Collapse of lung lobes and thier findings in x ray and ct With images and explaination
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive textbook content and images from Grainger & Allison's Diagnostic Radiology. Let me compile the complete answer.
Collapse of Lung Lobes: X-ray and CT Findings
Source: Grainger & Allison's Diagnostic Radiology, 7th edition
Terminology
"Collapse" and "atelectasis" are used interchangeably and refer to loss of volume within the lung. In practice:
- "Collapse" = complete loss of volume of an entire lobe/lung
- "Atelectasis" = partial or complete loss, described by extent (subsegmental, sublobar, lobar) or by cause
General Radiographic Principles
The two cardinal features of any lobar collapse are:
- Increased opacity of the affected lobe
- Volume loss - assessed by direct and indirect signs
| Sign Type | Examples |
|---|---|
| Direct (volume loss) | Displacement of fissures, pulmonary vessels, bronchi |
| Indirect (compensatory) | Hyperinflation of other lobes, mediastinal shift, hemidiaphragm elevation, narrowing of intercostal spaces |
Special Ancillary Signs
- Golden's S sign (reverse-S sign on the right): S-shaped fissure due to combined collapse + central mass, suggesting bronchogenic carcinoma as the cause
- Absence of air bronchograms: Suggests endobronchial obstruction rather than consolidation
- Luftsichel sign: "Air crescent" seen in left upper lobe collapse - aerated lung interposed between the aortic arch and the medial border of the collapse
- Juxtaphrenic peak sign: Small triangular density near hemidiaphragm in upper lobe collapse, due to reorientation of an inferior accessory fissure
- Shifting granuloma sign: A calcified granuloma changes position between serial films due to volume loss
Schematic of All Lobar Collapses
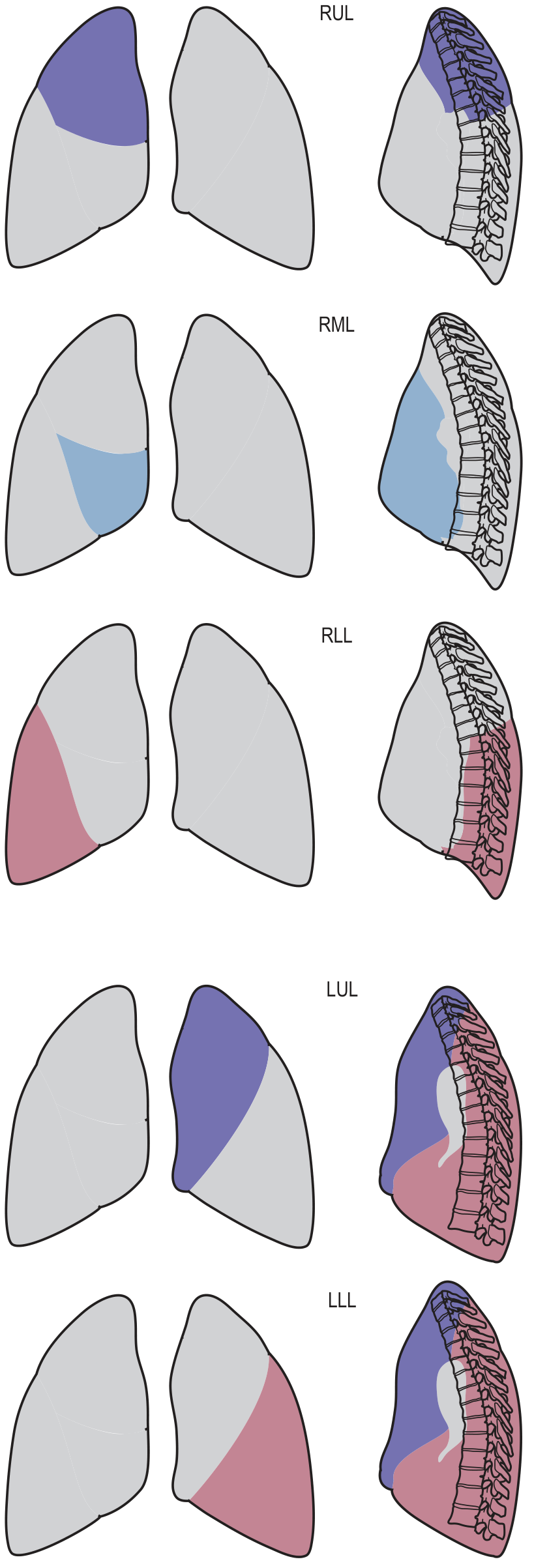
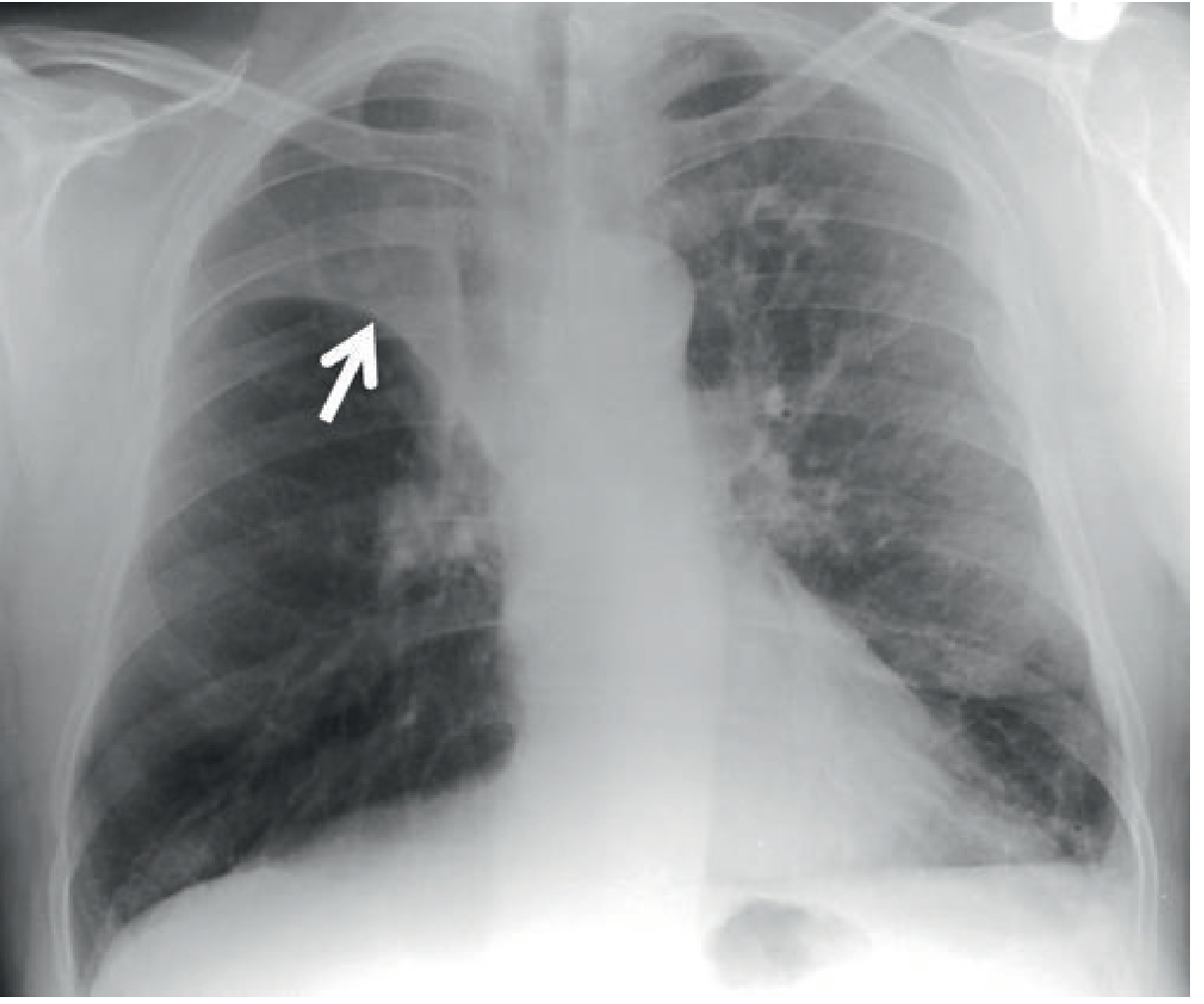
1. Right Upper Lobe (RUL) Collapse
Mechanism
Volume loss is primarily superior and medial. The horizontal fissure displaces upward.
