Dd of suprasellar mass and hypothalamic hemartoma
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive, textbook-grounded answer covering both topics:
Differential Diagnosis of Suprasellar Mass
The suprasellar region includes the sella, suprasellar cistern, optic chiasm, hypothalamus, infundibulum, and third ventricle. The mnemonic SATCHMO (or variants) is often used to recall the key entities.
Age-Based Differential (most important organizing principle)
| Entity | Child/Young Adult | Older Adult |
|---|---|---|
| Craniopharyngioma | Most common suprasellar mass | Less common (papillary type) |
| Germ cell tumor (germinoma) | Common | Rare |
| Pilocytic astrocytoma / optic-hypothalamic glioma | Common | Rare |
| Pituitary macroadenoma | Uncommon | Most common overall |
| Rathke cleft cyst | Any age | Any age |
| Meningioma | Rare | Common |
| Colloid cyst | - | Third ventricle |
| Hypothalamic hamartoma | Children | Rare |
(Bradley and Daroff's Neurology; Table 72.1)
The Major Entities in Detail
1. Craniopharyngioma
- Most common suprasellar mass in children; bimodal peak at ages 10-14 and again in middle age
- Arises from Rathke cleft remnants; WHO Grade I
- Two histological subtypes:
- Adamantinomatous - children; cystic, calcified, "machinery oil" fluid
- Papillary - adults; solid, isointense on T1, less calcification
- MRI: mixed cystic-solid mass with suprasellar extension, rim + solid enhancement; T1 hyperintensity if protein/cholesterol-rich cyst contents; heterogeneous T2
- Calcification in >90% of adamantinomatous type on CT
- Complications post-surgery: diabetes insipidus (90%), hypothalamic obesity (~50%), panhypopituitarism
- (K.J. Lee's Essential Otolaryngology; Bradley and Daroff's)
2. Pituitary Macroadenoma (with suprasellar extension)
- Most common sellar/suprasellar mass in adults
- Microadenoma <10 mm; macroadenoma >10 mm
- 65% functional: prolactinomas (48%), GH-secreting (10%), ACTH-secreting (6%), TSH (1%)
- MRI: iso/hypointense on T1, enhancing; "snowman" shape when extending through diaphragma sellae
- Stalk effect raises prolactin (<200 ng/mL); true prolactinoma levels often >200
- Apoplexy = hemorrhagic infarction → sudden headache, visual loss, panhypopituitarism
3. Germ Cell Tumor (Germinoma)
- Peak 10-12 years; more common in Asia; >90% in under-20 age group
