MCA stroke
Reading File
Finding Sources
Finding Sources
Searching PubMed
"middle cerebral artery" AND "ischemic stroke"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information to write a detailed, well-organized answer. Here it is:
Middle Cerebral Artery (MCA) Stroke
Anatomy & Territory
The MCA is the most common vessel involved in stroke. Its main trunk (M1 segment) arises from the internal carotid artery and divides into two main divisions (M2 segments) - superior and inferior - within the Sylvian fissure. Some patients have a trifurcation.
Cortical supply (via superficial branches):
- Lateral frontal lobe - motor areas 4 and 6, Broca's area (dominant hemisphere), frontal eye fields
- Parietal lobe - primary sensory cortex, supramarginal and angular gyri
- Superior temporal lobe and insula - Wernicke's area (dominant hemisphere)
Deep supply (via lenticulostriate/penetrating branches):
- Putamen, head and body of caudate nucleus
- Posterior limb of internal capsule
- Outer globus pallidus
- Deep white matter / corona radiata
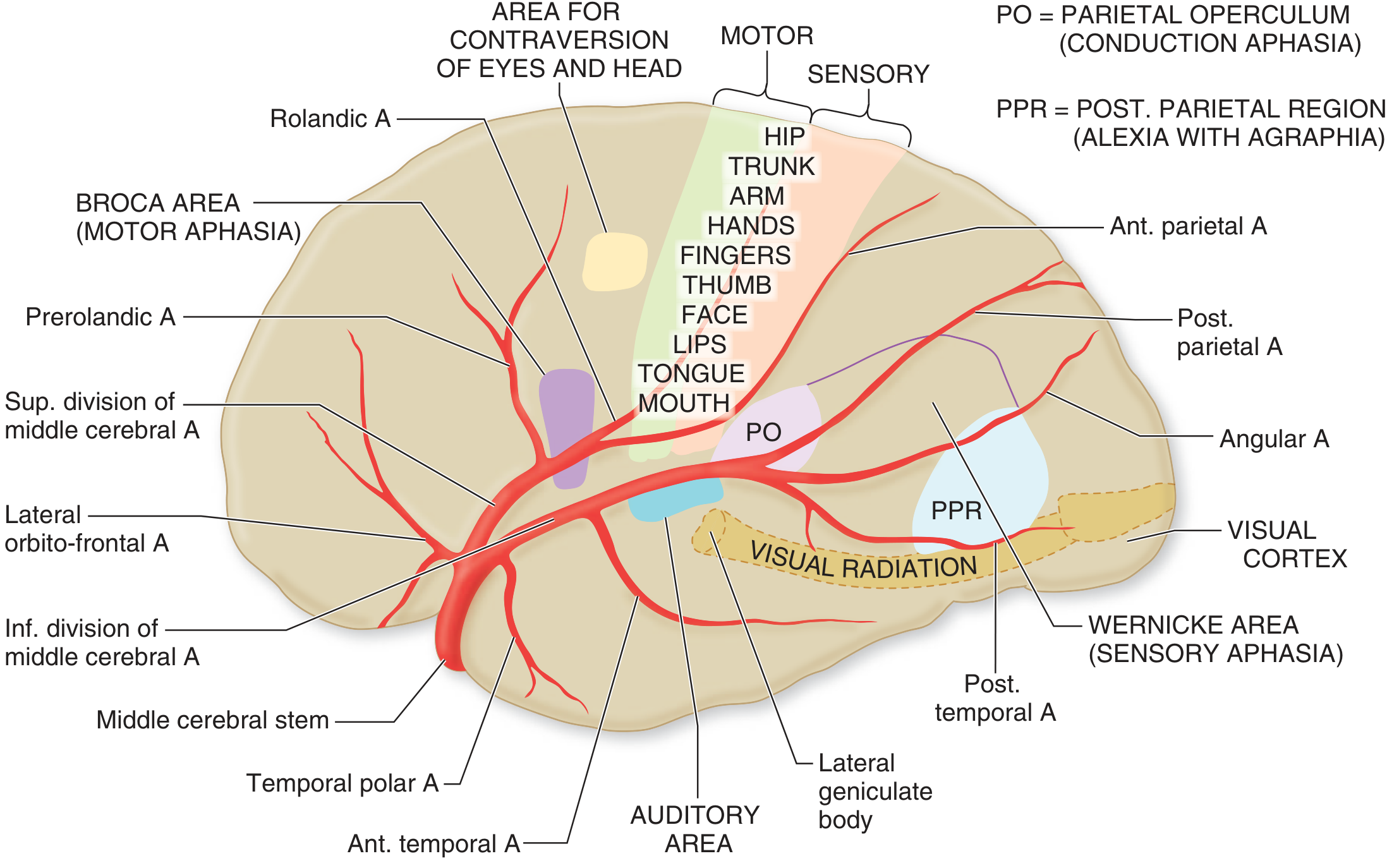
MCA territory - lateral view showing superior and inferior divisions, Broca's area, Wernicke's area, motor/sensory cortex, and visual radiation (Adams & Victor's Principles of Neurology, 12th Ed.)
