phyllodes tumoir
Reading File
search_medical_text
phyllodes tumor breast classification pathology management
search_medical_image
phyllodes tumor breast histology imaging
GradeResponse
GradeResponse
Phyllodes Tumor of the Breast
Overview
Phyllodes tumor (also spelled "cystosarcoma phyllodes") is a rare fibroepithelial neoplasm of the breast, accounting for ~0.3–1% of all breast tumors. The name derives from the Greek phyllon (leaf), reflecting the characteristic leaf-like stromal projections seen histologically. It occurs predominantly in women, with a peak incidence in the 4th–5th decade — roughly 15–20 years later than fibroadenoma.
Classification
Phyllodes tumors are classified into three grades based on histological features:
| Feature | Benign | Borderline | Malignant |
|---|---|---|---|
| Stromal cellularity | Mild | Moderate | Marked |
| Stromal atypia | Mild | Moderate | Marked |
| Mitotic rate | < 5/10 HPF | 5–9/10 HPF | ≥ 10/10 HPF |
| Tumor margins | Well-defined/pushing | Intermediate | Infiltrative |
| Stromal overgrowth | Absent | Focal | Present |
| Proportion of cases | ~60–75% | ~15–20% | ~10–20% |
Histopathology
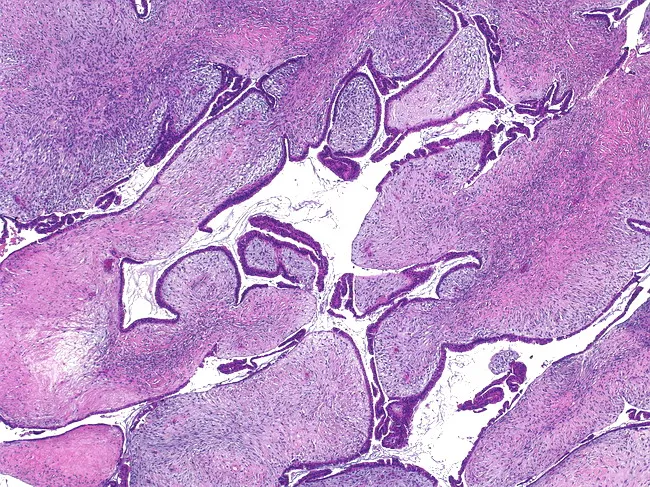
The hallmark is biphasic morphology — both stromal and epithelial components — with:
- Leaf-like fronds of hypercellular stroma projecting into cleft-like, slit-shaped spaces
- Spindle-to-oval stromal cells with variable atypia
- Epithelial glands lining the clefts (no myoepithelial proliferation in the clefts)
- Absence of DCIS
The image below demonstrates the characteristic histology:
Key distinction from fibroadenoma: Phyllodes tumors show stromal overgrowth, increased mitotic activity, and infiltrative margins — fibroadenoma is paucicellular and does not recur after excision.
Clinical Presentation
- Painless, rapidly growing breast mass — often described as enlarging over weeks to months
- Mean size at presentation: 4–5 cm (can be much larger; giant phyllodes tumors >10 cm exist)
- Overlying skin may be stretched, thinned, or show visible veins (due to rapid growth)
- Nipple discharge is uncommon
- Usually unilateral and solitary
- Axillary lymphadenopathy is rare (even in malignant cases)
Diagnosis
Imaging
| Modality | Findings |
|---|---|
| Mammography | Well-circumscribed, lobulated, hyperdense mass; may resemble fibroadenoma |
| Ultrasound | Heterogeneous, hypoechoic mass with internal cleft-like spaces (anechoic areas); increased vascularity on Doppler |
| MRI | Lobulated mass with heterogeneous enhancement; internal septations; high T2 signal |
No imaging modality reliably distinguishes phyllodes from fibroadenoma or between grades — histology is required.
Pathology Workup
- Core needle biopsy (CNB) is the standard preoperative approach — allows stromal assessment
- Fine needle aspiration (FNA) is insufficient (cannot assess architecture)
- Final grading on excisional specimen (CNB may under-grade)
Differential Diagnosis
- Fibroadenoma (most common) — paucicellular stroma, no stromal overgrowth
- Primary breast sarcoma — pure stromal malignancy, no epithelial component
- Metaplastic carcinoma — keratin-positive, no leaf-like architecture
- Giant fibroadenoma — typically in adolescents
Management
Surgery — Cornerstone of Treatment
| Grade | Recommended Surgery |
|---|---|
| Benign | Wide local excision with ≥1 cm clear margins |
| Borderline | Wide local excision with ≥1 cm clear margins |
| Malignant | Wide excision with ≥1 cm margins; mastectomy if margins cannot be achieved |
Key principles:
- Margin status is the most important predictor of local recurrence
- Routine axillary lymph node dissection/SLNB is NOT indicated — nodal metastasis risk is negligible, even for malignant phyllodes (lymphatic spread is rare; hematogenous spread predominates)
- Breast-conserving surgery is preferred when adequate margins can be obtained
Adjuvant Therapy
- Radiation: May be considered for malignant phyllodes with close/positive margins or large tumors; evidence is limited
- Chemotherapy: No established regimen; malignant phyllodes behaves like soft-tissue sarcoma — ifosfamide-based regimens used in metastatic disease
- Hormonal/HER2 therapy: Not indicated (phyllodes tumors are generally ER/PR/HER2-negative in the stromal component)
Recurrence and Metastasis
| Benign | Borderline | Malignant | |
|---|---|---|---|
| Local recurrence | ~10–17% | ~14–25% | ~23–30% |
| Distant metastasis | Rare (<1%) | ~4% | ~22–34% |
| Metastatic sites | — | — | Lung, bone, liver, brain |
- Recurrences often occur within 2 years of surgery
- Recurrent tumors may upgrade in grade
- Malignant phyllodes metastasize hematogenously (not via lymphatics)
Prognosis
- Benign: Excellent — essentially curable with adequate excision
- Borderline: Good with clear margins; surveillance recommended
- Malignant: 5-year overall survival ~60–80%; worse with stromal overgrowth, high mitotic rate, and positive margins
Surveillance
Recommended follow-up (no universal consensus; general practice):
- Clinical exam + imaging every 6–12 months for 2–3 years, then annually
- Contralateral breast surveillance as standard breast cancer screening
Bottom line: Phyllodes tumor is distinguished from fibroadenoma by stromal hypercellularity and overgrowth, requires wide excision with ≥1 cm margins, and does not warrant axillary surgery regardless of grade. Malignant phyllodes behaves as a sarcoma and spreads hematogenously.
This is a shared conversation. Sign in to Orris to start your own chat.