- Typical midline locations: suprasellar (more in girls) and pineal (more in boys)
- Synchronous pineal + suprasellar lesions = pathognomonic for germinoma
- CT: hyperdense, avid homogeneous enhancement; MRI: T2 hypointense (due to cellularity), restricted diffusion
- Cause of diabetes insipidus in young + absence of posterior pituitary bright spot
- Extremely radiosensitive
- (Grainger & Allison's Diagnostic Radiology)
4. Optic Pathway / Hypothalamic Glioma
- 10-15% of supratentorial tumors in children
- Usually pilocytic astrocytoma (WHO I) - very indolent; hypothalamic/chiasmatic involvement may be WHO II with more aggressive behavior
- Strongly associated with NF-1 (neurofibromatosis type 1)
- MRI: T1 iso/hypointense, T2 hyperintense; fusiform expansion of optic nerves; variable enhancement
- "Unidentified bright objects" in globi pallidi, thalami, midbrain = NF-1 hallmark
- Main differential from craniopharyngioma: glioma presents earlier, no calcification, no cyst with cholesterol fluid
5. Hypothalamic Hamartoma
(Covered in detail in the next section)
6. Meningioma
- Suprasellar/tuberculum sellae meningioma: adults, more common in women
- MRI: isointense to cortex T1/T2, intense homogeneous enhancement, dural tail
- May compress the optic chiasm - bitemporal hemianopia
7. Rathke Cleft Cyst
- Benign, intrasellar with variable suprasellar extension
- MRI: variable signal (T1 hypo or hyperintense depending on protein content); no solid enhancing component
- Key differentiator from craniopharyngioma: no calcification, no solid enhancing nodule
8. Arachnoid Cyst / Epidermoid
- Arachnoid cyst: follows CSF on all sequences; no diffusion restriction
- Epidermoid: follows CSF on T1/T2 but restricts on DWI - key feature
9. Infundibular/Stalk lesions (important subset)
- Langerhans cell histiocytosis (LCH): enhancement and thickening of infundibulum; diabetes insipidus in a child; correlates with absent posterior pituitary bright spot on T1
- Germinoma (as above)
- Sarcoidosis: granulomatous thickening of stalk; may involve hypothalamus
- Lymphoma/Lymphocytic hypophysitis: infundibular mass + hyperprolactinemia
10. Vascular
- Supraclinoid aneurysm (ICA, ACoA): can mimic suprasellar mass; pulsation artifact on MRI; flow void; CTA/MRA confirm