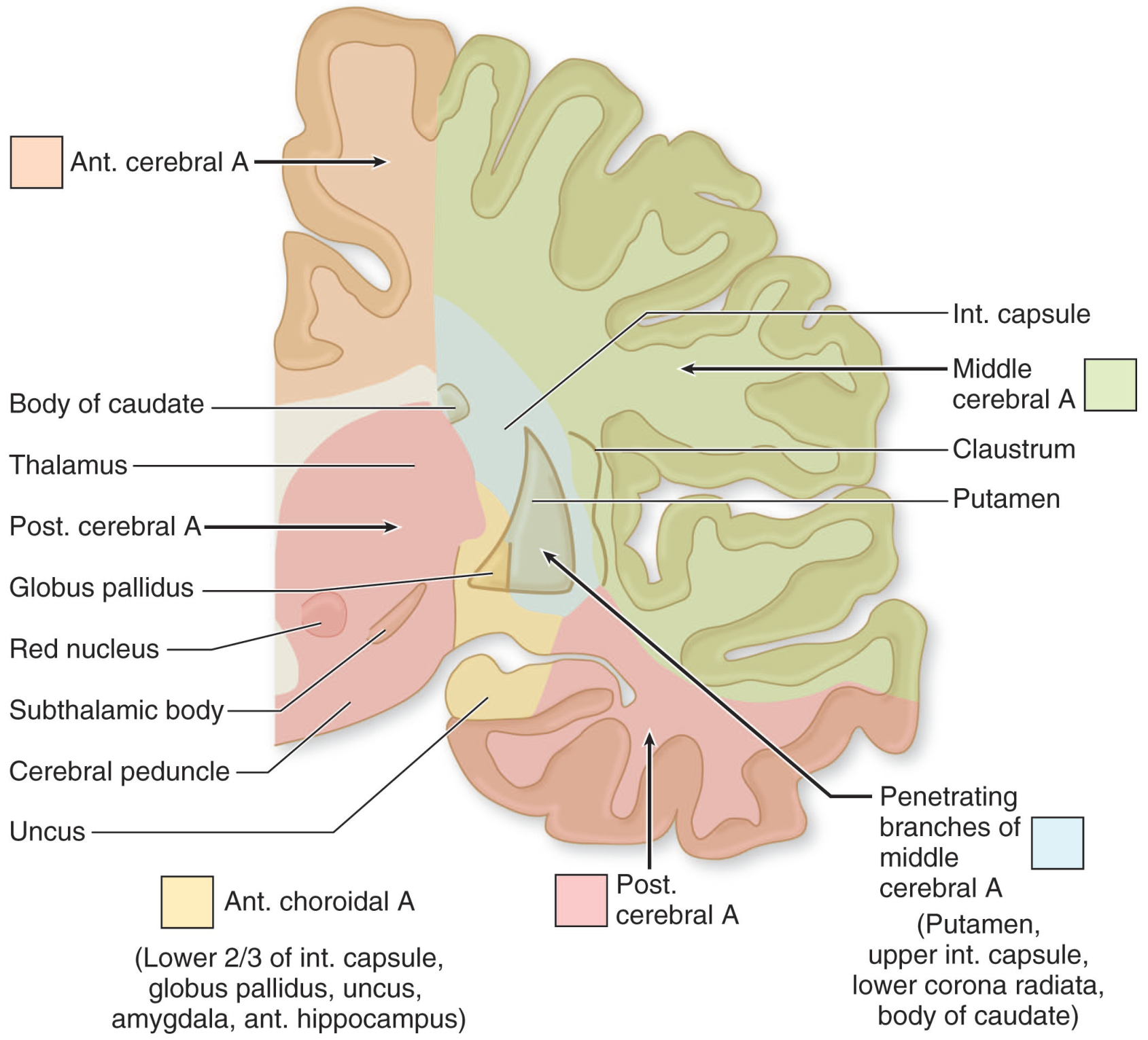
Coronal section: MCA deep territory (green) includes the internal capsule, putamen, caudate, and corona radiata (Adams & Victor's, 12th Ed.)