Chest X-ray (PA view)
- Increased opacity at the right apex, adjacent to the mediastinum
- Horizontal fissure elevated with a concave inferior border
- Small convexity at the hilum (from pulmonary vessels) = early Golden's S sign
- In tight collapse: can mimic an apical pleural cap or mediastinal widening
- Compensatory hyperinflation of right middle and lower lobes + left upper lobe
- Right main bronchus and lower lobe bronchus take a more horizontal course
Chest X-ray (Lateral view)
- Both horizontal and oblique fissures displaced superiorly and medially
- Collapsed lobe forms a superior ill-defined wedge-shaped density
CT Findings
- Roughly triangular density with base anteriorly against chest wall and apex at hilum
- Focal bulge of lateral border = underlying mass (suggests carcinoma)
- Compensatory hyperinflation of RML, RLL, and even left upper lobe
X-ray Image
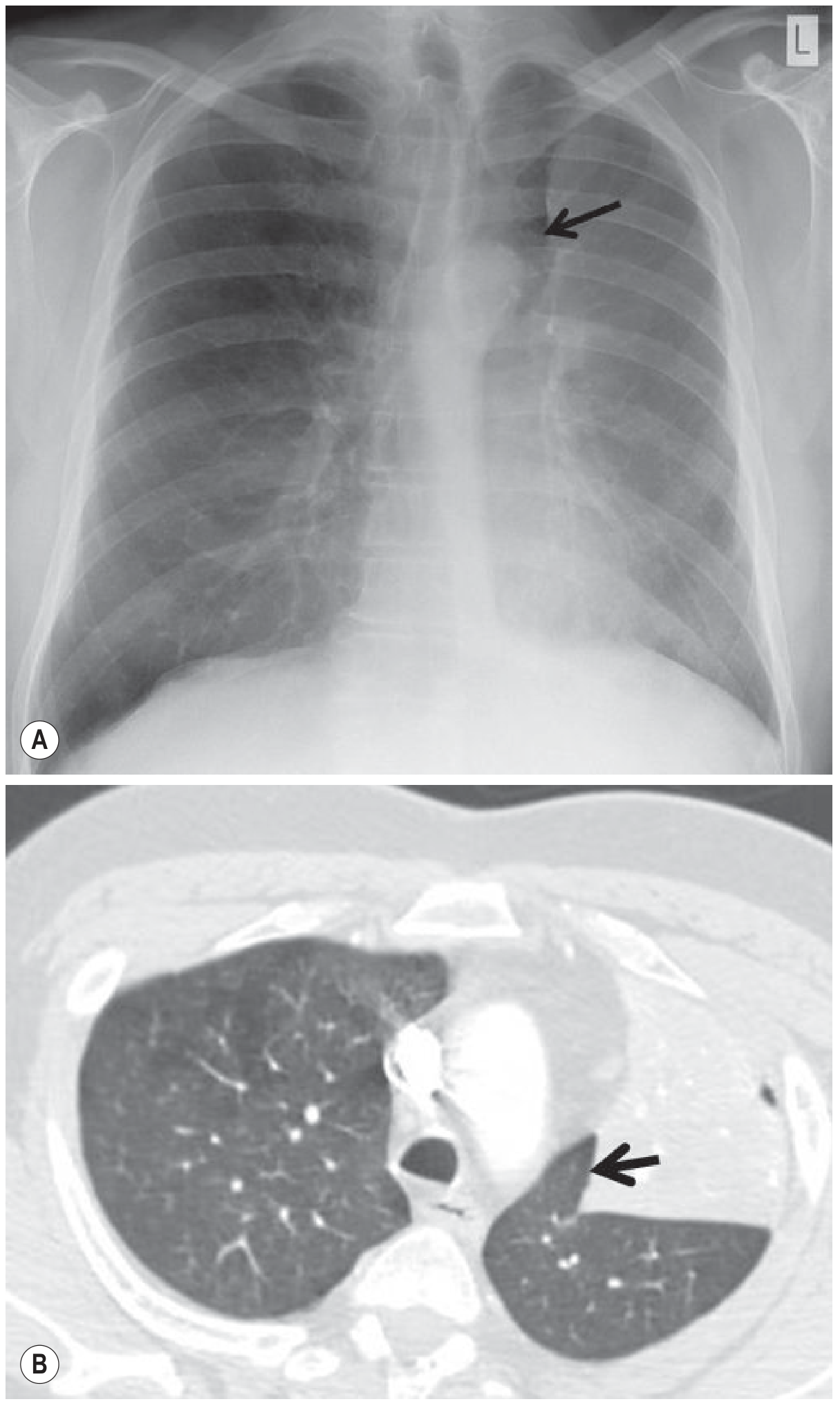
