Latest guidelines for management of hypertension in pregnancy
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "pregnancy" AND "management"
Searching the Web
hypertension in pregnancy management guidelines 2024 2025 ACOG ISSHP
Reading File
Reading File
Searching PubMed
"hypertensive disorders" AND "pregnancy" AND "treatment"
Reading File
Reading File
Reading Article
PMID: 40216176
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
I now have everything needed for a comprehensive, well-structured response.
Management of Hypertension in Pregnancy — Current Guidelines
Classification
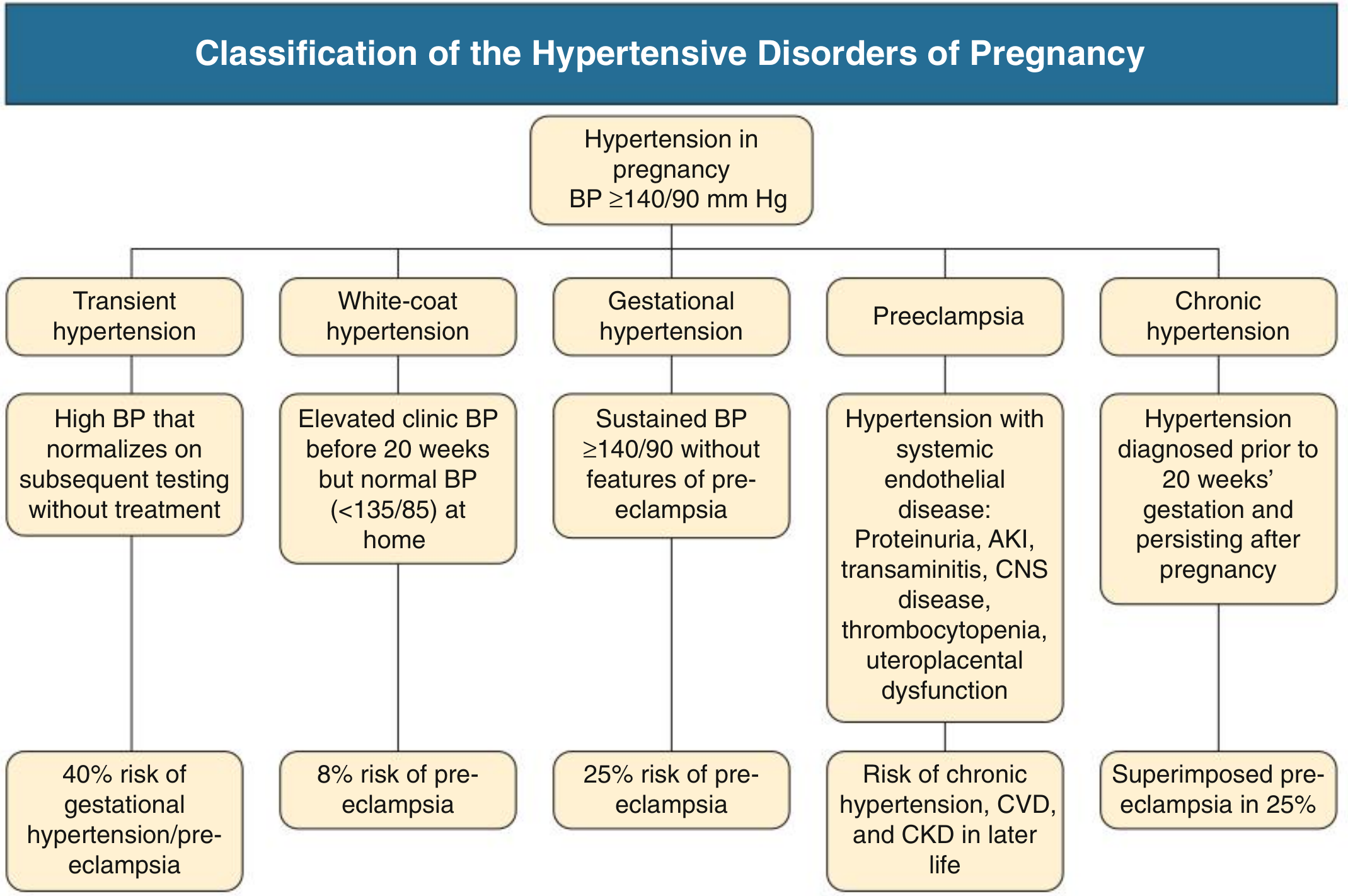
Comprehensive Clinical Nephrology, 7th Ed., Fig. 44.3
Hypertension affects 10–12% of all pregnancies. The diagnostic threshold is BP ≥140/90 mmHg. Four main disorders are recognised:
| Disorder | Definition | Key Risk |
|---|---|---|
| Gestational hypertension | New HTN after 20 weeks, no features of preeclampsia | 25% progress to preeclampsia |
| Preeclampsia | HTN after 20 weeks + organ/uteroplacental dysfunction | Stroke, HELLP, eclampsia |
| Chronic hypertension | HTN before 20 weeks or pre-existing, persists >12 wks postpartum | Superimposed preeclampsia in 25% |
| White-coat HTN | Clinic BP ≥140/90, home BP <135/85 | 8% preeclampsia risk — not benign |
Preeclampsia diagnosis does not require proteinuria if other features exist: AKI, thrombocytopenia, elevated transaminases, CNS symptoms, uteroplacental dysfunction, or fetal growth restriction. — Comprehensive Clinical Nephrology, 7th Ed.
1. Blood Pressure Targets
- Severe HTN (SBP ≥160 or DBP ≥105 mmHg): treat immediately — risk of maternal stroke is high.
- Mild-to-moderate HTN: The landmark CHIPS trial (Control of Hypertension in Pregnancy Study) showed that treating to a tight target (DBP 85 mmHg) vs. less-tight (DBP 100 mmHg) significantly reduced maternal complications (severe HTN, thrombocytopenia, transaminitis) with no significant difference in pregnancy loss, neonatal outcomes, or small-for-gestational-age rates.
- Clinical trials have failed to demonstrate benefit of targets <130/80 mmHg vs. <140/90 mmHg. — Harrison's 22E; Brenner & Rector's The Kidney
