Ulnar claw hand for 10 marks
Reading File
search_medical_text
ulnar claw hand deformity anatomy pathophysiology causes
search_medical_image
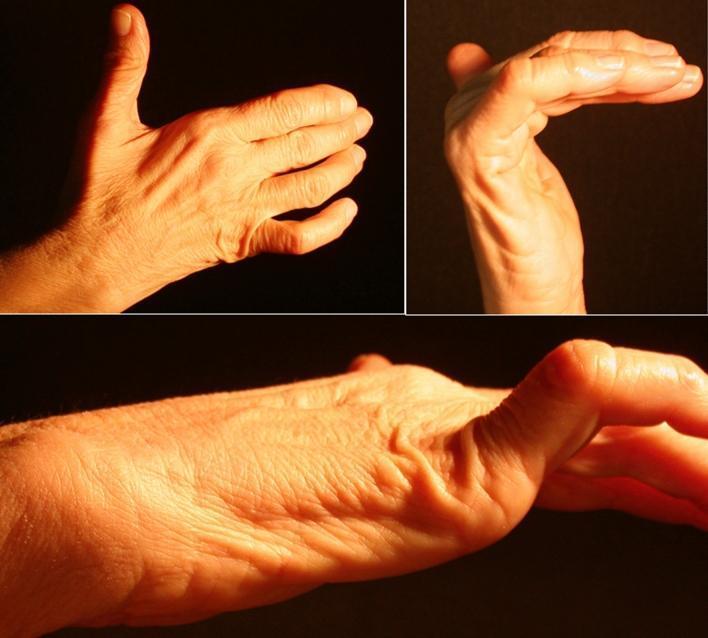
ulnar claw hand deformity
GradeResponse
GradeResponse
search_medical_text
ulnar nerve injury claw hand intrinsic muscles lumbrical interossei paradox
GradeResponse
Here is a comprehensive 10-mark answer on Ulnar Claw Hand:
Ulnar Claw Hand (Main en Griffe)
Definition
Ulnar claw hand is a deformity characterized by hyperextension at the metacarpophalangeal (MCP) joints and flexion at the proximal and distal interphalangeal (PIP and DIP) joints of the ring and little fingers (4th and 5th digits), resulting from ulnar nerve paralysis.
Anatomy and Pathophysiology
The deformity arises due to loss of intrinsic muscle function supplied by the ulnar nerve:
| Muscle | Action Lost |
|---|---|
| Interossei (dorsal & palmar) | MCP flexion + IP extension |
| 3rd and 4th lumbricals | MCP flexion + IP extension of ring & little fingers |
| Hypothenar muscles | Abduction/opposition of little finger |
| Adductor pollicis | Adduction of thumb |
Mechanism:
- Normally, the lumbricals and interossei flex the MCP joints and extend the IP joints
- When the ulnar nerve is injured, these intrinsic muscles are paralyzed
- Unopposed action of extensor digitorum communis (radial nerve) causes MCP hyperextension
- Unopposed action of flexor digitorum superficialis and profundus (median/ulnar nerve) causes IP flexion
- Result: the classic "claw" posture in the ring and little fingers
The Ulnar Paradox
More proximal ulnar nerve injuries produce LESS clawing
| Level of Injury | Clawing |
|---|---|
| Wrist (distal) | Severe clawing of ring & little fingers |
| Elbow (proximal) | Milder clawing |
Reason: In high (elbow-level) lesions, the flexor digitorum profundus (FDP) to ring and little fingers is also paralyzed. Without FDP, there is no force to maintain IP flexion, so the claw is less pronounced.
Causes
A. Traumatic
- Fracture of medial epicondyle
- Elbow dislocation
- Fractures of the hamate/wrist
B. Compressive (Entrapment)
- Cubital tunnel syndrome (elbow) — most common
- Guyon's canal compression (wrist)
C. Infective
- Leprosy — most common cause worldwide (bilateral claw hand due to ulnar + median nerve involvement) (Bailey & Love, p. 100)
- Tuberculosis (cold abscess)
D. Vascular
- Volkmann's ischemic contracture (associated)
E. Other
- Cervical rib (thoracic outlet syndrome)
- Cubitus valgus deformity (tardy ulnar nerve palsy) — late complication of malunited lateral condyle fractures (Bailey & Love, p. 505)
Clinical Features
Posture:
- Clawing of ring and little fingers (hyperextended MCPs, flexed IPs)
- Index and middle fingers relatively spared (supplied by median nerve lumbricals)
Wasting:
- Hypothenar eminence wasting
- Hollowing of interosseous spaces (dorsal guttering)
- Flattening of the medial palm
Sensory Loss:
- Little finger and medial half of ring finger (palmar and dorsal)
- Medial aspect of palm (Guyon's canal lesion spares dorsum)
Motor Loss / Special Tests:
- Froment's sign — patient grips paper between thumb and index; uses FPL (flexor pollicis longus) instead of adductor pollicis → thumb IP joint flexes
- Wartenberg's sign — little finger abducted at rest (unopposed abductor digiti minimi)
- Card test / Egawa's test — inability to abduct/adduct fingers
Differences: High vs. Low Ulnar Nerve Lesion
| Feature | High (Elbow) | Low (Wrist) |
|---|---|---|
| FDP to ring & little finger | Paralyzed | Intact |
| Clawing severity | Less (ulnar paradox) | More severe |
| Sensory loss | Ring, little, medial forearm | Ring, little finger only |
| Hypothenar wasting | Yes | Yes |
| Flexor carpi ulnaris | Paralyzed | Intact |
Management
Conservative
- Splinting: Knuckle-bender splint — maintains MCP flexion to restore intrinsic-plus position
- Physiotherapy and occupational therapy
- Treat underlying cause (e.g., dapsone + MDT for leprosy)
Surgical
A. For the nerve:
- Decompression (cubital tunnel release, Guyon's canal release)
- Ulnar nerve transposition (anterior transposition at elbow)
- Nerve repair/grafting for transection injuries
B. For the deformity (static correction):
- Fowler's procedure — release of extensor mechanism at MCP level
- Zancolli lasso procedure — FDS tendon looped through A1 pulley to flex MCP joint
- Tendon transfers — e.g., FDS to lateral bands (Brand's procedure) to restore intrinsic function
- Capsulodesis of MCP joints
Summary
Ulnar claw hand results from ulnar nerve palsy causing loss of intrinsic muscles (interossei + medial two lumbricals), leading to unopposed extrinsic flexion and extension producing clawing of the ring and little fingers. The ulnar paradox dictates that distal lesions cause more clawing than proximal ones. Management depends on the level and cause of the lesion, ranging from splinting and nerve decompression to tendon transfer procedures.
This is a shared conversation. Sign in to Orris to start your own chat.