11. Granulomatous
- Tuberculoma, sarcoidosis: associated with basal meningitis, CSF changes
Hypothalamic Hamartoma - In Depth
Definition
A hamartoma (not a true neoplasm) - a benign, congenital tumor-like malformation arising from the floor of the third ventricle / hypothalamus. By definition it is a hypothalamic mass rather than a true tumour.
Two Classic Presentations
| Feature | Precocious Puberty Type | Gelastic Epilepsy Type |
|---|---|---|
| Morphology | Pedunculated (attached by stalk) | Sessile (intrahypothalamic) |
| Location | Hangs inferiorly from floor of 3rd ventricle into suprasellar / interpeduncular cistern | Embedded within hypothalamus at level of mammillary bodies |
| Age of onset | Early childhood | Early life (infancy to 2 years) |
| Seizure type | Absent or minimal | Gelastic seizures (earliest), then dacrystic, focal, generalized |
| Other features | Short stature | Cognitive and behavioral deterioration |
Seizure Characteristics
- Gelastic seizures: involuntary laughing (ictal laughter, often without mirth) - pathognomonic when arising from hypothalamic hamartoma
- The hamartoma itself is the epileptogenic zone - seizures originate within the lesion
- Other seizure types develop later: dacrystic (crying spells), focal aware/unaware, generalized tonic-clonic
- 25% of gelastic seizures are associated with hypothalamic hamartoma; 21% of patients with hypothalamic hamartoma have gelastic seizures
- Cognitive decline and behavioral disturbance are progressive
- (Bradley and Daroff's; Localization in Clinical Neurology 8e; K.J. Lee's)
MRI Features (Pathognomonic)
- Isointense to grey matter on T1 and T2 (the key distinguishing feature from other suprasellar lesions)
- No contrast enhancement (the other critical feature)
- Well-defined, round or ovoid lesion
- Sessile type: broad base attached to hypothalamus/floor of third ventricle
- Pedunculated type: stalk, projecting into the suprasellar or interpeduncular cistern
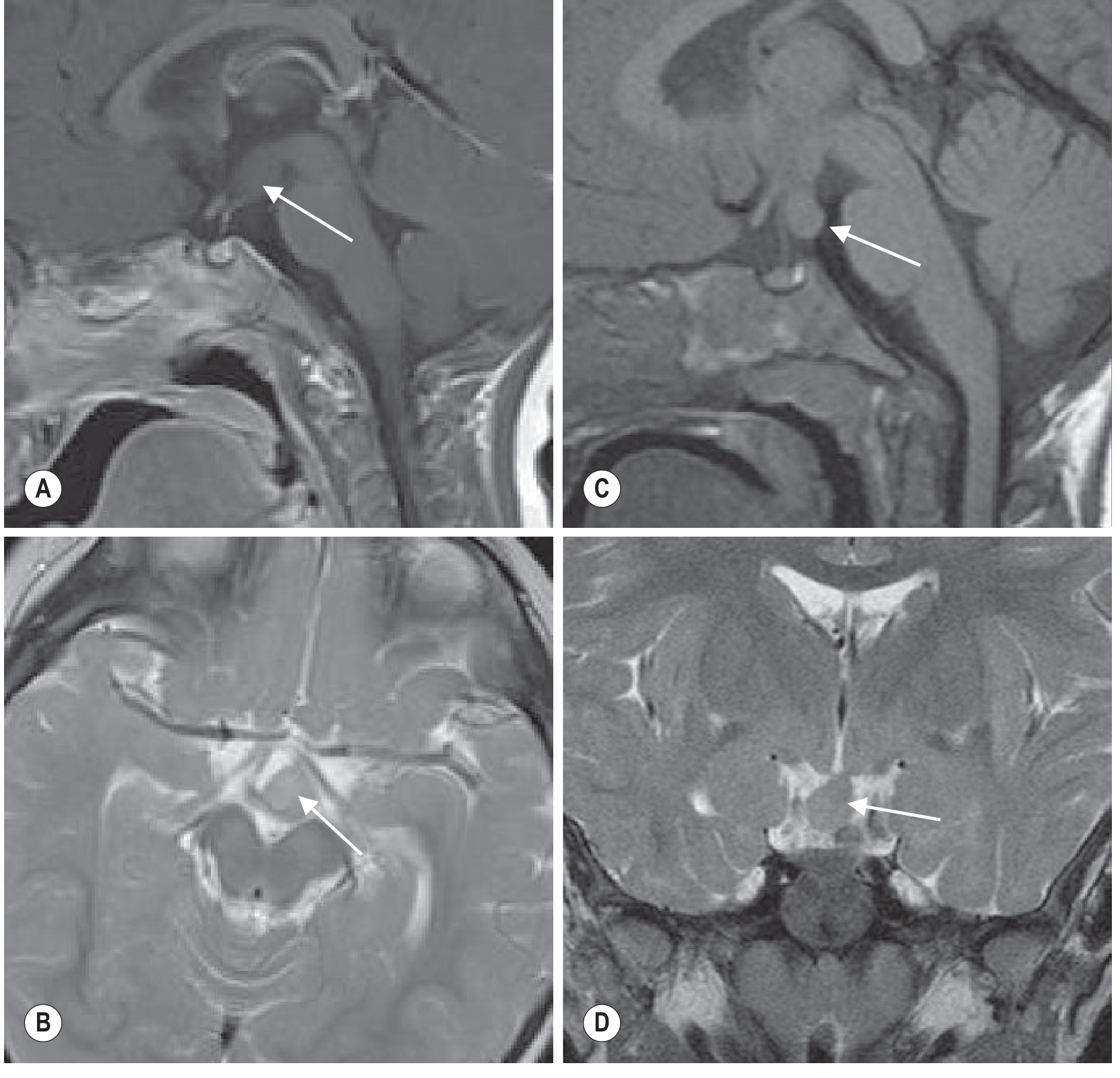
Grainger & Allison's Diagnostic Radiology - Fig. 76.65: (A) Post-contrast sagittal T1 and (B) axial T2 showing sessile hamartoma isointense to grey matter, no enhancement. (C) Sagittal T1 and (D) coronal T2 showing pedunculated hamartoma projecting from floor of third ventricle into suprasellar cistern.
