Management of stroke
Reading File
Finding Sources
Searching PubMed
"ischemic stroke" AND management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a thorough, well-organized response. Here is the comprehensive synthesis:
Management of Stroke
Stroke management divides into two broad tracks - ischemic stroke (~85% of cases) and hemorrhagic stroke (~15%) - plus a shared framework of acute stabilization, prevention of complications, and secondary prevention. Time is the most critical variable in every phase.
1. ACUTE STABILIZATION (All Stroke Types)
Airway, Breathing, Circulation
- Protect the airway: prevent obstruction, hypoventilation, and aspiration
- Pulse oximetry or ABG; supplemental oxygen if saturation is low
- Cardiac monitoring for at least 48 hours (arrhythmias occur in up to 20% of patients, and concomitant myocardial ischemia in 3-20%)
- Immediate 12-lead ECG and troponin level
- Admit to a stroke unit - this alone reduces mortality, shortens hospital stay, and reduces nursing-home discharge rates
Emergency Investigations
| Investigation | Purpose |
|---|---|
| CT head without contrast (urgent) | Rule out hemorrhage before any thrombolytic |
| CTA / CT perfusion | Identify large vessel occlusion; select for thrombectomy |
| CBC with differential, platelet count | Thrombocytopenia excludes tPA |
| PT/INR, aPTT | Coagulopathy excludes tPA |
| Electrolytes, BUN, creatinine, glucose | Metabolic mimics; guide management |
| Oxygen saturation | Hypoxia worsens ischemia |
| Echocardiography (TEE/TTE) | Cardioembolic source |
| Carotid duplex ultrasonography | Carotid stenosis |
Assess with the NIH Stroke Scale (NIHSS) - scores >15 indicate large infarction. Patients with TIA or acute stroke within 72 hours of onset should be hospitalized.
- Bradley and Daroff's Neurology in Clinical Practice; Textbook of Family Medicine 9e
2. ISCHEMIC STROKE: ACUTE REPERFUSION THERAPY
A. Intravenous Thrombolysis - Alteplase (tPA)
The NINCDS trial established tPA 0.9 mg/kg IV (max 90 mg, 10% as bolus, 90% over 60 minutes) within a 3-hour window, with benefit extending to 4.5 hours for selected patients. Patients treated earliest within the 3-hour window had more benefit. Symptomatic cerebral hemorrhage occurs in ~6% (twice the untreated rate).
AHA/ASA 2018 Inclusion Criteria:
- Age ≥18 years
- Measurable neurological deficit from acute ischemic stroke
- Symptom onset <3 hours (standard) or 3-4.5 hours (extended)
Key Exclusion Criteria:
- Intracranial hemorrhage on CT (any type)
- Prior ischemic stroke or severe head trauma within 3 months
- Intracranial/intraspinal surgery within 3 months
- GI malignancy or GI bleeding within 21 days
- Pre-treatment SBP >185 mmHg or DBP >110 mmHg despite treatment
- Platelet count <100,000/mm³
- INR >1.7, aPTT >40s, or PT >15s
- Use of LMWH within 48 hours
- Current direct thrombin inhibitors or direct Xa inhibitors
- CT showing extensive hypoattenuation (>2/3 of MCA territory)
- NIHSS too low (mild/rapidly-improving deficit, score ≤3) or stroke too massive
Tenecteplase (0.25 mg/kg) has shown similar results to alteplase in some trials, and may have improved revascularization rates before thrombectomy.
Note: If tPA is given, blood pressure must be maintained below 185/110 mmHg.
