Bilirubin formation in detail from basica
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have all the detail needed to write a comprehensive answer. Let me compile it:
Bilirubin Formation - From Basics
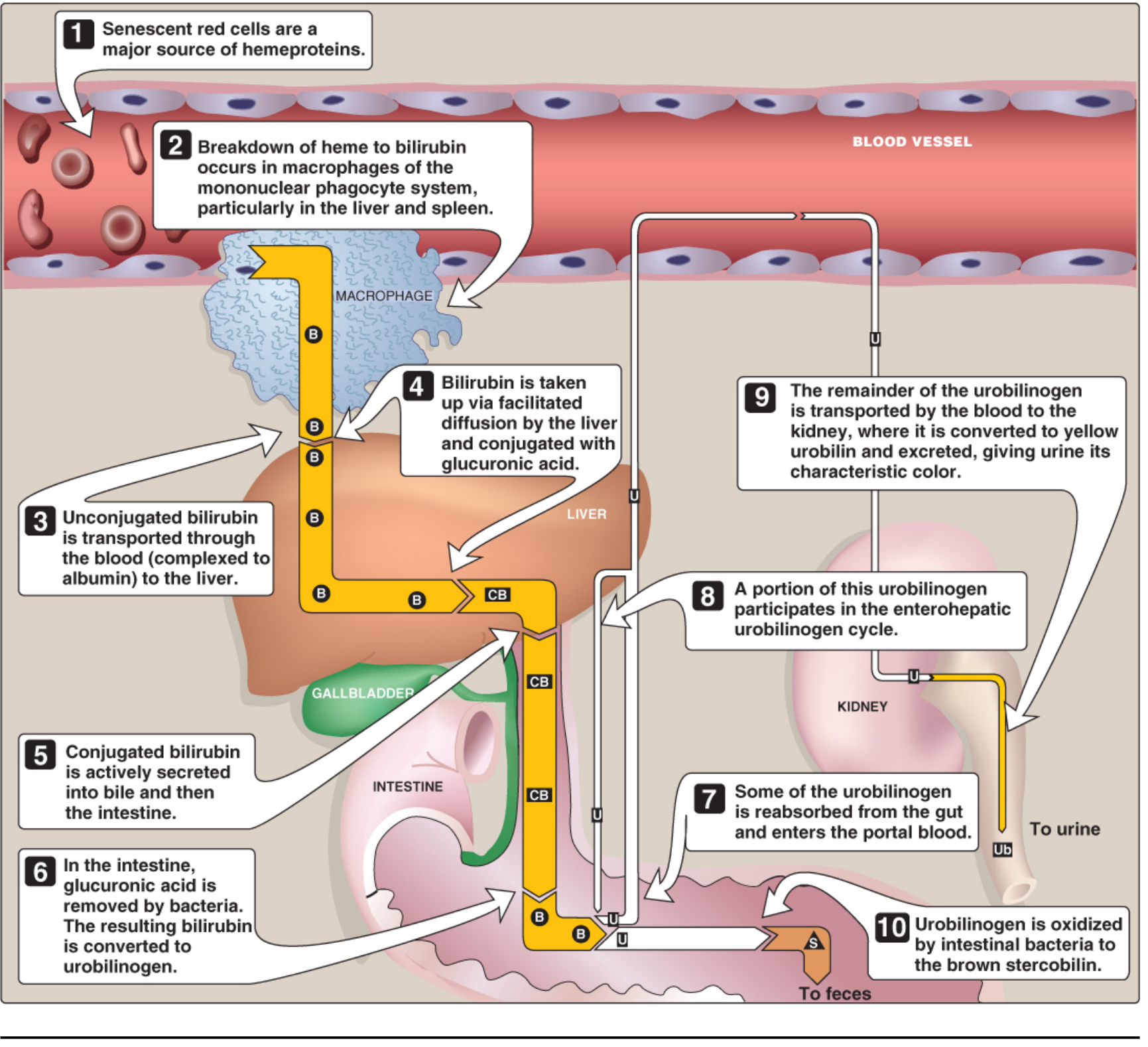
Bilirubin is the major end product of heme catabolism. Its metabolism is a tightly organized, multi-organ process spanning the mononuclear phagocyte system (MPS), blood, liver, and intestine.
