | Functional improvement but facial asymmetry may persist |
Key takeaway: CMT is the most common cause of neck deformity in infants. Early diagnosis and aggressive physiotherapy before 3 months of age yields excellent outcomes. The SCM mass type and delayed treatment are the main predictors of surgical need. Facial asymmetry is the most important long-term complication to prevent through timely intervention.
Bailey and Love's Short Practice of Surgery, 28th Ed., p. 651
Hernias: hernias of the anterior abdominal wall, inguinal hernias
search_medical_text
anterior abdominal wall hernias umbilical epigastric incisional classification anatomy
search_medical_text
inguinal hernia anatomy types direct indirect diagnosis treatment surgery
search_medical_image
inguinal hernia anatomy direct indirect canal
GradeResponse
GradeResponse
GradeResponse
Hernias of the Anterior Abdominal Wall and Inguinal Hernias
General Definition
A hernia is the protrusion of a viscus (or part of it) through a defect or weakness in the wall of the cavity in which it is normally contained. Every hernia has three components:
- Sac — peritoneal outpouching
- Contents — bowel, omentum, bladder, ovary, etc.
- Coverings — layers of abdominal wall draped over the sac
PART I — Hernias of the Anterior Abdominal Wall (Ventral Hernias)
The term ventral hernia refers to hernias occurring in the anterior abdominal wall, excluding inguinal and femoral hernias (though lumbar hernia is included despite its dorsolateral position). The European Hernia Society (EHS) classification (2009) divides them into:
- Primary ventral hernias — occur spontaneously at anatomically weak points
- Incisional hernias — occur at previous surgical wounds (Bailey & Love, 28th Ed., p. 1093)
1. Umbilical Hernia
In Infants
- Due to failure of the umbilical ring to close after birth
- Very common; majority close spontaneously by 3–4 years of age
- Surgical repair indicated if persists beyond age 4–5 or if ring diameter > 1.5 cm
In Adults
- Strictly termed paraumbilical hernia — hernia passes through a defect just above or below the umbilical ring (not through it)
- More common in obese, multiparous women
- Contents: omentum, transverse colon, small bowel
- Risk of strangulation is relatively high — elective repair recommended even if asymptomatic
- Repair: Mayo "vest-over-pants" repair or mesh repair for larger defects
2. Epigastric Hernia
- Occurs through defects in the linea alba between xiphoid process and umbilicus
- Usually small; contains extraperitoneal fat (pre-peritoneal fat plug), rarely a true sac
- More common in young adult males
- Often multiple; frequently symptomatic (pain disproportionate to size)
- Treatment: surgical closure; mesh for larger defects
3. Incisional Hernia
- Develops through a previous surgical incision in the abdominal wall
- Risk factors:
- Wound infection, dehiscence
- Obesity, malnutrition, steroid use
- Poor surgical technique (excessive tension, inadequate closure)
- Midline incisions carry highest risk
EHS Classification — based on:
- Location (midline vs. lateral)
- Width of defect (W1 <4 cm, W2 4–10 cm, W3 >10 cm)
- Recurrent vs. primary
Treatment:
- Small defects: primary suture repair
- Defects ≥ 4 cm: mesh repair (open or laparoscopic) — lower recurrence rate
- Component separation technique for massive defects
4. Spigelian Hernia
- Occurs through the spigelian fascia (aponeurosis of the transversus abdominis) at the lateral border of the rectus sheath, typically just below the arcuate line