- Adams and Victor's Principles of Neurology 12e; Bradley and Daroff's Neurology in Clinical Practice
B. Endovascular Thrombectomy (Mechanical)
Mechanical clot retrieval devices (stent retrievers) are the standard for large vessel occlusion (intracranial ICA, M1/M2 MCA, less often ACA):
- Standard window: up to 6-8 hours from onset
- Extended window: up to 16-24 hours with appropriate imaging selection (mismatch on CT perfusion/MRI)
- Main selection criterion: confirmed large-vessel occlusion on CTA
- The ASPECTS score gauges extent of infarction to guide eligibility
- A 2025 meta-analysis (PMID: 40245349) confirms endovascular thrombectomy benefit even for large ischemic core strokes
- Adams and Victor's Principles of Neurology 12e
3. BLOOD PRESSURE MANAGEMENT IN ISCHEMIC STROKE
Areas of cerebral ischemia lose autoregulation - perfusion becomes directly dependent on mean arterial pressure. Aggressive BP lowering can convert ischemic penumbra into infarcted tissue.
| Situation | BP Threshold for Treatment |
|---|---|
| No tPA | Do NOT treat unless SBP persistently >220 or DBP >120 mmHg |
| After tPA | Maintain <185/110 mmHg |
| With active MI, heart failure, aortic dissection, renal failure | More aggressive control |
When treatment is needed, preferred agents are:
- Nicardipine 5 mg/hr IV (first-line, titrate to max 15 mg/hr)
- Labetalol 10 mg IV over 1-2 min (repeat/double every 10-20 min, max 300 mg)
- Sodium nitroprusside 0.3 mcg/kg/min IV (avoid if possible - causes cerebral vasodilation, can worsen edema)
- Sublingual calcium channel blockers are contraindicated (precipitous BP drops)
- Textbook of Family Medicine 9e; Bradley and Daroff's Neurology in Clinical Practice
4. GLUCOSE AND TEMPERATURE MANAGEMENT
- Glucose: Keep close to euglycemia. Hyperglycemia worsens ischemic outcome. However, intensive glucose control (SHINE trial, GIST-UK, SELESTIAL) conferred no benefit and increased hypoglycemia risk. Use standard glucose control.
- Temperature: Mild hypothermia is neuroprotective; hyperthermia worsens ischemic outcome. Treat fever aggressively.
- Avoid supplemental oxygen in normoxic patients (large RCT showed no benefit from low-dose O₂ in acute stroke).
- Adams and Victor's Principles of Neurology 12e; Bradley and Daroff's Neurology in Clinical Practice
5. CEREBRAL EDEMA AND RAISED ICP IN ISCHEMIC STROKE
Brain edema peaks at 72-120 hours post-infarction. Cytotoxic edema precedes vasogenic edema. Younger patients and those with large MCA territory infarctions are at highest risk of herniation.
Medical management of raised ICP:
- Head of bed elevated 15-30 degrees
- Correct hypercarbia, hypoxia, hyperthermia, acidosis, hypotension, hypovolemia
- Avoid head/neck positions compressing jugular veins
- Hyperventilation to PaCO₂ 35±3 mmHg (if actively herniating - short-term bridge only)
- Mannitol 0.25-1 g/kg IV over 30 minutes (max 2 g/kg total; repeat every 6 hours); replace urinary losses with normal saline
- Hypertonic saline - alternative to mannitol
- IV fluids: isotonic (normal saline); avoid glucose-containing solutions
Do not use corticosteroids in ischemic stroke edema - they are ineffective and worsen hyperglycemia.
