portal vein obstruction caput medusae
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information. Let me compose the full answer.
Portal Vein Obstruction & Caput Medusae
These two findings are intimately linked: portal vein obstruction raises portal venous pressure, and caput medusae is one of the classic collateral pathways that develops as a result.
Portal Vein Obstruction
Overview
Blockage of the portal vein and its tributaries may be insidious and well tolerated, or may be a catastrophic, potentially lethal event. Occlusive disease typically produces abdominal pain and, in most instances, manifestations of portal hypertension - principally esophageal varices prone to rupture.
- Robbins Pathologic Basis of Disease
Levels of Obstruction
| Level | Typical Causes |
|---|---|
| Extrahepatic portal vein | Neonatal umbilical sepsis, hypercoagulable states, trauma, pancreatitis/pancreatic cancer, HCC invasion, cirrhosis |
| Intrahepatic portal vein radicles | Acute thrombosis (often malignancy or hypercoagulable state) |
| Small portal vein branches | Schistosomiasis (most common worldwide); idiopathic noncirrhotic portal hypertension |
Causes of Extrahepatic Portal Vein Obstruction
- Neonatal umbilical sepsis or umbilical vein catheterization - often subclinical; presents with variceal bleeding and ascites years later
- Intraabdominal sepsis (diverticulitis, appendicitis) causing pylephlebitis in the splanchnic circulation
- Hypercoagulable states - myeloproliferative neoplasms (polycythemia vera), Factor V Leiden, etc.
- Trauma - surgical or otherwise
- Pancreatitis / pancreatic cancer - splenic vein thrombosis propagating into the portal vein
- Hepatocellular carcinoma - direct vascular invasion
- Cirrhosis - associated with portal vein thrombosis in ~25% of patients
- Robbins Pathologic Basis of Disease
Small Branch Obstruction - Special Cases
- Schistosomiasis: The most common cause worldwide. Parasite eggs lodge in small portal vein branches; the granulomatous response causes periportal fibrosis ("pipestem fibrosis") and noncirrhotic portal hypertension.
- Idiopathic noncirrhotic portal hypertension: Associated with prothrombotic states, HIV infection (and antiretroviral therapy), toxins, autoimmune diseases. Particularly common in India. Liver transplantation may be necessary for fatal sequelae.
Portal Hypertension and Collateral Formation
When portal venous pressure exceeds 12 mmHg, clinically significant portal hypertension develops. Portosystemic collaterals form at sites where portal and caval systems communicate, allowing blood to bypass the obstructed liver.
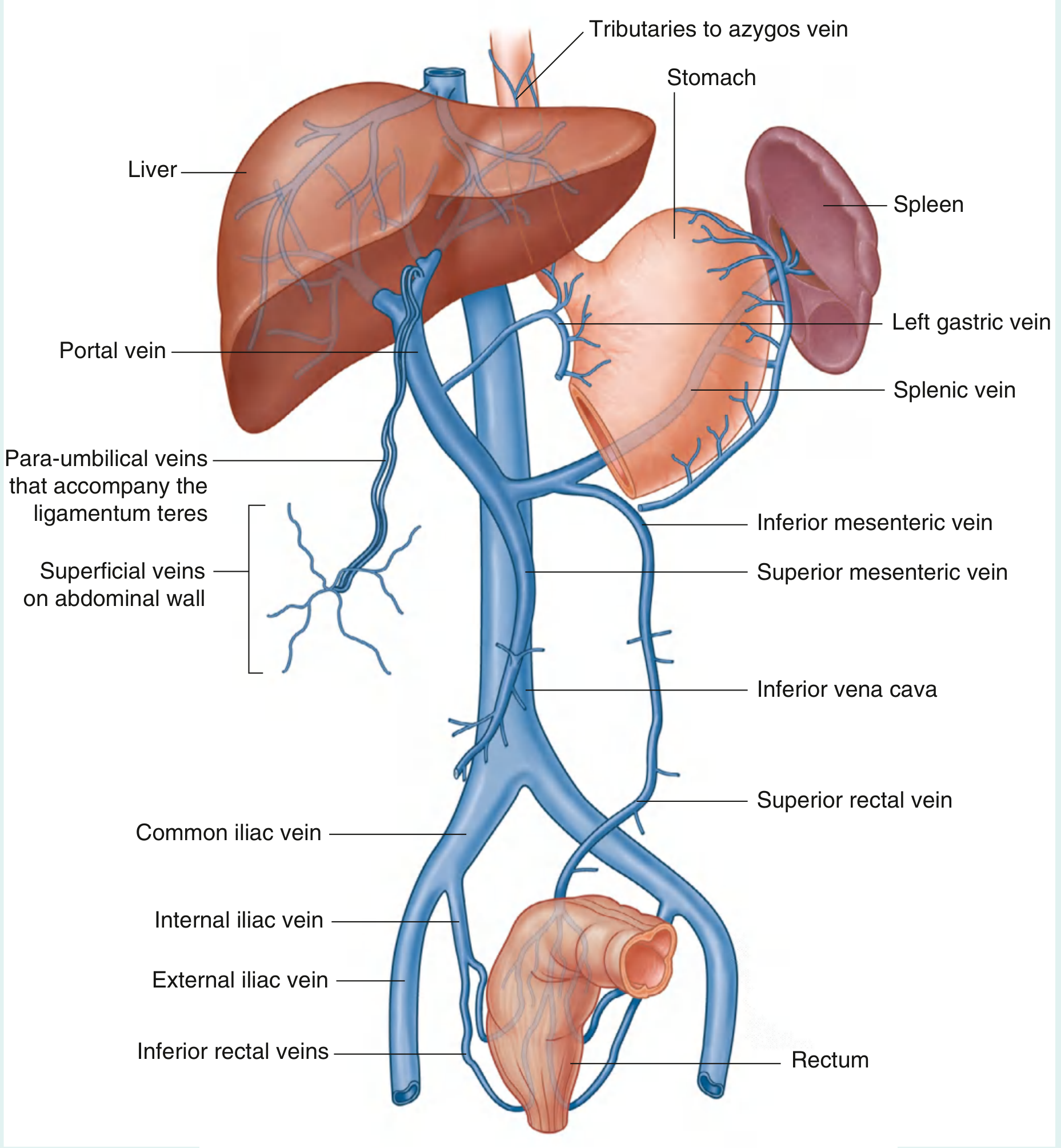
The three major sites of portosystemic anastomosis are:
| Site | Portal Tributary | Systemic Tributary | Result |
|---|---|---|---|
| Gastroesophageal junction | Left gastric (coronary) vein | Tributaries to azygos vein | Esophageal varices |