Clinical Syndromes by Territory
MCA Stem (M1) Occlusion - Most Severe
Total M1 occlusion produces a combination of all elements below:
| Feature | Mechanism |
|---|---|
| Contralateral hemiplegia (face + arm + leg) | Posterior limb of internal capsule infarction |
| Contralateral hemianesthesia | Sensory cortex + thalamic radiations |
| Homonymous hemianopia | Lateral geniculate body / optic radiations |
| Ipsilateral head and eye deviation | Damage to frontal eye fields (drives eyes toward lesion) |
| Global aphasia (left hemisphere) | Combined Broca + Wernicke damage |
| Anosognosia + hemineglect (right hemisphere) | Non-dominant parietal involvement |
| Initial drowsiness | Widespread neuronal dysfunction |
Cause: Almost always embolic (Fisher, 1975; Caplan, 1989). Atherosclerotic thrombosis is less common but more prevalent in Asian populations (with diabetes and hypertension as key risk factors).
MCA Branch Occlusions (Partial Syndromes)
| Location | Deficits |
|---|---|
| Left MCA superior division | Right face + arm weakness (UMN type), Broca's (non-fluent) aphasia; may have right arm cortical sensory loss; leg relatively spared |
| Left MCA inferior division | Wernicke's (fluent) aphasia + right visual field deficit; motor findings usually absent; patient may appear confused or psychotic |
| Right MCA superior division | Left face + arm weakness (UMN type), left hemineglect (variable) |
| Right MCA inferior division | Profound left hemineglect, left visual and somatosensory deficits; motor findings often absent or subtle |
| Left MCA deep territory | Right pure motor hemiparesis (UMN); larger infarcts may produce aphasia as well |
| Right MCA deep territory | Left pure motor hemiparesis; larger infarcts may produce hemineglect |
Key clinical pearls:
- Face and arm > leg in MCA strokes (leg spared because ACA territory supplies the leg motor strip)
- Dominant hemisphere (left) occlusion: aphasia is the hallmark language finding
- Non-dominant hemisphere (right) occlusion: neglect, anosognosia, constructional apraxia, dysarthria without aphasia
Deep MCA Infarcts (Striatocapsular)
Infarction of lenticulostriate territory produces larger-than-lacunar but smaller-than-cortical syndromes. The most common pattern: partial hemiparesis + limited Broca-type aphasia (often short-lived) or hemineglect. These are typically embolic (M1 embolus lodges and then moves distally, leaving deep structures infarcted with a patent MCA on imaging).
Etiology
- Embolism (cardiac sources: atrial fibrillation, valvular disease, low EF; or artery-to-artery from ICA plaque) - the dominant cause
- In situ atherosclerosis - more common in Asian, diabetic, hypertensive patients
- Lacunar / small vessel disease - affects only penetrating branches
- Hypercoagulable states - protein C/S deficiency, Factor V Leiden, antiphospholipid syndrome, malignancy, sickle cell
Risk factors: hypertension, diabetes, hypercholesterolemia, smoking, obesity, atrial fibrillation, prior stroke/TIA.