Surgical options:
- Hemicraniectomy + durotomy for malignant MCA infarction (improves survival and functional outcome)
- Posterior fossa decompression for cerebellar stroke with herniation (can be life-saving)
- Ventriculostomy (risk of upward cerebellar herniation)
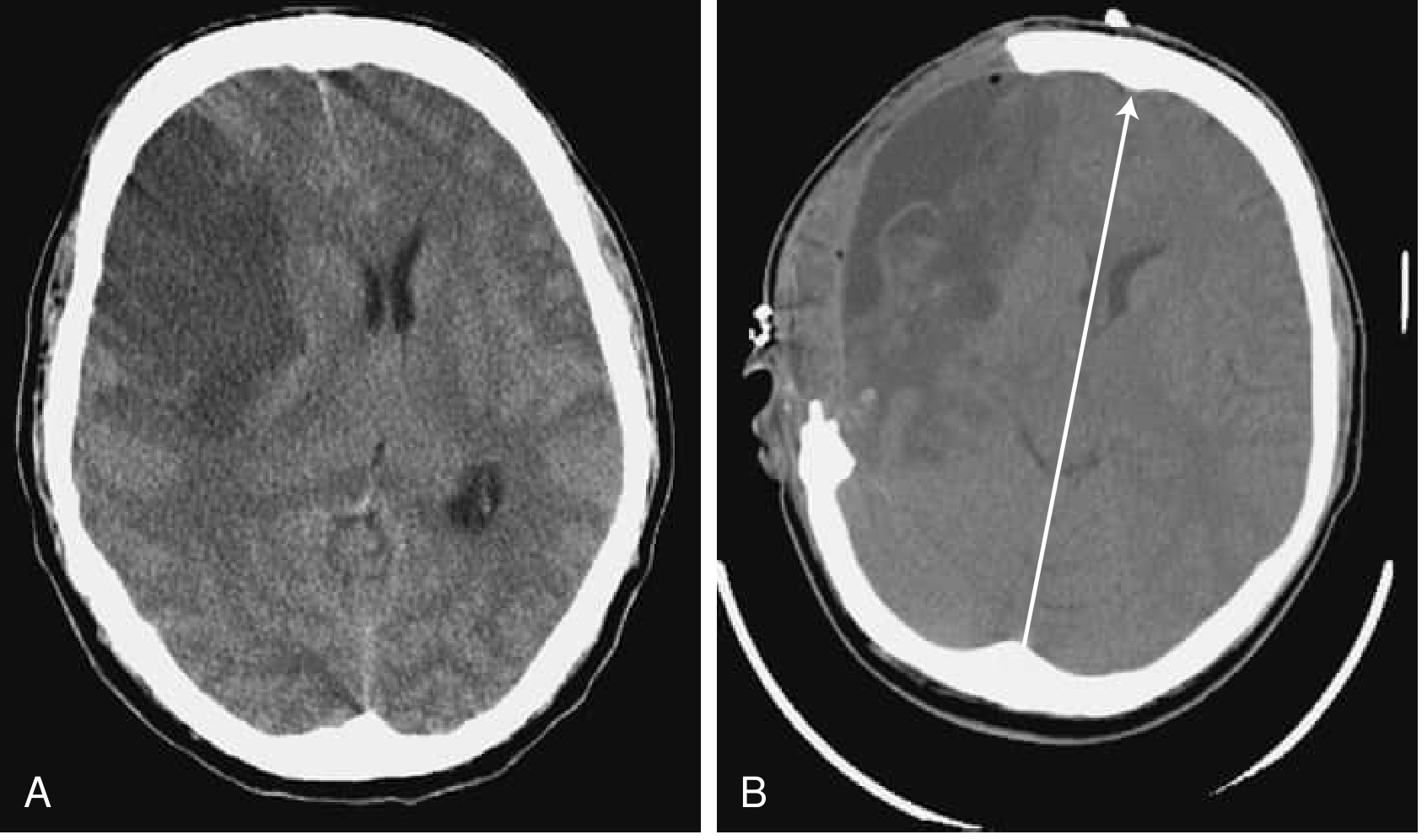
Pre- and post-hemicraniectomy CT - Bradley and Daroff's Neurology in Clinical Practice
6. HEMORRHAGIC STROKE MANAGEMENT
Intracerebral Hemorrhage (ICH)
CT findings: round or oval hyperdense lesion (40-60 HU early, up to 80-100 HU over days).