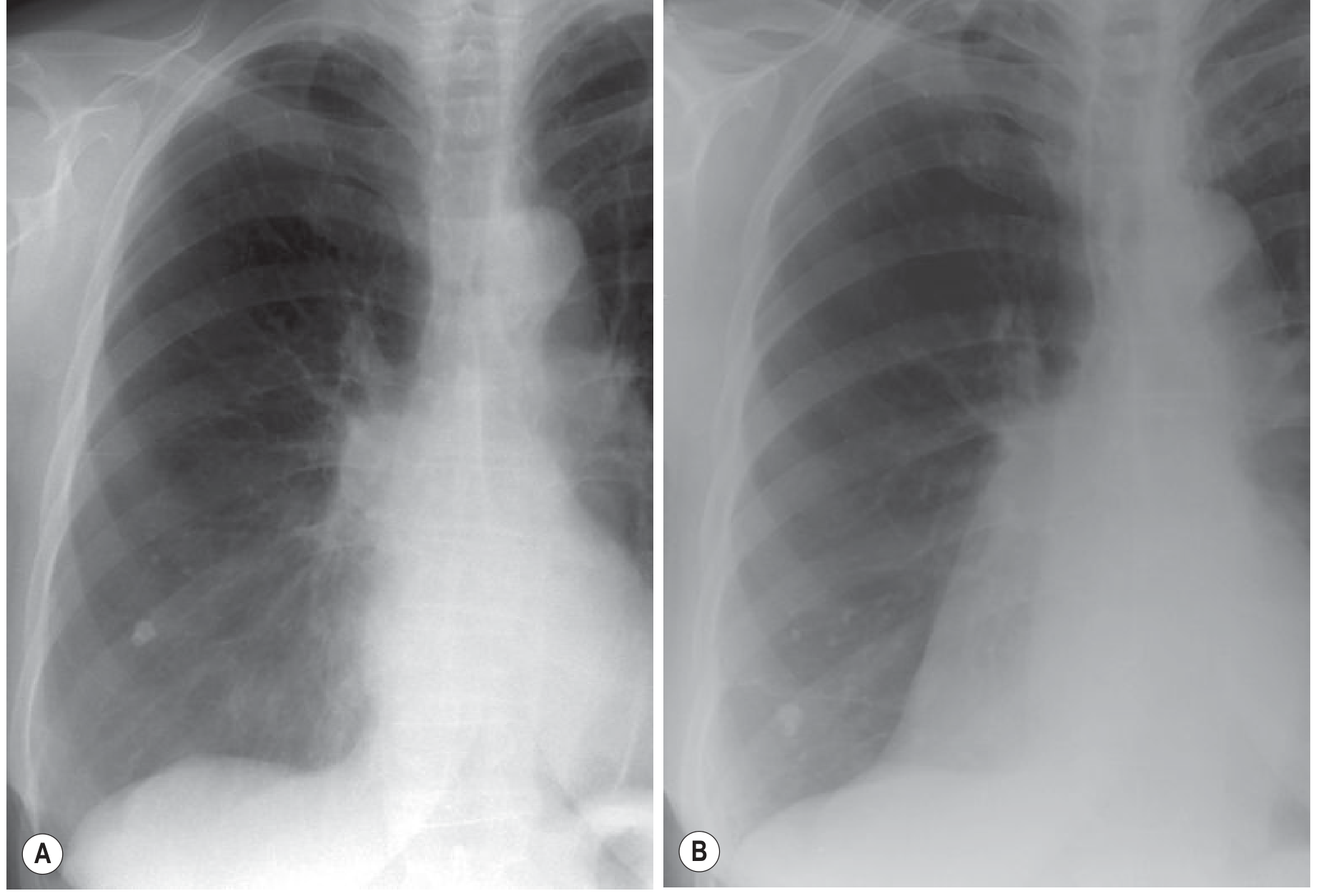
2. Left Upper Lobe (LUL) Collapse
Key Difference from RUL Collapse
There is rarely a horizontal fissure on the left, so the direction of collapse is anterior and medial, not superior.
Chest X-ray (PA view)
- Veil-like increased density of the entire left hemithorax - most dense at the hilum, gradually fading laterally
- No clear inferior demarcation (unlike RUL collapse)
- Luftsichel sign: Paramediastinal lucency due to aerated lower lobe slipping upward between the collapse and the aortic arch
- Left heart border, left mediastinal outline, and aortic knuckle may be obscured (in less severe collapse)
- In more severe collapse, aortic knuckle may paradoxically become visible again (lower lobe hyperinflates superiorly)
- Increased angulation between left main bronchus and lower lobe bronchus
- On lateral: entire oblique fissure displaced anteriorly, parallel to chest wall. Increased retrosternal lucency.