- ACOG previously recommended against antihypertensive treatment for BP <160/105 in the absence of end-organ damage, though this has evolved with CHIPS data toward treating to DBP ≤85 mmHg.
2. Antihypertensive Drug Choice
Oral First-Line Agents
| Drug | Mechanism | Advantage | Caution |
|---|---|---|---|
| Methyldopa | Central α2-agonist | Most extensive long-term safety data in offspring | Multiple daily dosing; rarely used outside pregnancy |
| Labetalol | α/β-blocker | Theoretical benefit on uteroplacental flow via α-blockade; good safety record | Avoid in reactive airway disease |
| Long-acting nifedipine | CCB (dihydropyridine) | Once-daily dosing (slow-release) | Peripheral edema |
Brenner & Rector's The Kidney, Table 48.6; Harrison's 22E
A 2025 network meta-analysis (Hup et al., AJOG, PMID 40216176) of 23 RCTs (3,989 women) found that compared to placebo, labetalol and methyldopa both significantly reduced severe hypertension (RR 0.20 and 0.44 respectively). Head-to-head, labetalol showed a modest advantage over nifedipine in reducing preeclampsia (RR 0.50) and preterm birth (RR 0.68), though overall study quality was low-to-moderate.
IV Agents for Acute/Severe Hypertension
| Drug | Notes |
|---|---|
| IV Labetalol | First choice; good safety data |
| IV Nicardipine | Extensive data as tocolytic; effective antihypertensive |
| Hydralazine | Extensive clinical experience but increased risk of maternal hypotension and placental abruption — now considered second-line |
Second-Line Oral Agents
- Metoprolol (long-acting formulation; less data than labetalol)
- Verapamil, diltiazem (no evidence of adverse fetal effects; limited data)
- Hydrochlorothiazide (used as second-line in some centres)
Drugs to Avoid
| Drug | Reason |
|---|---|
| ACE inhibitors / ARBs | Teratogenic — renal dysgenesis, oligohydramnios, neonatal renal failure |
| Atenolol | Associated with IUGR |
| Diuretics | May impair pregnancy-associated plasma volume expansion |
| Spironolactone | Theoretical risk of inadequate male fetal virilisation |
3. Preeclampsia Prevention
- Low-dose aspirin (60–150 mg/day), started after 12 weeks' gestation, is recommended for women at elevated risk of preeclampsia (prior history, chronic HTN, diabetes, renal disease, multifetal pregnancy, nulliparity with risk factors). — Fuster & Hurst's The Heart, 15th Ed.
