Management of migraine
Reading File
Finding Sources
Finding Sources
Searching PubMed
"migraine" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Management of Migraine
Migraine management is divided into two broad strategies: acute (abortive) treatment of individual attacks and preventive (prophylactic) treatment to reduce attack frequency and severity. Non-pharmacological measures apply to both.
Overview of Attack Phases & Treatment Targets
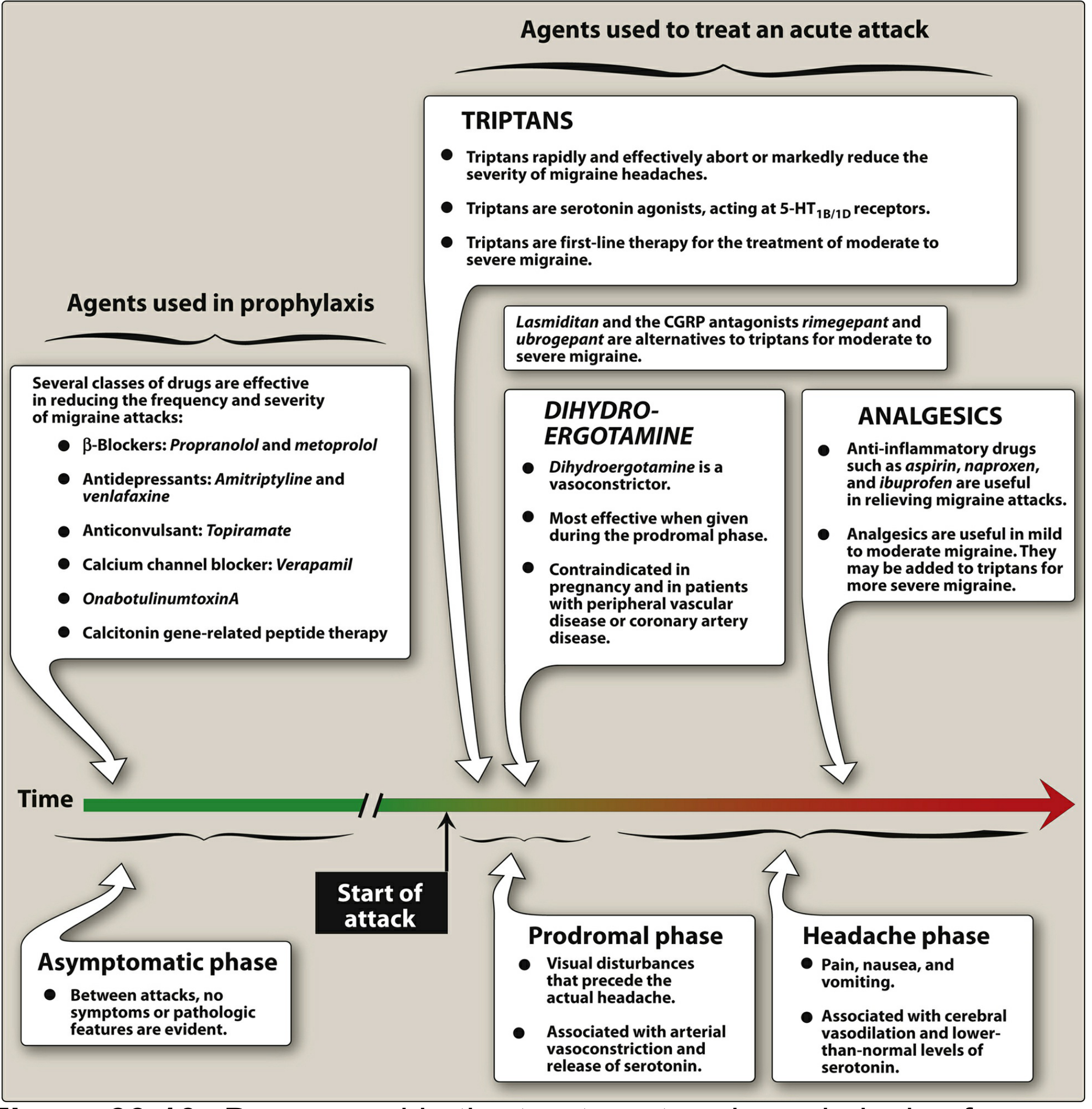
Lippincott Illustrated Reviews: Pharmacology - Figure 39.10. Agents deployed across migraine phases.
1. General Principles
- Begin acute treatment early - ideally at the visual prodrome or at the very onset of headache. Delayed treatment reduces efficacy of nearly all drug classes. - Adams and Victor's Principles of Neurology, 12th Ed.