CT Findings
- Triangular soft-tissue density, apex at upper lobe bronchus, base against anterior chest wall adjacent to left mediastinal border
- Lingular segment is a separate density closely opposed to the left heart border
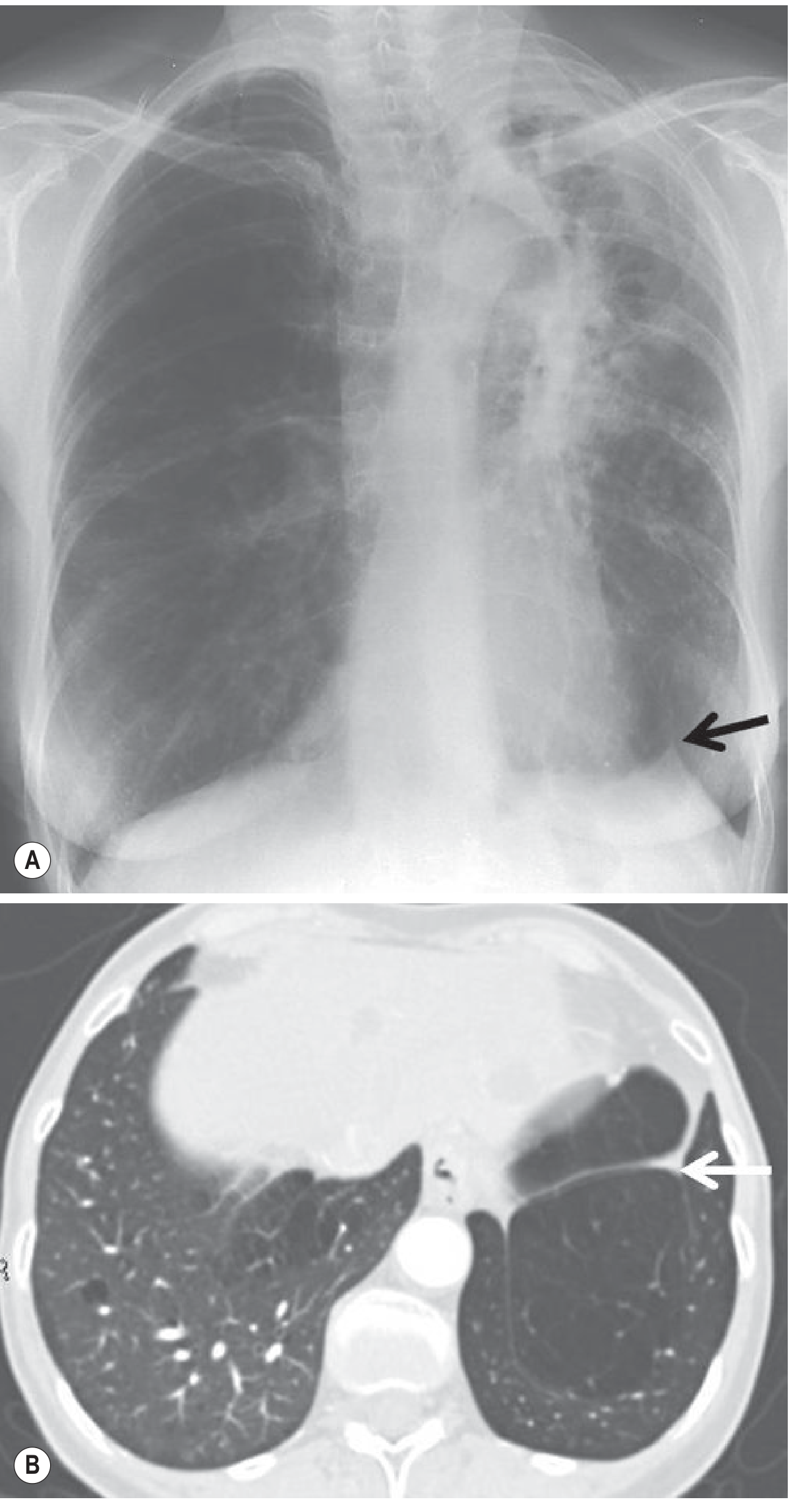
Luftsichel Sign (X-ray + CT)
Left Upper Lobe Collapse (Frontal + Lateral X-ray)
3. Right Middle Lobe (RML) Collapse
Chest X-ray (PA view)
- Findings can be very subtle on the frontal view - easy to miss
- Collapsed lobe lies against the right heart border → loss of right heart border silhouette
- May show only indistinctness of the right atrial border
- When collapse is parallel to the x-ray beam or the patient is in a lordotic position: triangular "sail-shaped" density adjacent to the heart
- The opacity itself may not be visible at all on the frontal view
Chest X-ray (Lateral view)
- Much more obvious on lateral: triangular density with approximation of the minor fissure and inferior major fissure, apex at hilum
- In severe collapse, fissures become nearly parallel - thin wedge of density between them
CT Findings
- Triangular-shaped density adjacent to the heart border
