Treatment of supracondylar humerus in children
Reading File
Finding Sources
Searching PubMed
"supracondylar humerus fracture" AND children AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to write a detailed, well-structured response. Let me compile everything.
Supracondylar Humerus Fractures in Children
Supracondylar humerus fractures are the most common elbow fractures in children, with peak incidence between ages 5-7. Extension-type (posterior displacement) accounts for ~97-98% of cases; flexion-type is rare (~2%).
Mechanism and Clinical Presentation
Extension type: Fall on an outstretched hand with the elbow extended or hyperextended. The triceps pulls the distal fragment posteriorly and proximally. The child holds the arm at the side with a characteristic S-shaped deformity. The sharp proximal fragment may threaten the anterior neurovascular structures (brachial artery, anterior interosseous nerve/median nerve).
Flexion type: Direct blow to the posterior aspect of the flexed elbow. The distal fragment displaces anteriorly. The child supports the forearm with the opposite hand, elbow at 90 degrees. Ulnar nerve injury occurs in over 90% of flexion-type cases.
Radiographic Assessment
Two key measurements guide diagnosis and reduction quality:
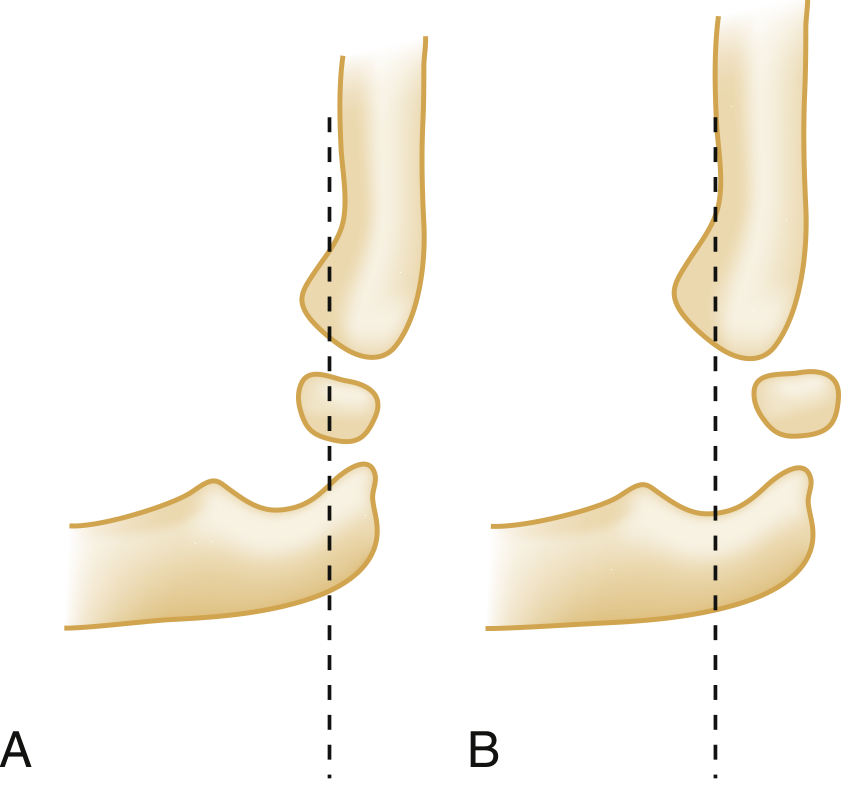
1. Anterior humeral line - drawn along the anterior cortex of the humerus on a lateral film. Normally transects the middle third of the capitellum. In extension supracondylar fractures, it passes through the anterior third or entirely anterior to the capitellum.

2. Baumann's angle - intersection of the humeral mid-shaft axis with the capitellar physis on AP film, normally ~75 degrees. Asymmetry indicates varus/valgus malreduction.
Soft tissue signs: A posterior fat pad sign on lateral film, or an abnormal anterior humeral line, may be the only evidence of a minimally displaced fracture. Comparison views of the contralateral elbow are often useful in children.