1. Sources of Heme (What Gets Degraded)
About 80-85% of daily bilirubin (~4 mg/kg/day) comes from the breakdown of hemoglobin in senescent red blood cells (RBC lifespan ~120 days). The remaining 15-20% comes from:
- Premature destruction of erythroid precursors in the bone marrow (ineffective erythropoiesis)
- Turnover of non-hemoglobin hemoproteins: myoglobin, cytochrome P-450, catalase, peroxidase
These sources are collectively called the "early-labeled" bilirubin fraction.
Harrison's Principles of Internal Medicine 22E, p. 364
2. Step 1 - RBC Destruction and Heme Liberation
Senescent RBCs are engulfed by macrophages of the MPS - primarily in the spleen, liver (Kupffer cells), and bone marrow. Inside the macrophage:
- Hemoglobin is split into globin (recycled as amino acids) and heme (ferroprotoporphyrin IX)
- Heme = an iron-containing, cyclic tetrapyrrole (porphyrin ring with Fe²⁺ at the center)
3. Step 2 - Heme → Biliverdin (via Heme Oxygenase)
This is the rate-limiting step in bilirubin formation.
Enzyme: Microsomal heme oxygenase (located in the ER of macrophages)
Reaction: Three successive oxygenations using NADPH + O₂:
- The α-methene bridge carbon of the porphyrin ring is oxidatively cleaved
- The cyclic heme ring is opened to form a linear tetrapyrrole
- Products released: Biliverdin (green pigment) + CO (carbon monoxide) + Fe²⁺
The equation per molecule of heme:
Heme + 3O₂ + 3NADPH → Biliverdin + CO + Fe²⁺ + 3NADP⁺
By-products have functions:
- CO acts as a signaling molecule and anti-inflammatory mediator
- Fe²⁺ is recycled - bound to transferrin and transported back to bone marrow for re-use in new hemoglobin