- Because collapse represents a flat sheet of tissue, only a small portion may be seen on each axial slice
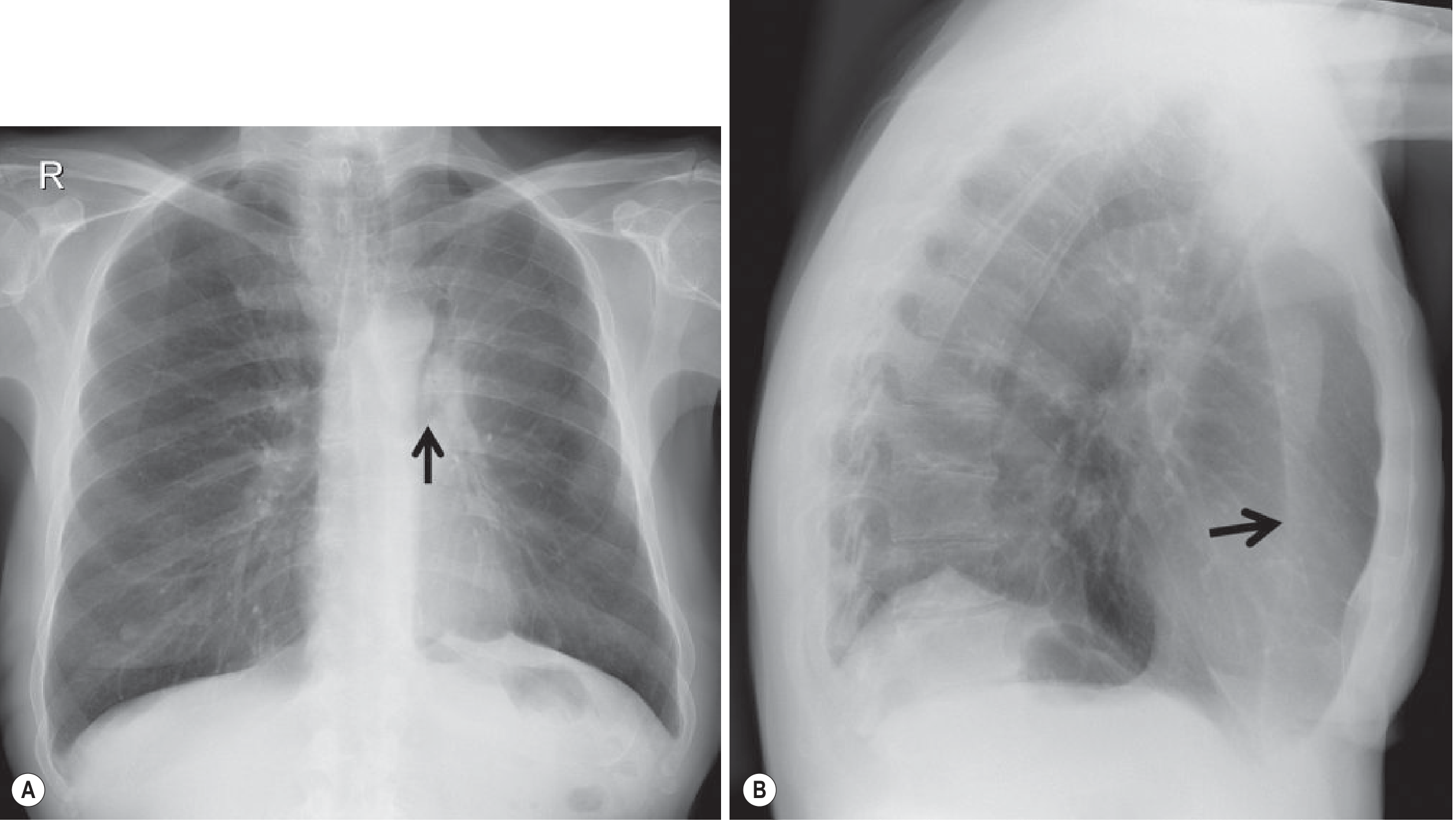
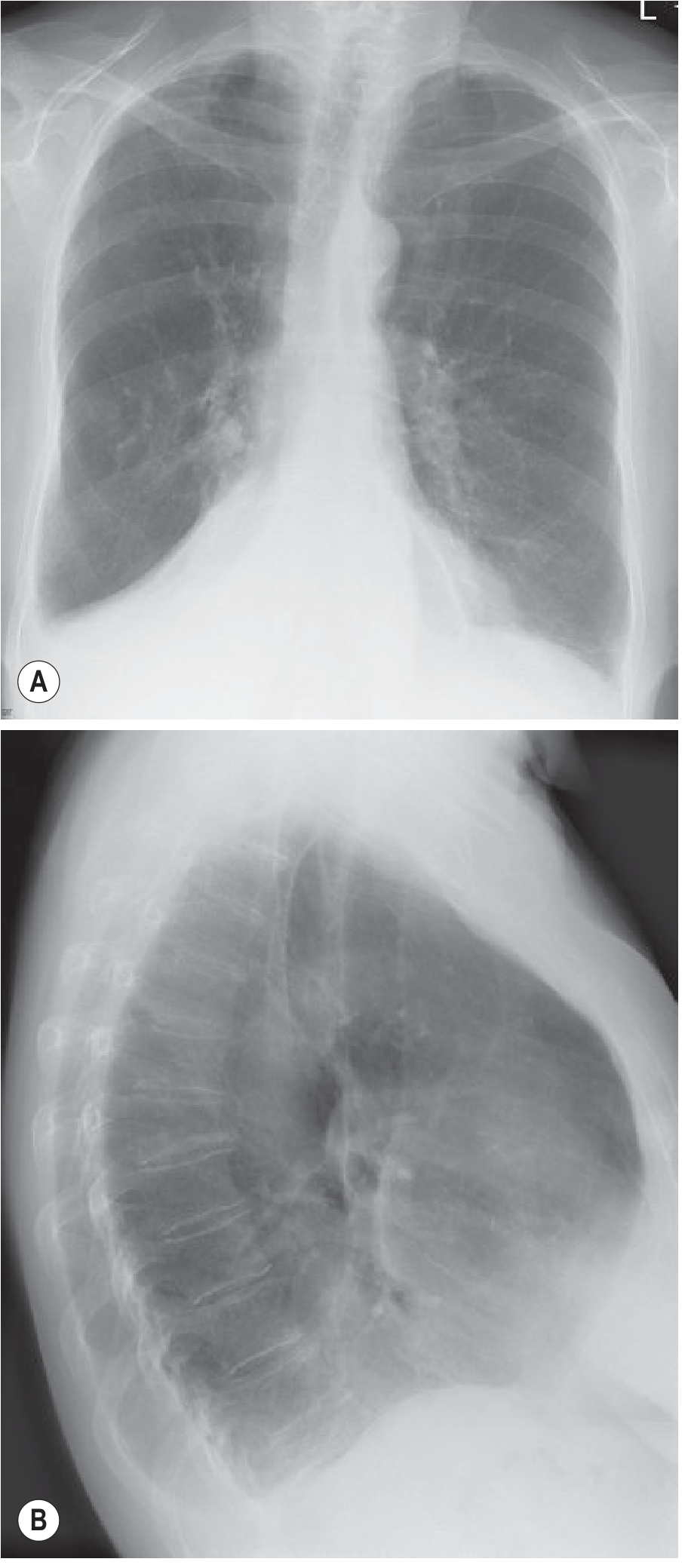
4. Right Lower Lobe (RLL) and Left Lower Lobe (LLL) Collapse
These two lobes behave very similarly.
Direction of Collapse
The oblique fissure moves posteriorly and medially; collapsed lobe lies in the posteromedial chest.
Chest X-ray (PA view)
- Triangular density behind the heart (posteromedial)
- Medial portion of the hemidiaphragm obscured (no longer outlined by aerated lung)
- Hilar structures may be depressed
Chest X-ray (Lateral view)
- Posterior portion of the hemidiaphragm may not be visible
- Vertebral column appears progressively denser inferiorly (reversed normal transparency gradient)
- In more severe collapse, diaphragm may reappear as it is outlined by hyperinflated upper lobe
CT Findings
- Collapsed lobe seen as a posteromedial wedge of density
- Volume loss readily appreciated
Juxtaphrenic Peak Sign (LLL collapse shown)
Shifting Granuloma Sign (Before and After Lower Lobe Collapse)
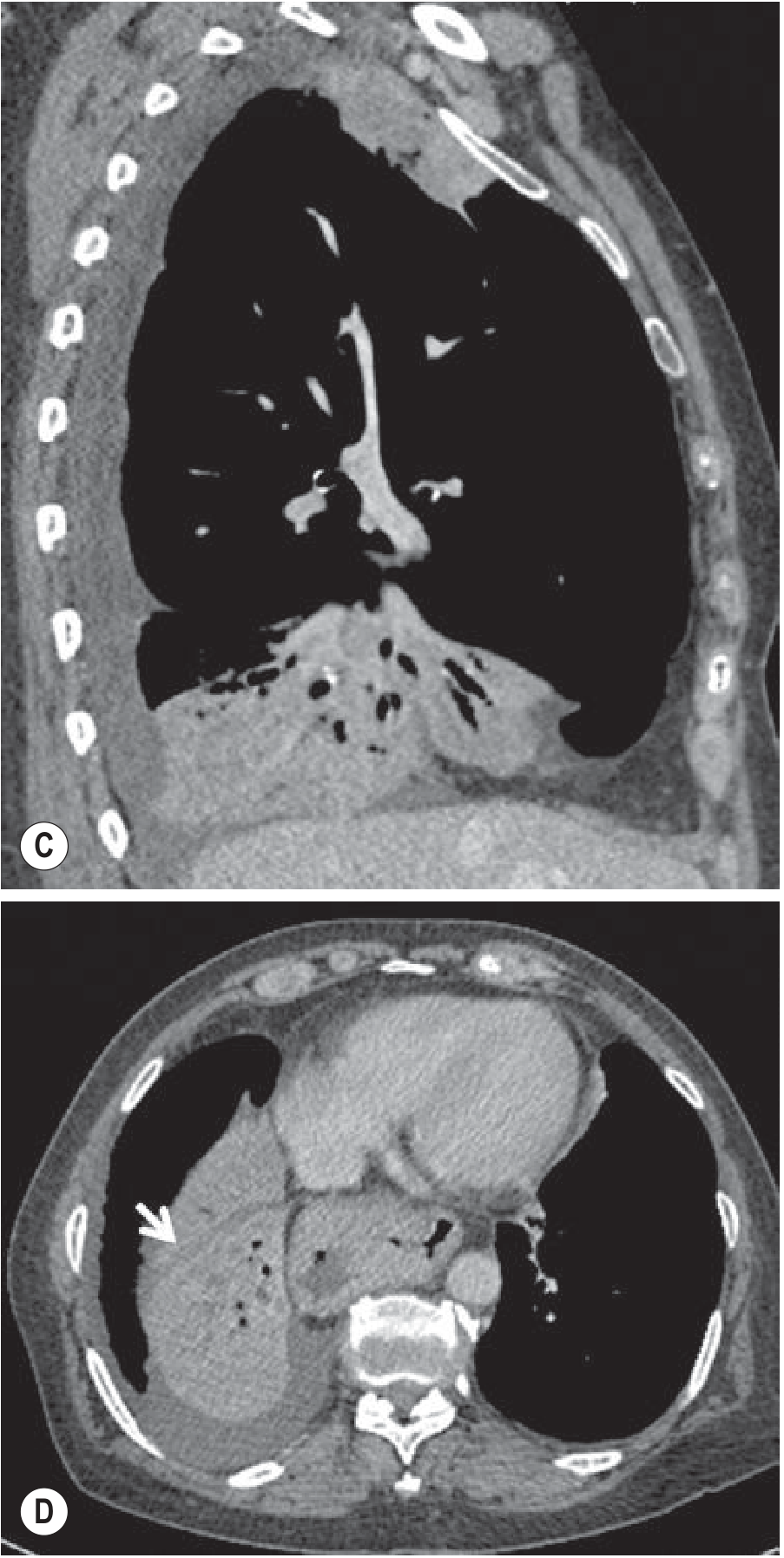
5. Combined Lobar Collapses