CRITOE mnemonic (ossification center appearance sequence):
| Center | Age of Appearance |
|---|---|
| Capitellum | 1-2 years |
| Radial head | 4-5 years |
| Internal (medial) epicondyle | 4-5 years |
| Trochlea | 8-10 years |
| Olecranon | 8-9 years |
| External (lateral) epicondyle | 10-11 years |
Classification: Gartland (Modified)
| Type | Description |
|---|---|
| Type I | Non-displaced or minimally displaced; posterior cortex intact |
| Type IIA | Displaced, posterior cortex intact, no rotational component |
| Type IIB | Displaced, posterior cortex intact, with rotational component |
| Type III | Completely displaced; no cortical contact; periosteal contact remains |
| Type IIIA | No rotation |
| Type IIIB | Rotation present |
| Type IV | Complete circumferential periosteal disruption; multidirectionally unstable |
Treatment by Type
Type I (Non-displaced)
- Immobilize in a posterior splint or long-arm cast with elbow flexed 75-80 degrees, forearm in neutral rotation
- Protected range of motion begins at ~3 weeks
- Discharge from ED with instructions to elevate, apply ice, and follow up in 1-2 days
- Even without definite radiographic fracture, a child with localized tenderness consistent with a supracondylar fracture should be splinted and reviewed within 24-48 hours
- Source: Rosen's Emergency Medicine, Bailey and Love's
Type IIA (Displaced, no rotation, posterior cortex intact)
- Closed reduction under procedural sedation
- If the dorsal periosteal hinge is intact, above-elbow cast immobilization for 3-4 weeks is often sufficient to hold the reduction
- Elbow flexion to 110-120 degrees uses the intact posterior periosteum as a tension band
- If swelling prevents this degree of flexion, do not force it - this risks vascular obstruction
- Admit for neurovascular monitoring during first 24-48 hours when swelling peaks
- Source: Rosen's Emergency Medicine, Bailey and Love's
Type IIB (Displaced with rotation)
- Closed reduction + percutaneous K-wire (Kirschner wire) pinning is recommended
- Studies show better outcomes with pinning than without for IIB fractures
- Above-elbow cast applied after pinning
- Source: Rosen's Emergency Medicine
Type III (Completely displaced)
- Closed reduction and percutaneous pinning (CRPP) is the gold standard
- Operative timing: urgent, though not all centers require "emergent" same-night surgery - evidence supports safe delay to next morning with close neurovascular monitoring for stable type III injuries (without vascular compromise)
- If closed reduction fails: open reduction via anterior (cubital) or lateral approach
- Admit for neurovascular observation; risk of compartment syndrome highest at 24-48 hours
- Source: Rosen's Emergency Medicine, Campbell's Operative Orthopaedics
Type IV (Circumferential periosteal disruption)
- Emergent orthopedic consultation and operative intervention
- These are surgically challenging but good outcomes are achievable
- Source: Rosen's Emergency Medicine
Percutaneous Pinning Technique
- Standard technique: two or three lateral-entry K-wires (all from lateral side), or cross-pinning (one medial + one lateral)
- Lateral-entry pins are preferred by most surgeons - they avoid iatrogenic ulnar nerve injury while providing adequate stability when divergent configuration is used
- Cross-pin (medial + lateral) provides better rotational stability biomechanically but risks ulnar nerve injury with the medial pin
- If medial pin is used, the elbow should be extended (not fully flexed) to protect the ulnar nerve
- Recent network meta-analysis (Lin et al., 2026, PMID 41076056) examined optimal pin configurations, with biomechanical data favoring three lateral pins for most fractures
- Pins are typically removed in clinic at 3-4 weeks once early healing is confirmed
Neurovascular Injuries
Nerve injuries occur in ~10% of extension-type fractures overall, rising to 20-50% with increasing displacement severity. Most are neuropraxias that resolve with fracture reduction and swelling subsidence. Motor function typically returns within 7-12 weeks; sensory recovery can take over 6 months.
| Fracture Type | Most Common Nerve Injury |
|---|---|
| Extension type | Anterior interosseous nerve > radial nerve > median nerve |
| Flexion type | Ulnar nerve (>90% of cases) |
Vascular Injury
Pulseless hand occurs in ~10% of cases (usually swelling, not direct arterial injury). Two scenarios:
- White pulseless hand: Surgical emergency. Requires immediate assessment and urgent reduction. If pulse does not return after reduction, vascular exploration by a vascular surgeon is mandatory.
- Pink pulseless hand (adequate perfusion): More controversial. If there is satisfactory perfusion, no compartment syndrome, and no neurological injury, fracture reduction and stabilization with a more expectant approach is acceptable. The pulse often returns within 24-48 hours.
Complications
| Complication | Notes |
|---|---|
| Volkmann's ischaemic contracture | Rare but feared. Due to excessive swelling and missed compartment syndrome. Do NOT place elbow in deep flexion with significant swelling; use K-wire fixation instead |
| Cubitus varus (gunstock deformity) | Most common malunion. Due to varus malreduction. More cosmetic than functional. Corrected by supracondylar osteotomy if severe |
| Cubitus valgus | Less common malunion |
| Compartment syndrome | Risk peaks at 24-48 hours post-injury; monitor carefully after reduction |
| Iatrogenic ulnar nerve injury | Risk with medial-entry pin; use lateral-only configuration when possible |
| Stiffness | Usually resolves with time; avoid prolonged immobilization |
Flexion-Type Fractures (Special Considerations)
- Immobilize in extension (not flexion) - anterior periosteum acts as tension band
- Type I: splint comfortably flexed, no need for extension immobilization
- Types II and III: emergent orthopedic consultation; closed reduction and percutaneous pinning; open reduction if CR fails
- Ulnar nerve is at highest risk
Summary Algorithm
Supracondylar fracture identified
|
_____|______
| |
Type I Types II-IV
| |
Splint Neurovascular assessment FIRST
75-80° |
Outpatient Pulseless/ischemic → emergent
________________________
| |
Type IIA Type IIB/III
CR + cast CRPP (lateral K-wires)
(if hinge intact) Admit/monitor
|
Type IV
Emergent OR
Sources:
- Rosen's Emergency Medicine, Ch. 44 (Pediatric Extremity Fractures)
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 32
- Campbell's Operative Orthopaedics, 15th Ed. 2026 (SUPRACONDYLAR FRACTURES section)
Recent evidence: A 2026 network meta-analysis (PMID 41076056) on pin configuration optimization suggests three lateral-entry pins offer superior biomechanical stability. No major departures from established management principles were identified in 2024-2026 systematic reviews.
This is a shared conversation. Sign in to Orris to start your own chat.