- Assess disability using the MIDAS score (Migraine Disability Assessment Score):
- Grade I (0-5): minimal disability
- Grade II (6-10): mild disability
- Grade III (11-20): moderate disability
- Grade IV (>20): severe disability - Harrison's Principles of Internal Medicine, 22nd Ed.
- Patient education is an integral part of management: lifestyle triggers (sleep disruption, stress, fasting, alcohol, hormonal fluctuations), and the understanding that migraine can be controlled but not cured. - Harrison's
2. Acute (Abortive) Treatment
A. Mild-to-Moderate Attacks - Non-specific Analgesics (First-Line)
| Drug | Dose | Notes |
|---|---|---|
| Aspirin / Ibuprofen / Naproxen | e.g., Ibuprofen 400 mg PO q3-4h; Naproxen 220-550 mg bid | First-line for mild attacks |
| Acetaminophen + Aspirin + Caffeine | Two tablets q6h (max 8/day) | Combination (e.g., Excedrin Migraine) |
| Diclofenac K | 50 mg PO with water | - |
- NSAIDs are first-line for mild attacks. Trying 2-3 different NSAIDs across successive attacks is reasonable since response varies. Caution: risk of medication overuse headache (MOH) with frequent use. - Adams and Victor's
- Antiemetics (e.g., metoclopramide 10 mg IV, prochlorperazine 5-10 mg IV/PR) address nausea/vomiting and have independent analgesic properties in migraine. - Tintinalli's Emergency Medicine
B. Moderate-to-Severe Attacks - Migraine-Specific Therapy
Triptans (5-HT1B/1D Receptor Agonists) - First-Line for Moderate/Severe
Sumatriptan was the prototype; triptans abort or markedly reduce migraine in ~70% of patients. They act at 5-HT1B/1D receptors on trigeminal nerve terminals and intracranial vessels, causing vasoconstriction and inhibiting release of pro-inflammatory neuropeptides (including CGRP). - Lippincott Pharmacology
| Triptan | Route | Dose |
|---|---|---|
| Sumatriptan | Subcutaneous | 6 mg SC (onset ~20 min) |
| Sumatriptan | Oral | 50-100 mg |
| Sumatriptan | Intranasal | 20 mg/spray |
| Zolmitriptan | Oral / Nasal | 2.5-5 mg |
| Rizatriptan | Oral | 5-10 mg; repeat in 2 h if needed |
| Naratriptan | Oral | 2.5 mg |
| Frovatriptan | Oral | 2.5 mg (longest t½ >24 h - useful for menstrual migraine) |
| Almotriptan | Oral | 12.5 mg |
| Eletriptan | Oral | 40-80 mg |
- SC triptans should not be given during the aura (ineffective for prevention); give at onset of headache. Oral/nasal formulations should be given as early as possible, even during the aura. - Adams and Victor's
- If one triptan fails, trying a different agent or a different route is worthwhile.
- Contraindications: ischemic heart disease, uncontrolled hypertension, hemiplegic or basilar migraine, pregnancy (category C). Cardiac evaluation required before use in patients with CAD risk factors. - Tintinalli's; Lippincott
Ergot Alkaloids
- Ergotamine tartrate 1-2 mg sublingual: alpha-adrenergic + 5-HT1 agonist + dopamine receptor activity. Most effective early in attack. Strict dose limits due to rebound headache and dependence potential. - Lippincott
- Dihydroergotamine (DHE): Available IV (1 mg IV over 3 min) or intranasal (Migranal). Efficacy similar to sumatriptan. Pretreat with an antiemetic. Contraindicated in pregnancy (category X), basilar/hemiplegic migraine, uncontrolled hypertension, ischemic heart disease, within 24 h of triptan use. - Tintinalli's
Ditans (5-HT1F Receptor Agonists)
- Lasmiditan: Acts exclusively at neural targets (5-HT1F), no vasoconstriction. An alternative to triptans for patients with cardiovascular contraindications. - Harrison's; Lippincott
CGRP Receptor Antagonists (Gepants) - Acute Use
CGRP (calcitonin gene-related peptide) is a key vasoactive neuropeptide released from trigeminal terminals during migraine. Gepants block its receptor. - Harrison's
- Ubrogepant (oral): approved for acute migraine
- Rimegepant (oral): approved for both acute and preventive use
Common adverse effects: nausea and somnolence. - Lippincott
C. Emergency / Rescue Treatment (ED Setting)
(From Tintinalli's Emergency Medicine)
| Drug | IV/IM Dose | Notes |
|---|---|---|
| Ketorolac | 10-30 mg IV/IM | NSAID - equivalent analgesic effect across doses |
| Prochlorperazine | 5-10 mg IV/PR | Antiemetic + analgesic; give diphenhydramine concurrently |
| Metoclopramide | 10 mg IV | Antiemetic; give diphenhydramine concurrently |
| Droperidol | 2.5 mg IV/IM | Monitor QTc |