Workup
Immediate:
- Non-contrast head CT - performed within 20 minutes of arrival to exclude hemorrhage before giving thrombolytics
- CT Angiography (CTA) - identifies large vessel occlusion (LVO) at M1/M2
- CT Perfusion or MRI DWI/PWI - identifies ischemic core vs. salvageable penumbra; guides thrombectomy eligibility
- Blood: CBC, BMP, coagulation (PT/INR/aPTT), glucose, type and screen
- ECG (detect AFib), cardiac monitoring, echocardiography (TTE/TEE)
- NIHSS score - standard neurological severity assessment
Diagnostic workup for etiology:
- 24-72 hour cardiac monitoring (paroxysmal AFib)
- Carotid duplex / MRA for ICA stenosis
- Hypercoagulability panel if indicated (young patient, no clear cause)
Acute Management
Reperfusion Therapies
1. IV Alteplase (tPA)
- Indicated within 4.5 hours of symptom onset (earlier = better outcomes)
- Dose: 0.9 mg/kg IV (max 90 mg), 10% as bolus, rest over 60 minutes
- Key contraindications: hemorrhage on CT, BP >185/110 mmHg (uncontrolled), active bleeding, recent major surgery (<2 weeks), platelets <100,000, INR >1.7
- IV tenecteplase has been compared favorably to alteplase and is an emerging alternative
- Time pressure is paramount: "door-to-needle" <30 minutes strongly reduces disability at 3 months
2. Endovascular Mechanical Thrombectomy (MT)
- Indicated for large vessel occlusion (ICA, M1, proximal M2) with significant NIHSS deficits
- Time window: up to 6 hours from onset (selected patients to 24 hours with favorable perfusion imaging)
- MR-CLEAN (2015) and 4 concurrent trials (ESCAPE, SWIFT PRIME, EXTEND-IA, REVASCAT) demonstrated dramatically superior 90-day outcomes - trials terminated early for benefit
- tPA remains the standard first-line therapy even in those who will undergo MT (bridging therapy)
- Advantages over tPA: fewer exclusion criteria, works for large clot burden, effective where tPA achieves <20% recanalization
A 2025 meta-analysis of RCTs (Lin et al., PMID 40245084) confirmed benefit of thrombectomy even in patients with large ischemic cores, expanding the eligible population.
General Supportive Care
- BP management: Permissive hypertension (allow up to 220/120 mmHg pre-thrombolysis; maintain <185/110 for tPA candidates). For those not receiving reperfusion, target systolic <220 mmHg unless hypertensive emergency. Post-thrombectomy or tPA: target <180 mmHg.
- IV fluids: Normal saline (isotonic), no glucose-containing solutions (glucose worsens ischemic injury via osmotic shifts)
- Normovolemia, normothermia, normoglycemia
- Admit to dedicated stroke unit / ICU; frequent neurological checks
- Aspirin 325 mg within 24-48 hours (if no thrombolytics given) for antiplatelet effect
Malignant MCA Syndrome
Large MCA territory infarctions (typically >50% of MCA territory) cause massive cerebral edema, typically peaking at 3-5 days post-stroke. This can cause:
- Midline shift
- Transtentorial herniation
- Death or severe disability
Decompressive hemicraniectomy is a life-saving option in selected patients (younger age, dominant-hemisphere involvement controversial). Studies show favorable mortality reduction, though functional outcome is still poor in many (less than half return home after rehabilitation). Shared decision-making with family regarding quality of life expectations is essential.
Secondary Prevention
| Category | Intervention |
|---|---|
| Non-cardioembolic stroke | Antiplatelet therapy (aspirin, clopidogrel, or aspirin+dipyridamole) |
| Cardioembolic (AFib) | Anticoagulation (DOACs preferred over warfarin) |
| ICA stenosis >70% | Carotid endarterectomy (CEA) or stenting |
| Intracranial atherosclerosis | Aggressive medical management (aspirin, statins, BP control); angioplasty/stenting in refractory cases |
| All patients | Statin therapy, BP control (<130/80), lifestyle modification |
Summary
The MCA supplies the largest portion of the cerebral hemisphere. Its occlusion at different levels produces predictable but variable deficits - from global aphasia + hemiplegia in M1 occlusion, to isolated fluent aphasia with inferior division occlusion, to pure motor deficits with deep territory involvement. Time-sensitive reperfusion with IV tPA and/or mechanical thrombectomy is the cornerstone of acute treatment. Malignant MCA stroke may require hemicraniectomy. Long-term management targets the underlying etiology (AFib, atherosclerosis, hypercoagulability).
Sources: Adams & Victor's Principles of Neurology 12th Ed., Neuroanatomy Through Clinical Cases 3rd Ed., Tintinalli's Emergency Medicine, Schwartz's Principles of Surgery 11th Ed. | PMID 40245084 (2025 meta-analysis, thrombectomy in large ischemic core)
This is a shared conversation. Sign in to Orris to start your own chat.