| Anorectal junction | Superior rectal vein | Inferior/middle rectal veins | Anorectal varices |
| Umbilicus | Para-umbilical veins | Superficial epigastric veins | Caput medusae |
- Gray's Anatomy for Students; Sleisenger & Fordtran's GI and Liver Disease
Caput Medusae
Definition and Mechanism
Caput medusae (Latin: "head of Medusa") refers to the visible, dilated, tortuous veins radiating from the umbilicus across the anterior abdominal wall. It is a sign of portal hypertension.
Mechanism:
-
Normally, the umbilical vein obliterates after birth to form the ligamentum teres.
-
In portal hypertension, increased portal pressure forces blood through patent para-umbilical veins that accompany the ligamentum teres.
-
These para-umbilical veins connect the left branch of the portal vein to the superficial veins of the anterior abdominal wall.
-
Blood bypasses the liver, flowing from the portal system into the superficial epigastric veins (which drain into the external iliac vein) and the thoracoepigastric veins (which drain into the axillary vein).
-
The result is visibly engorged superficial veins radiating outward from the umbilicus, resembling the snakes on Medusa's head.
-
Goldman-Cecil Medicine; Gray's Anatomy for Students
Clinical Photograph

From Goldman-Cecil Medicine: caput medusae accentuated by massive ascites in a liver transplant candidate. The large vein coursing inferiorly along the right flank (arrows) is the superficial epigastric vein draining into the external iliac vein.
Clinical Significance
- One of the classic stigmata of chronic liver disease and portal hypertension, alongside spider nevi, palmar erythema, and ascites.
- Helps distinguish portal hypertension from inferior vena cava (IVC) obstruction: in portal hypertension, blood in caput medusae flows away from the umbilicus in all directions; in IVC obstruction, flow is upward (as the collaterals carry blood around the obstructed IVC toward the superior vena cava).
- Tintinalli's Emergency Medicine; Goldman-Cecil Medicine
Flow Direction Test (Practical Exam Point)
To determine flow direction: place two fingers on a vein, milk the blood out, then release one finger and watch which direction refilling occurs.
- Caput medusae (portal HTN): centrifugal (away from umbilicus in all directions)
- IVC obstruction collaterals: upward (inferior to superior)
Summary
Portal vein obstruction
↓
Portal hypertension (>12 mmHg gradient)
↓
Portosystemic collateral formation
├── Esophageal varices (left gastric → azygos)
├── Anorectal varices (superior rectal → inferior rectal)
└── Caput medusae (para-umbilical → superficial epigastric veins)
Caput medusae is a direct visible consequence of the para-umbilical collateral pathway opening up in response to portal vein obstruction / portal hypertension. It is always abnormal and should prompt investigation for underlying liver disease or portal vein pathology.
This is a shared conversation. Sign in to Orris to start your own chat.