In birds, reptiles, and amphibians, biliverdin is the final excretory product. In mammals, it is reduced further to bilirubin - this is evolutionarily important because bilirubin (unlike biliverdin) can cross the placenta, allowing fetal bilirubin to be excreted via the maternal liver.
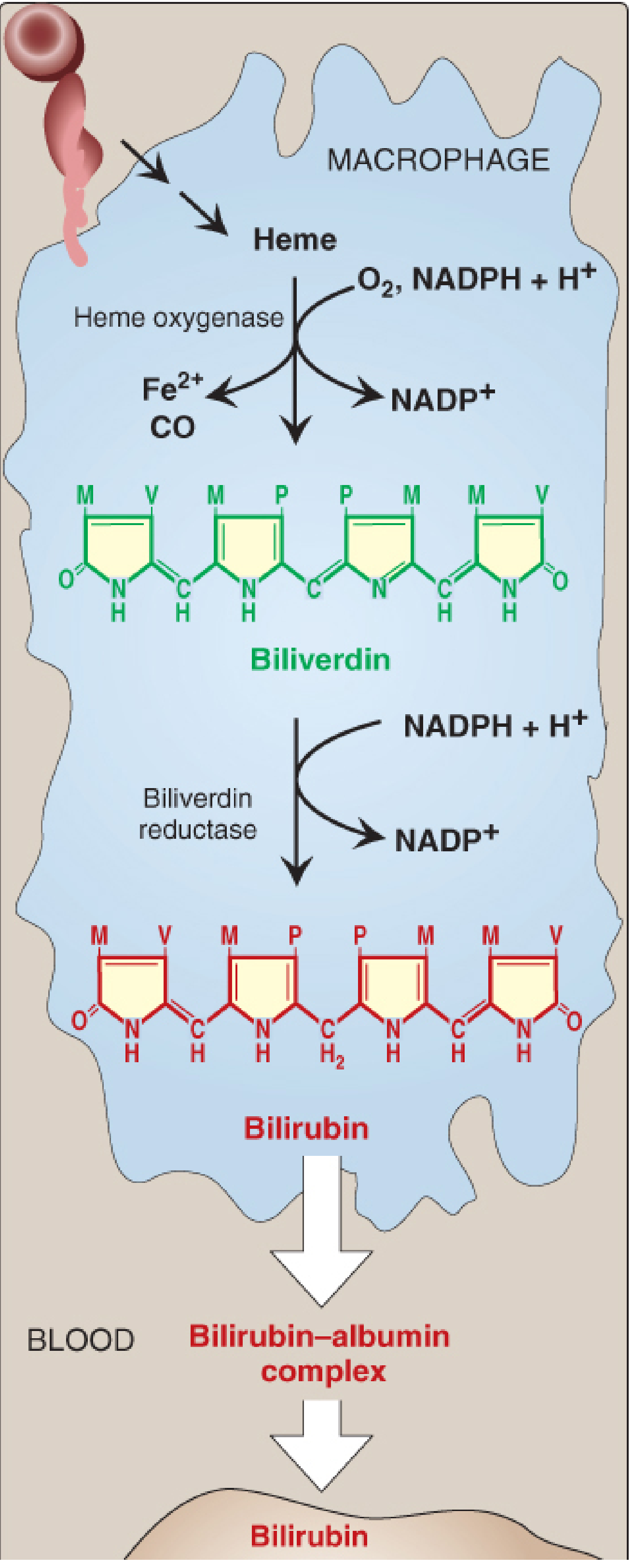
4. Step 3 - Biliverdin → Bilirubin (via Biliverdin Reductase)
Enzyme: Cytosolic biliverdin reductase
Reaction: Reduces the central methylene bridge of biliverdin using NADPH:
Biliverdin + NADPH + H⁺ → Bilirubin + NADP⁺
This converts the green biliverdin to the characteristic red-orange bilirubin.
Why bilirubin is insoluble: Bilirubin has tight internal hydrogen bonds between its propionic acid carboxyl groups and the imino/lactam groups of the opposite dipyrrolic half. This "ridge-tile" configuration:
- Places hydrophobic residues outward
- Buries polar residues inward
- Makes bilirubin virtually insoluble in water
Note: Bilirubin in mammals also has antioxidant function at low concentrations. It is oxidized back to biliverdin, which is then reduced again by biliverdin reductase - creating a redox cycle.
Lippincott's Illustrated Reviews: Biochemistry 8e, p. 795
5. Step 4 - Blood Transport (Unconjugated Bilirubin)
Because bilirubin is water-insoluble, it cannot travel freely in plasma. It is:
- Bound noncovalently to albumin (2 binding sites per albumin molecule)
- This form is called unconjugated (indirect) bilirubin or free bilirubin
- It is NOT filtered by the kidney in normal conditions (too large as albumin complex)
Clinical note: Certain drugs (salicylates, sulfonamides, furosemide, radiographic contrast agents) competitively displace bilirubin from albumin. In neonates, this raises free bilirubin which can cross the blood-brain barrier and cause kernicterus.