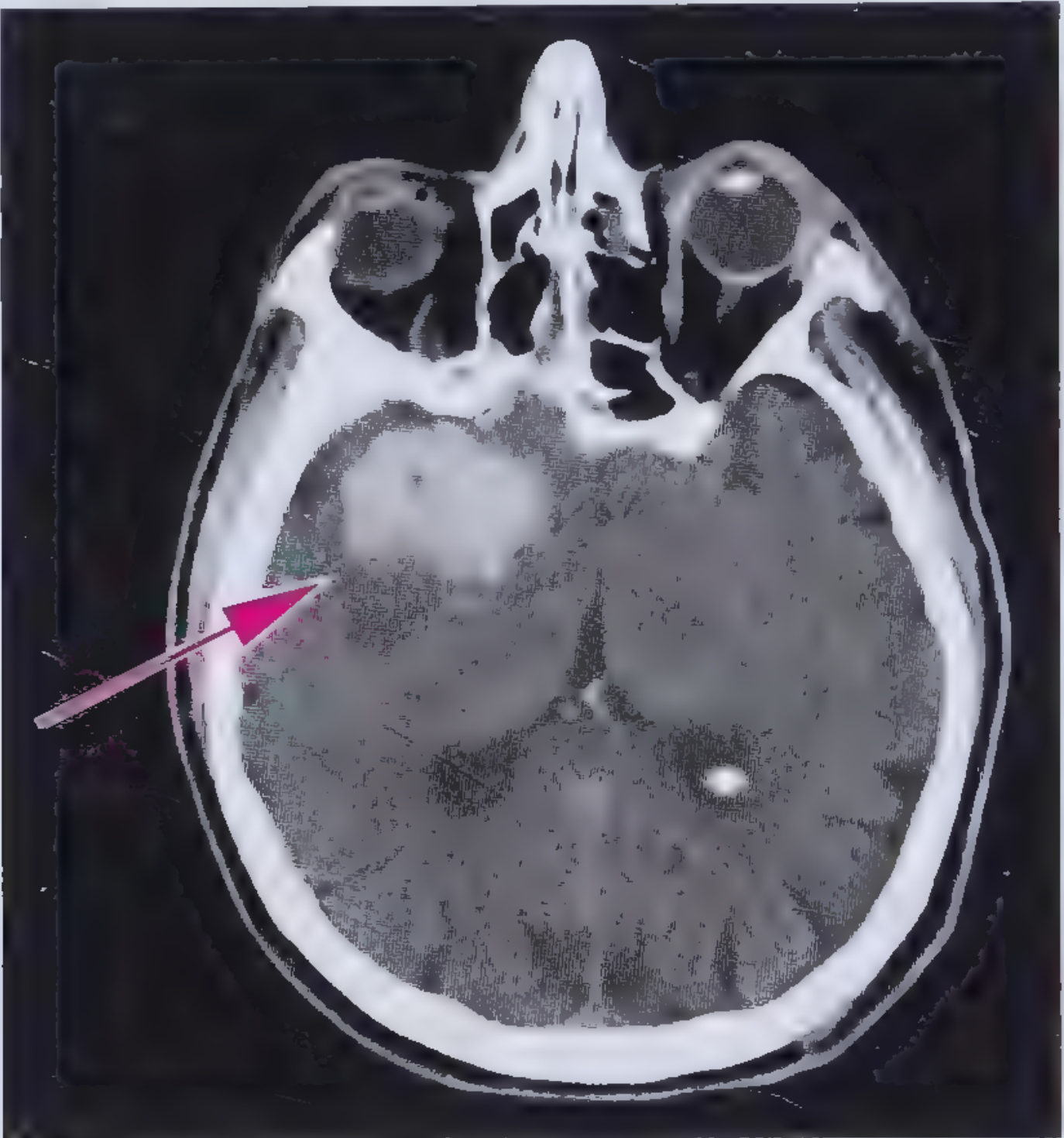
Noncontrast CT: right temporal ICH (arrow) - Frameworks for Internal Medicine
General medical treatment:
- Reverse coagulopathy - correct elevated INR (fresh frozen plasma, vitamin K, prothrombin complex concentrate as indicated)
- Blood pressure control - for SBP 150-220 mmHg, acutely lower to 140 mmHg (safe and effective)
- Glucose - avoid both hyperglycemia and hypoglycemia
- Seizures - treat with antiepileptic drugs
- Raised ICP - intubation/sedation, head elevation, hypertonic fluids, hemicraniectomy if needed
30-day mortality of ICH is nearly 50%.