Genetics
- Some cases associated with congenital anomalies and mutations in the transcription factor gene GLI3 (Goldman-Cecil Medicine)
Treatment
- Medical: Antiepileptic drugs often poorly effective for gelastic seizures
- Stereotactic radiosurgery (Gamma Knife): well established
- Surgical disconnection: transcallosal or endoscopic approaches
- Laser interstitial thermal therapy (LITT): emerging option
Key Distinguishing Features: Suprasellar Masses at a Glance
| Feature | Craniopharyngioma | Hypothalamic Hamartoma | Germinoma | Optic Glioma | Pituitary Adenoma |
|---|---|---|---|---|---|
| Calcification | Yes (adamantinomatous) | No | Rare | No | Rare |
| Enhancement | Rim + solid | None | Avid, homogeneous | Variable | Yes |
| T1 signal | Heterogeneous/hyperintense | Isointense to grey matter | Iso/hypointense | Iso/hypointense | Iso/hypointense |
| T2 signal | Hyperintense (cyst) | Isointense to grey matter | Hypointense | Hyperintense | Iso/hyperintense |
| Cystic component | Yes (classic) | No | Rare | Sometimes | Sometimes |
| DWI restriction | No | No | Yes | No | No |
| Clinical hallmark | Bitemporal hemianopia + DI | Gelastic seizures / precocious puberty | DI in child + ↑AFP/β-hCG | NF-1 association | Hormonal excess/deficit |
The isointensity to grey matter on both T1 and T2 with no enhancement is the pathognomonic MRI signature of a hypothalamic hamartoma and distinguishes it from every other suprasellar mass.
Sources: Grainger & Allison's Diagnostic Radiology; Bradley and Daroff's Neurology in Clinical Practice; Localization in Clinical Neurology 8e; K.J. Lee's Essential Otolaryngology; Goldman-Cecil Medicine; Adams and Victor's Principles of Neurology
Cerebral av malformation imaging
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
Finding Sources
I now have comprehensive content. Let me compile the complete answer:
Cerebral Arteriovenous Malformation (AVM) - Imaging
Classification of Intracranial Vascular Malformations
Intracranial vascular malformations are classified by the presence or absence of arteriovenous shunting:
| With AV Shunting | Without AV Shunting |
|---|---|
| Cerebral (subpial) AVM | Cavernous angioma (cavernoma) |
| Dural arteriovenous fistula (dAVF) | Developmental venous anomaly (DVA) |
| Pial fistula | Capillary telangiectasia |
DSA remains the gold standard for lesions with AV shunting. Cavernomas and telangiectasias are angiographically occult and characterised on MRI.
(Grainger & Allison's Diagnostic Radiology)
Cerebral (Subpial) AVM
Pathology