Goldman-Cecil Medicine, Chapter 133
6. Step 5 - Hepatic Uptake
When albumin-bilirubin complex reaches the liver sinusoids:
- Bilirubin dissociates from albumin (albumin stays in blood)
- Unconjugated bilirubin enters hepatocytes by facilitated diffusion (specific transporters, including OATP1B1/OATP1B3)
- Inside the hepatocyte cytosol, bilirubin binds to ligandin (glutathione-S-transferase Y) and protein Z - these reduce back-diffusion and shuttle bilirubin to the ER
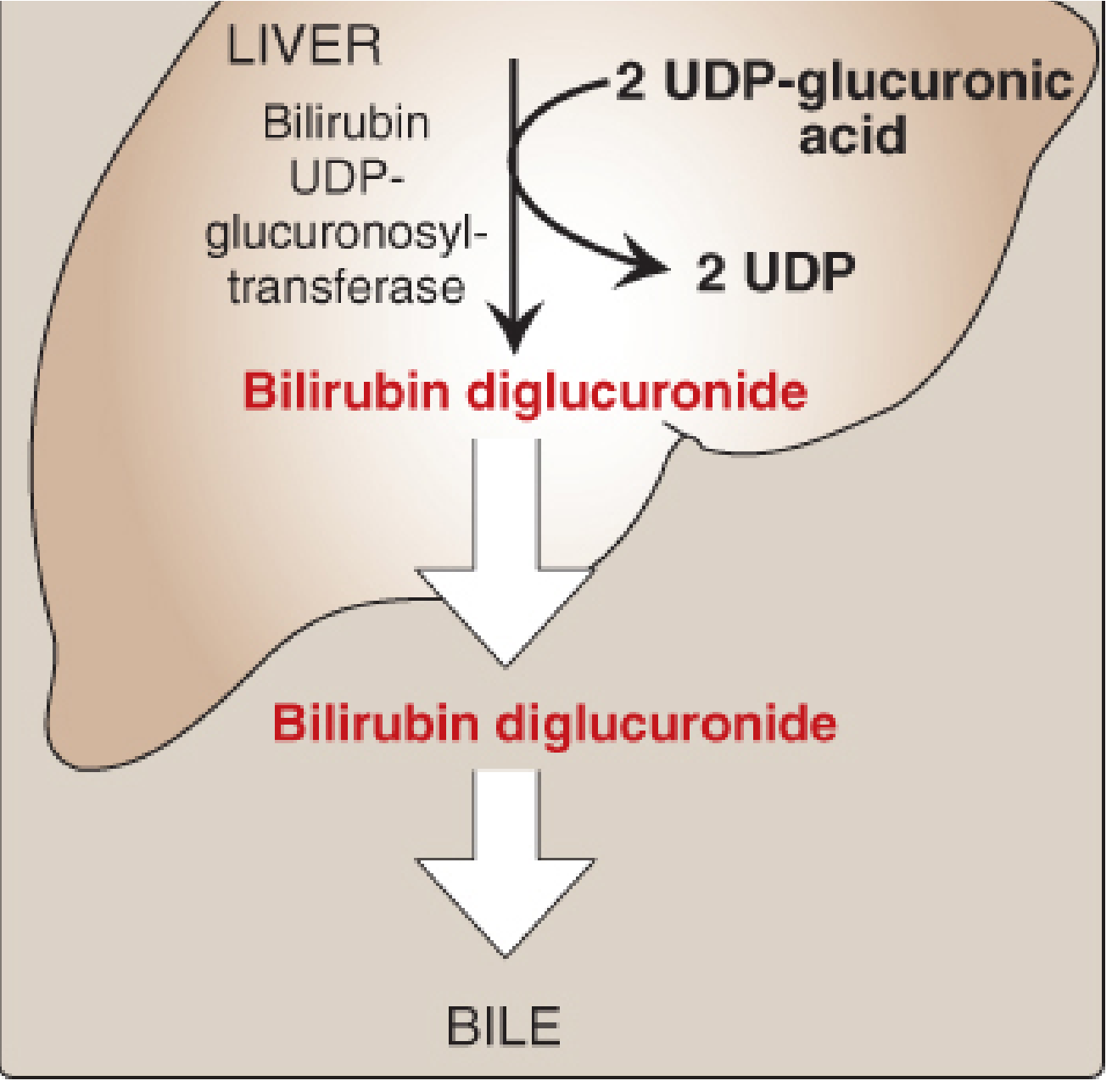
7. Step 6 - Conjugation in the Liver (Making Bilirubin Water-Soluble)
Location: Endoplasmic reticulum of hepatocytes
Enzyme: Bilirubin UDP-glucuronosyltransferase (UGT1A1), encoded by the UGT1 gene complex
Reaction: Sequential addition of two glucuronic acid molecules from UDP-glucuronic acid:
- Bilirubin + UDP-glucuronic acid → Bilirubin monoglucuronide (BMG)
- BMG + UDP-glucuronic acid → Bilirubin diglucuronide (BDG) ← predominant form
The conjugation disrupts the internal hydrogen bonds, making bilirubin water-soluble (conjugated/direct bilirubin). It can now be excreted.