Right Middle + Right Lower Lobe Collapse
- Due to obstruction at the bronchus intermedius
- On frontal view: opacity extends to the right costophrenic angle
- On lateral view: opacity extends from front to back of the hemithorax
Combined RML + RLL X-ray and CT
Right Upper + Right Middle Lobe Collapse
- Less common - RUL and RML don't share a common bronchial origin
- Usually from carcinoma obstructing one bronchus + extrinsically compressing the other
- Appearance mimics left upper lobe collapse on both frontal and lateral radiographs
Causes of Lobar Collapse (Summary)
| Category | Causes |
|---|---|
| Intrinsic endobronchial | Bronchogenic carcinoma (most common in adults), carcinoid, metastases (breast, renal, colon), lymphoma, mucous plugs, foreign bodies, granulomatous disease |
| Extrinsic compression | Hilar/mediastinal lymphadenopathy, mediastinal masses, fibrosing mediastinitis, aortic aneurysm |
| Non-obstructive | Pleural effusion, pneumothorax, post-operative, surfactant loss |
In a middle-aged or elderly smoker, lobar collapse should be considered due to bronchogenic carcinoma until proven otherwise.
CT vs X-ray: Advantages of CT
- No superimposition of structures
- Multiplanar reformats (coronal, sagittal, axial)
- Identifies the cause of collapse (e.g., endobronchial mass, mucous plug)
- Differentiates collapsed lung from pleural effusion
- Air bronchograms visible on CT even when absent on X-ray
- PET/CT can delineate tumour from post-obstructive collapse - useful for biopsy targeting and radiotherapy planning
Quick Reference Table
| Lobe | Direction of Collapse | Key X-ray Sign | Silhouette Sign |
|---|---|---|---|
| RUL | Superior + medial | Elevated horizontal fissure, concave inferior border | Right superior mediastinum |
| LUL | Anterior + medial | Veil-like opacity, Luftsichel sign | Left heart border, aortic knuckle |
| RML | Inferior + medial | Subtle; triangular density on lateral | Right heart border |
| RLL | Posterior + medial | Triangular density behind heart | Right hemidiaphragm (medial) |
| LLL | Posterior + medial | Triangular density behind heart | Left hemidiaphragm (medial) |
Grainger & Allison's Diagnostic Radiology, 7th edition, Chapter 7 - Lobar Collapse
This is a shared conversation. Sign in to Orris to start your own chat.