- Congenital anomalies consisting of direct arteriovenous shunts without a normal intervening capillary bed
- No capillary bed = high-pressure flow directly from artery to vein
- May be purely fistulous (direct single artery-to-vein connection) or have a plexiform nidus (tangle of abnormal vessels), or a combination
- Located within brain substance or cerebral sulci
- Supply from ICA or vertebrobasilar branches; may recruit additional meningeal supply
Clinical Presentation
- Intracranial hemorrhage - most common (intracerebral > subarachnoid)
- Epilepsy
- Headache
- Focal neurological deficit (ischaemia from "vascular steal")
Imaging Modalities
CT (Non-contrast)
- Lobulated hyperdense (calcification) areas in a young, normotensive patient with haemorrhage
- Areas of calcification within or around the nidus
- No mass effect unless haemorrhage present
- Surrounding low-attenuation ischaemic change (from steal)
CT with Contrast
- Avid, serpiginous enhancement of the nidus and draining veins
- CTA: used in the emergency setting to detect ruptured AVM and plan surgical approach before haematoma evacuation
- Dynamic/time-resolved CTA: good results compared with catheter angiography for demonstrating shunting
MRI
- "Flow voids" - the hallmark: signal dropout due to fast flowing blood in feeding arteries, nidus, and draining veins on T1 and T2 (serpentine dark channels)
- Mixed signal within the nidus: areas of flow void + high signal (representing thrombosis or flow-related enhancement)
- Haemorrhage at different stages of evolution within or around the nidus (T1/T2 signal varies with age of blood products - see Table 56.5)
- Surrounding T2 hyperintensity representing ischaemic change from steal or gliosis
- Dilated, early-draining veins visible as prominent serpentine structures
Key MRI sequences:
- T2/FLAIR: flow voids + surrounding ischaemia
- T1 post-contrast: enhancing nidus + draining veins
- SWI/GRE: most sensitive for haemosiderin, microbleeds, calcification
- MRA (time-of-flight or contrast-enhanced): 3D depiction of feeding vessels
DSA - Gold Standard
- Dilated feeding arteries supplying the nidus
- Early opacification of draining veins during the arterial phase = the hallmark of AV shunting
- Compact nidus tangle visible
- Important: timing of angiography matters - a haematoma can compress a small AVM making it invisible; defer to subacute phase if the patient is stable
- Very small AVMs/fistulae cannot be reliably excluded on CTA/MRA alone - DSA still required
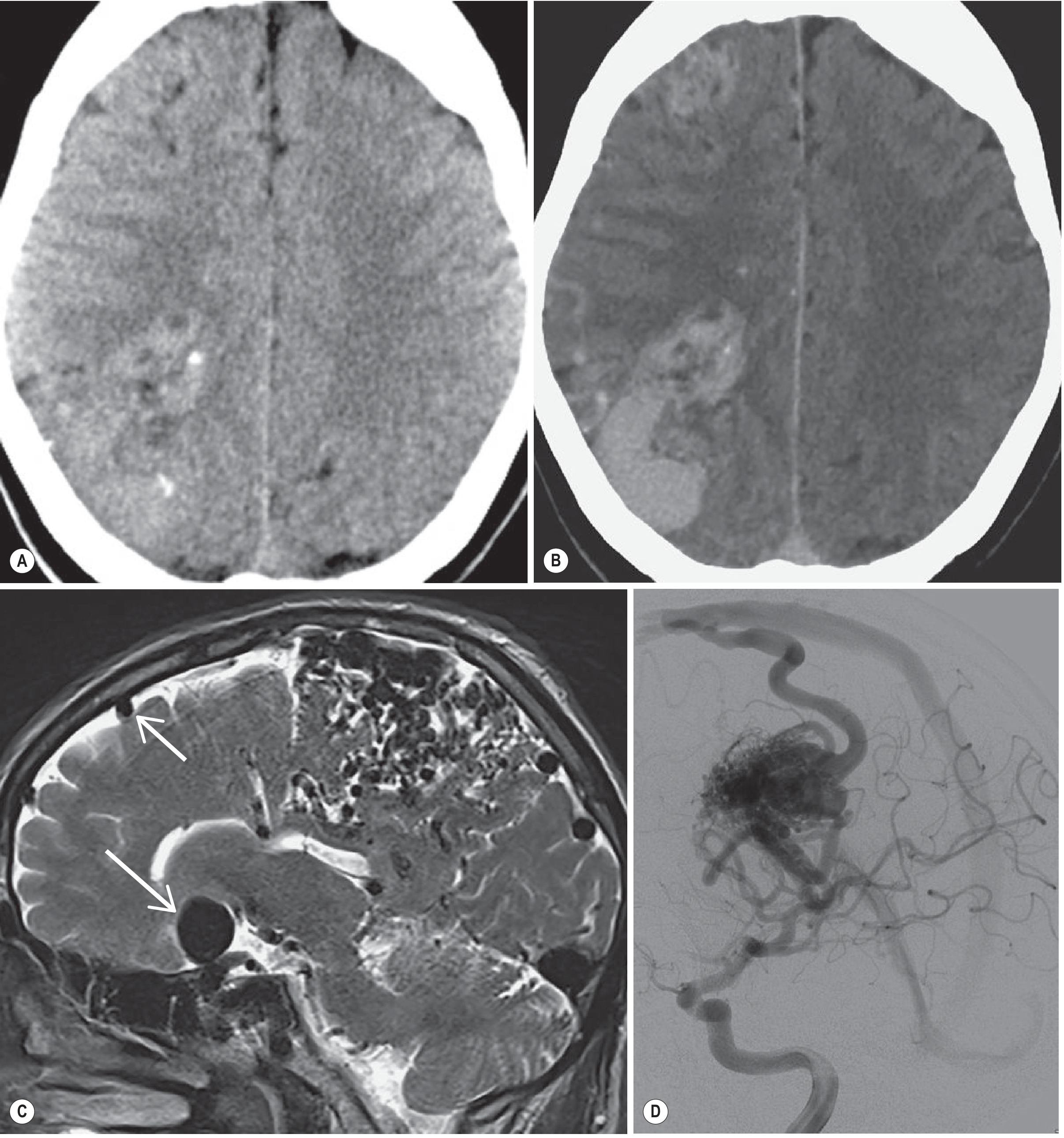
Grainger & Allison's - Fig. 56.36: CT and MRI-DSA correlation of cerebral AVM.