According to Guyton and Hall: ~80% is conjugated as bilirubin glucuronide, ~10% as bilirubin sulfate, and ~10% with other substances.
Clinical relevance of UGT1A1:
- Gilbert syndrome: Mild UGT1A1 reduction → mild unconjugated hyperbilirubinemia
- Crigler-Najjar syndrome type I: Complete absence of UGT1A1 → severe, life-threatening unconjugated hyperbilirubinemia
- Crigler-Najjar syndrome type II (Arias): Markedly reduced UGT1A1
8. Step 7 - Biliary Secretion
Conjugated bilirubin is actively transported across the canalicular membrane into bile by:
- MRP2 (Multidrug Resistance-associated Protein 2), also called cMOAT/ABCC2 - an ATP-dependent transporter
- This is the rate-limiting step for bilirubin excretion (not conjugation)
- MRP3 transports some conjugated bilirubin back into sinusoidal blood when MRP2 is overloaded (regurgitation pathway)
Clinical note: Deficiency of MRP2 (canalicular transport) = Dubin-Johnson syndrome (conjugated hyperbilirubinemia, benign).
Conjugated bilirubin flows into bile, is stored in the gallbladder, and enters the duodenum.
9. Step 8 - Intestinal Fate and Enterohepatic Circulation
In the small intestine, conjugated bilirubin is NOT absorbed (too hydrophilic and large). In the terminal ileum and colon, intestinal bacteria:
- Hydrolyze the glucuronide conjugate (beta-glucuronidase) → free unconjugated bilirubin
- Reduce bilirubin → urobilinogen (colorless compound), a series of compounds (mesobilirubinogen, stercobilinogen)
Fate of urobilinogen:
- Most (~80%) is further oxidized by bacteria to stercobilin (brown pigment) → excreted in feces (gives stool its brown color)
- ~20% is reabsorbed from the gut into portal blood:
- Most is re-extracted by the liver and re-secreted into bile = enterohepatic circulation of urobilinogen
- A small fraction escapes into systemic blood → kidneys → oxidized to urobilin (yellow) → excreted in urine (gives urine its yellow color)
Summary Table
| Stage | Location | Key Enzyme/Protein | Product |
|---|---|---|---|
| RBC destruction | Spleen/liver/BM macrophages | - | Heme liberated |
| Heme → Biliverdin | Macrophage ER | Heme oxygenase | Biliverdin + CO + Fe²⁺ |
| Biliverdin → Bilirubin | Macrophage cytosol | Biliverdin reductase | Unconjugated bilirubin |
| Blood transport | Plasma | Albumin | Bilirubin-albumin complex |
| Hepatic uptake | Hepatocyte cytosol | Ligandin/OATP | Unconjugated bilirubin (intrahepatic) |
| Conjugation | Hepatocyte ER | UGT1A1 | Bilirubin diglucuronide (conjugated) |
| Biliary secretion | Bile canaliculus | MRP2 (ATP-dependent) | Conjugated bilirubin in bile |
| Intestinal reduction | Colon bacteria | Bacterial reductases | Urobilinogen |
| Fecal excretion | Intestine | Bacterial oxidases | Stercobilin (brown) |
| Urinary excretion | Kidney | - | Urobilin (yellow) |
Normal Reference Values
- Total serum bilirubin: ≤1 mg/dL
- Conjugated (direct): ≤0.3 mg/dL
- Jaundice clinically visible: ≥2-3 mg/dL
Sources: Lippincott's Illustrated Reviews: Biochemistry 8e (pp. 794-799) | Harrison's Principles of Internal Medicine 22E (p. 364) | Goldman-Cecil Medicine, Chapter 133 | Guyton and Hall Medical Physiology 14e, Chapter 71
This is a shared conversation. Sign in to Orris to start your own chat.