- Interparietal — sac lies between muscle layers (difficult to detect clinically)
- Often missed on examination; diagnosed by ultrasound or CT
- High risk of strangulation
- Treatment: surgical repair (laparoscopic preferred)
5. Lumbar Hernia
- Through the superior lumbar triangle (Grynfeltt) or inferior lumbar triangle (Petit)
- Rare; often contains retroperitoneal fat
- Treatment: mesh repair
6. Obturator Hernia
- Through the obturator canal in the obturator foramen
- Predominantly elderly, thin women
- Classic sign: Howship-Romberg sign — pain along inner thigh (obturator nerve compression)
- Frequently presents as small bowel obstruction; diagnosed on CT
- High morbidity due to delayed diagnosis
PART II — Inguinal Hernias
Anatomy of the Inguinal Canal
The inguinal canal is an oblique passage (~4 cm long) in the lower anterior abdominal wall:
| Structure | Details |
|---|---|
| Deep (internal) ring | Defect in transversalis fascia; lateral to inferior epigastric vessels |
| Superficial (external) ring | Defect in external oblique aponeurosis; above pubic tubercle |
| Anterior wall | External oblique aponeurosis (+ internal oblique laterally) |
| Posterior wall | Transversalis fascia (+ conjoint tendon medially) |
| Roof | Arched fibers of internal oblique and transversus abdominis |
| Floor | Inguinal ligament (Poupart) + lacunar ligament medially |
Contents of the canal:
- In males: spermatic cord (vas deferens, testicular artery, pampiniform plexus, cremasteric muscle, processus vaginalis remnant) + ilioinguinal nerve
- In females: round ligament of the uterus + ilioinguinal nerve
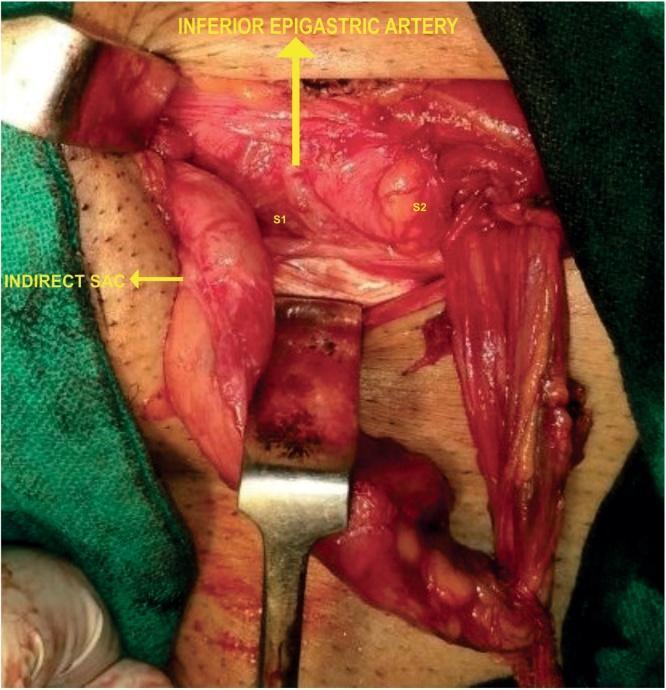
The inferior epigastric artery (branch of external iliac) runs on the posterior abdominal wall just medial to the deep ring — this is the key landmark distinguishing indirect from direct hernias.
Classification of Inguinal Hernias
(Bailey & Love, 28th Ed., p. 1086)
| Feature | Indirect (Lateral/Oblique) | Direct (Medial) |
|---|---|---|
| Path | Through deep ring → inguinal canal → superficial ring | Directly through posterior wall (Hesselbach's triangle) |
| Relation to inferior epigastric vessels | Lateral to vessels | Medial to vessels |
| Sac | Enters spermatic cord (covered by all cord coverings) | No cord involvement |
| Origin | Congenital (patent processus vaginalis) or acquired | Acquired (weakness of transversalis fascia) |
| Age | All ages; most common in young males | Middle-aged to elderly males |
| Neck | Narrow — high strangulation risk | Wide — low strangulation risk |
| Descent into scrotum | Yes (can become scrotal) | Rarely |
| Reduction on pressure | Lateral pressure controls | Not controlled laterally |
Hesselbach's triangle (site of direct hernia):
- Medially: lateral border of rectus abdominis
- Laterally: inferior epigastric vessels
- Inferiorly: inguinal ligament
Epidemiology
- Most common hernia overall (~75% of all hernias)
- Lifetime risk: 27% in males, 3% in females
- Right side > left side (due to later descent of right testis)
- Indirect > direct (ratio ~2:1)
- Bilateral in ~20% of cases
Clinical Presentation
Symptoms:
- Groin lump, typically appearing on standing/straining and reducing on lying down
- Dragging, aching discomfort
- In scrotal hernias: visible and palpable scrotal swelling
Signs:
- Visible/palpable impulse on coughing
- Invagination test: finger in superficial ring — indirect hernia impacts fingertip, direct hernia impacts pulp
- Reducibility assessment
- Irreducibility = hernia cannot be reduced (may still be viable)