Spetzler-Martin Grading (for surgical risk)
| Feature | Score |
|---|---|
| Size: <3 cm | 1 |
| Size: 3-6 cm | 2 |
| Size: >6 cm | 3 |
| Eloquence of adjacent brain: non-eloquent | 0 |
| Eloquence: eloquent (motor, sensory, language, visual, brainstem, cerebellar) | 1 |
| Venous drainage: superficial only | 0 |
| Venous drainage: any deep component | 1 |
- Grade I-II: low surgical risk; Grade III: intermediate; Grade IV-V: high surgical risk
Dural Arteriovenous Fistula (dAVF)
- Direct shunts between external carotid artery branches (or meningeal branches) and dural sinuses
- Thought to be acquired (often secondary to venous sinus thrombosis)
- Clinical features depend on location and venous drainage pattern:
- Cavernous sinus: proptosis, chemosis, bruit
- Transverse/sigmoid sinus: pulsatile tinnitus
- Cortical venous reflux: intracranial haemorrhage (ICH, SAH, or subdural)
- MRI/CT: may be invisible unless there are enlarged dural sinuses or cortical veins
- MRA/CTA: may show abnormal vessels but intra-arterial DSA still needed for definitive diagnosis and treatment planning
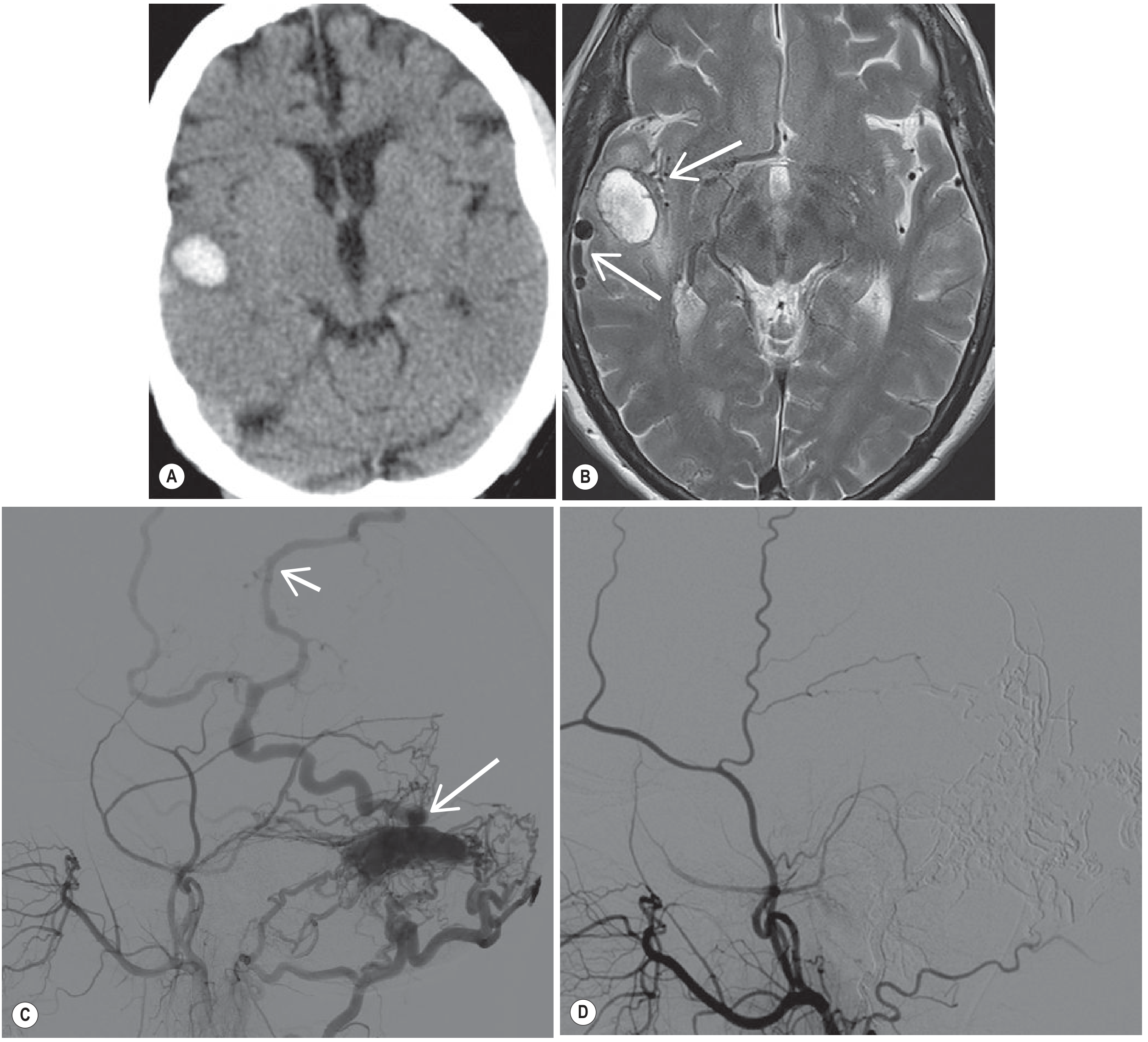
Grainger & Allison's - Fig. 56.37: dAVF CT, MRI and DSA correlation with post-embolisation.
Other Vascular Malformations - Key Imaging Points
Cavernous Angioma (Cavernoma)
- Angiographically occult - not visible on DSA
- CT: hyperdense or calcified lesion; patchy contrast enhancement
- MRI: "Popcorn" lesion - multi-lobular, mixed signal (blood products of different ages), surrounded by a dark haemosiderin rim on T2
- SWI/GRE is most sensitive sequence
- Familial form: multiple cavernomas; autosomal dominant (KRIT1, CCM2, PDCD10 mutations)