- Calcium supplementation reduces risk in women with low dietary calcium intake (Cochrane evidence).
- Screening for secondary causes (renal artery stenosis, phaeochromocytoma, primary hyperaldosteronism, OSA) is warranted in chronic hypertension — at least 10% have secondary causes, and outcomes are worse if unrecognised.
4. Management of Preeclampsia With Severe Features
Seizure Prophylaxis
Magnesium sulfate is the treatment of choice for seizure prophylaxis in preeclampsia with severe features, and for treatment of eclampsia. It is given routinely intrapartum and for 24–48 hours postpartum. Phenytoin is less effective and is reserved for cases where magnesium is contraindicated. — Creasy & Resnik's Maternal-Fetal Medicine
Definitive Treatment: Delivery
Delivery is the only cure. Indications for urgent delivery include:
- Severe HTN refractory to treatment
- AKI / oliguria
- HELLP syndrome
- Pulmonary oedema
- Eclampsia
- Non-reassuring fetal status
For preeclampsia without severe features, delivery is generally recommended at 37 weeks.
HELLP Syndrome
HELLP (Haemolysis, Elevated Liver enzymes, Low Platelets) is a severe manifestation. AKI occurs in 10–25% of HELLP cases — urgent delivery is indicated.
5. Postpartum Management
- Hypertension commonly persists or worsens in the first 48–72 hours postpartum.
- Methyldopa, labetalol, and nifedipine are all compatible with breastfeeding.
- Magnesium sulfate prophylaxis is continued postpartum in severe preeclampsia (typically 24 hours).
- If HTN persists beyond 12 weeks postpartum, diagnose chronic hypertension.
- Women with a history of preeclampsia carry elevated long-term risk of chronic HTN, CVD, and CKD — cardiovascular risk assessment at follow-up is essential.
6. Secondary Hypertension in Pregnancy
Consider secondary causes (present in ≥10% of chronic HTN in pregnancy) when:
- Hypertension is severe or resistant
- Hypokalemia is present (primary hyperaldosteronism — note: eplerenone preferred over spironolactone in pregnancy)
- Symptoms suggest phaeochromocytoma (paroxysmal HTN, palpitations, sweating)
- OSA is suspected (screen in obese women who snore)
MR angiography is the imaging modality of choice when renal artery stenosis is suspected (CT avoided due to radiation).
Summary of Key Threshold Recommendations
| Situation | BP Threshold | Action |
|---|---|---|
| Chronic HTN, no end-organ damage | <160/105 | Treat to DBP ≤85 mmHg (CHIPS) |
| Severe HTN (any cause) | ≥160/105 | Immediate IV/oral treatment |
| Preeclampsia with severe features | Any | Magnesium + delivery planning |
| Postpartum severe HTN | ≥160/110 | Treat immediately; watch for eclampsia up to 6 wks |
Sources: Brenner & Rector's The Kidney (2-Vol. Set) · Comprehensive Clinical Nephrology, 7th Ed. · Harrison's Principles of Internal Medicine, 22E (2025) · Creasy & Resnik's Maternal-Fetal Medicine · Fuster & Hurst's The Heart, 15th Ed. · Hup et al. 2025 network meta-analysis [PMID 40216176]
Detailed info about Chips trial
Searching PubMed
"CHIPS trial" OR "Control of Hypertension in Pregnancy Study"
Finding Sources
Searching PubMed
Magee "less-tight versus tight control" hypertension pregnancy 2015
Reading File
Reading File
Reading Article
PMID: 25629739
Reading Article
PMID: 26265372
Reading Article
PMID: 26259808
Searching PubMed
Magee CHIPS hypertension pregnancy follow-up cardiovascular outcomes
Reading Article
PMID: 25629739
!
peer closed connection without sending complete message body (incomplete chunked read)
We encountered an error while processing your request. Please try again or reach out to us for help.
This is a shared conversation. Sign in to Orris to start your own chat.