- Obstruction = bowel obstruction without vascular compromise
- Strangulation = vascular compromise → surgical emergency
Imaging
Usually a clinical diagnosis. Imaging is used in:
- Uncertain or occult hernias: ultrasound (first line)
- Complex cases, recurrence, or pre-operative planning: CT scan
- Identification of bilateral occult hernias: MRI (sports hernia evaluation)
Differential Diagnosis of Groin Swelling
| Condition | Key Feature |
|---|---|
| Femoral hernia | Below and lateral to pubic tubercle; more common in women |
| Lymphadenopathy | Firm, non-reducible nodes; look for source of infection/malignancy |
| Hydrocele | Transilluminates; cannot get above it; testicular |
| Varicocele | "Bag of worms" consistency; left side predominant |
| Undescended testis | Absent testis in scrotum |
| Lipoma of cord | Soft, reducible, no impulse on cough |
| Femoral artery aneurysm | Pulsatile; non-reducible |
| Psoas abscess | Fluctuant; systemic signs; comes from above inguinal ligament |
Management
Conservative
- Watchful waiting is acceptable for asymptomatic or minimally symptomatic direct inguinal hernias (low strangulation risk)
- Truss: rarely used; not curative; may mask symptoms
Surgical Repair
Indications: symptomatic hernia, irreducibility, strangulation/obstruction, all indirect hernias (high strangulation risk), all hernias in children
Open Repair
| Technique | Principle |
|---|---|
| Lichtenstein tension-free mesh repair | Gold standard for open repair; polypropylene mesh placed in inguinal canal |
| Shouldice repair | Multi-layer sutured repair of posterior wall; best non-mesh results |
| Bassini repair | Historical; sutured repair; higher recurrence |
| Herniotomy (in children) | Simple sac ligation without posterior wall repair |
Laparoscopic / Minimally Invasive Repair
(Bailey & Love, p. 1086)
| Technique | Approach |
|---|---|
| TAPP (Trans-Abdominal Pre-Peritoneal) | Laparoscopic; peritoneum incised, mesh placed, peritoneum closed |
| TEP (Totally ExtraPeritoneal) | Laparoscopic; mesh placed entirely in preperitoneal space; no peritoneal breach |
| RARP (Robot-Assisted) | Emerging; especially for bilateral/complex cases |
Advantages of laparoscopic repair: less post-op pain, faster recovery, better for bilateral hernias and recurrent hernias after open repair.
Complications
Intraoperative: injury to vas deferens, spermatic vessels, ilioinguinal/genitofemoral nerves, bladder, bowel
Post-operative:
| Complication | Notes |
|---|---|
| Seroma / hematoma | Most common early complication |
| Wound infection | Higher with mesh → mesh infection rare but serious |
| Urinary retention | Especially in elderly males |
| Chronic groin pain | Inguinodynia; neuropathic; most feared long-term complication |
| Testicular atrophy | Injury to testicular artery |
| Recurrence | ~1–5% with mesh repair; higher with pure tissue repair |
Special Situations
- Strangulated hernia: Emergency repair after resuscitation; bowel resection if non-viable; mesh use controversial in contaminated field
- Inguinal hernia in children: Always indirect (patent processus vaginalis); treated by herniotomy (sac ligation only); high incidence of contralateral patent processus — many surgeons explore both sides
- Inguinal hernia in women: Rare; always exclude femoral hernia; round ligament may be in sac; repair principles same
Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1086, 1093
This is a shared conversation. Sign in to Orris to start your own chat.