Developmental Venous Anomaly (DVA)
- Not a true malformation - benign variant of venous drainage
- "Caput medusae" pattern: radially arranged medullary veins converging on a collector vein
- Seen on venous phase of angiography or contrast-enhanced MRI/CT
- Often incidental; frequently associated with cavernomas
- No treatment needed
Capillary Telangiectasia
- Usually incidental; rarely symptomatic
- MRI: subtle T2 hyperintensity or ill-defined enhancement on post-contrast T1
- Best seen on SWI (blooming)
- Angiographically occult; no haemorrhage risk
Summary Table
| Feature | Cerebral AVM | dAVF | Cavernoma | DVA | Telangiectasia |
|---|---|---|---|---|---|
| AV shunting | Yes | Yes | No | No | No |
| Angiographic visibility | Yes | Yes | Occult | Yes (venous phase) | Occult |
| CT | Calcification, hyperdensity | Often normal | Calcification | Normal | Normal |
| MRI hallmark | Flow voids, mixed signal | Enlarged dural sinuses/veins | "Popcorn" + haemosiderin rim | Caput medusae | Brush-like enhancement |
| Best MRI sequence | T2, SWI, MRA | T2, MRV, MRA | SWI/GRE | Post-contrast T1 | SWI |
| Gold standard | DSA | DSA | MRI | MRI/contrast CT | MRI |
| Haemorrhage risk | High (~2-4%/year) | Variable (cortical reflux) | Low-moderate | Very low | Negligible |
Key clinical rule: In any young, normotensive patient with intracerebral haemorrhage, always pursue vascular imaging (CTA acutely, DSA electively) to exclude AVM. Note that a haematoma may compress and obscure a small AVM on acute angiography - repeat imaging after haematoma resolution if initial study is negative.
Source: Grainger & Allison's Diagnostic Radiology; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.