| Chlorpromazine | 7.5 mg IV | Pretreat with NS bolus (hypotension risk) |
| Magnesium sulfate | 2 g IV over 30 min | Non-validated; useful in migraine with aura |
| Dexamethasone | 6-10 mg IV | Adjunctive; reduces recurrence |
| Methylprednisolone | 125 mg IV/IM | Rescue therapy |
| Valproate | 500 mg IV | Avoid in pregnancy (category X) |
| Sumatriptan | 6 mg SC | - |
| DHE | 1 mg IV over 3 min | Pretreat with antiemetic |
3. Preventive (Prophylactic) Treatment
Indications for prevention:
- Attacks ≥2 per month
- Severe, prolonged, or disabling attacks (high MIDAS score)
- Attacks complicated by neurologic signs
- Overuse or failure of acute therapies
- Special forms: hemiplegic migraine, migraine with prolonged aura
Drug Classes for Prophylaxis
| Class | Drug(s) | Notes |
|---|---|---|
| Beta-blockers (first-line) | Propranolol, Metoprolol | Drugs of choice |
| Anticonvulsants | Topiramate, Divalproex (sodium valproate) | Effective; divalproex contraindicated in pregnancy |
| Antidepressants | Amitriptyline, Venlafaxine | Especially useful if comorbid depression/anxiety |
| Calcium channel blockers | Verapamil | Particularly useful in cluster overlap |
| OnabotulinumtoxinA | Botox | Approved for chronic migraine (≥15 headache days/month) |
| CGRP monoclonal antibodies | Erenumab (anti-CGRP receptor), Galcanezumab, Fremanezumab, Eptinezumab (anti-CGRP) | Subcutaneous; effective with good tolerability; expensive. Monthly or quarterly dosing |
| Oral gepants | Rimegepant, Atogepant | Oral CGRP antagonists approved for prevention |
- Lippincott; Katzung's; Bradley and Daroff's Neurology
Key points on prophylaxis:
- Beta-blockers (propranolol) are the first-choice drugs. - Lippincott
- CGRP monoclonal antibodies (erenumab, galcanezumab, fremanezumab, eptinezumab) are effective and well-tolerated but expensive and given SC. All four have been studied in chronic migraine with favorable results. Cardiovascular monitoring is warranted given CGRP's cardioprotective role. - Katzung's; Bradley and Daroff's
- A second PACAP monoclonal antibody showed efficacy in a phase 2 study. - Harrison's
- Any prophylactic agent should be given an adequate trial (2-3 months) before judging failure.
Menstrual Migraine
Frovatriptan (longest-acting triptan, t½ >24 h) is preferred for perimenstrual prophylaxis given its prolonged duration of action. Naratriptan is an alternative. - Bradley and Daroff's Neurology
4. Non-Pharmacological Measures
- Identify and avoid triggers: sleep irregularity, fasting, stress, alcohol (especially red wine), bright or flickering lights, strong odors, estrogen fluctuations.
- Lifestyle regularity: consistent sleep, meals, hydration, and exercise.
- Biofeedback and cognitive behavioral therapy (CBT): evidence-based adjuncts for prevention.
- Patient education about the nature of migraine and its management. - Harrison's
5. Pathophysiological Basis (Context for Drug Selection)
Migraine involves trigeminovascular activation - cells in the trigeminal nucleus release CGRP and PACAP at vascular terminals, causing vasodilation and neuroinflammation. Triptans reverse this by cranial vasoconstriction and inhibiting neuropeptide release. Ditans and gepants act via neural CGRP/5-HT1F mechanisms without vasoconstriction, making them safer in cardiovascular disease. Brainstem (dorsal raphe, locus coeruleus) and hypothalamic modulation also play a role - explaining the prodromal symptoms (yawning, food cravings, mood change) and the efficacy of dopamine-blocking antiemetics. - Harrison's
6. Recent Evidence Update
A 2024 network meta-analysis in the BMJ (PMID 39293828) compared drug interventions for acute migraine management across 53 trials and found differences in efficacy between agents; triptans and gepants both performed well. A 2025/2026 American Headache Society guideline update (PMID 41321235) updated evidence assessment for parenteral pharmacotherapies in the ED setting, reinforcing the role of dopamine antagonists and DHE.
Sources: Adams and Victor's Principles of Neurology, 12th Ed. | Harrison's Principles of Internal Medicine, 22nd Ed. | Lippincott Illustrated Reviews: Pharmacology | Katzung's Basic and Clinical Pharmacology, 16th Ed. | Tintinalli's Emergency Medicine | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.