Risk factors: hypertension (most common), older age, Black/Asian race, high alcohol intake, low LDL/triglycerides, cerebral amyloid angiopathy.
- Frameworks for Internal Medicine
7. PREVENTION OF COMPLICATIONS
| Complication | Prevention |
|---|---|
| Aspiration pneumonia (mortality 15-25%) | NPO until swallowing assessed by speech therapy; head of bed >30 degrees; frequent suctioning |
| DVT / pulmonary embolism | DVT prophylaxis while immobile |
| Pressure ulcers | Early mobilization, nursing care |
| Urinary tract infection | Appropriate catheter care |
| Falls | Bed rest first 24 hours with fall precautions; supervised mobilization |
Head of bed positioning: sitting position did not confer advantage over supine in a 2017 RCT (AVERT trial).
8. SECONDARY PREVENTION
Antiplatelet Therapy
- Aspirin within 48 hours reduces mortality and recurrence (IST and CAST trials) - begin unless tPA was given
- Dual antiplatelet therapy (aspirin + clopidogrel) for 3 weeks after minor stroke/TIA (CHANCE trial) reduces 90-day recurrence without increasing major hemorrhage; extending to 90 days (POINT trial) showed some excess systemic bleeding but still effective
- Not indicated if anticoagulation is planned
Anticoagulation
- Indicated for cardioembolic stroke (especially atrial fibrillation) - DOACs are now preferred over warfarin
- Early anticoagulation after large stroke carries risk of hemorrhagic transformation - defer unless the infarct is small
- Warfarin is not superior to aspirin in non-cardioembolic stroke (WARSS, WASID trials)
- For AF: anticoagulation > aspirin (multiple trials)
Statins
- High-dose statin therapy reduces subsequent stroke by ~2% over 5 years (SPARCL trial)
- Target LDL <70 mg/dL for secondary prevention
Carotid Revascularization
- Carotid endarterectomy or stenting for symptomatic stenosis ≥50-70%
- Intracranial stenting is an option for recurrent stroke despite optimal medical therapy in focal intracranial stenosis
Risk Factor Modification
- Tight blood pressure control (long-term)
- Glycemic control in diabetics
- Smoking cessation
- Anticoagulation for AF
- Pioglitazone may reduce recurrent stroke/MI in insulin-resistant non-diabetic patients (IRIS trial, Kernan 2016)
- Adams and Victor's Principles of Neurology 12e; Fuster and Hurst's The Heart 15e
9. REHABILITATION
- Multidisciplinary team: Neurology, physical therapy, occupational therapy, speech/language therapy, nutrition, social services
- Begin early mobilization as tolerated
- Feeding tube for oropharyngeal dysfunction pending swallow assessment
- Stroke units consistently outperform general wards for functional recovery outcomes
Summary: Time-Critical Actions
| Time | Action |
|---|---|
| 0-10 min | ABC, IV access, glucose, ECG, NIHSS |
| 0-25 min | Non-contrast CT head |
| 0-60 min | "Door-to-needle" target for tPA |
| 0-90 min | CTA for large vessel occlusion |
| <6-24 h | Thrombectomy if eligible |
| 24-48 h | Antiplatelet therapy, statin, swallow assessment |
| Days 2-5 | Peak edema risk, anticoagulation decision for AF |
| Discharge | Long-term secondary prevention plan, rehabilitation |
Recent evidence update (2025): A systematic review and meta-analysis (PMID: 40245349) confirms that endovascular thrombectomy benefits patients with large ischemic core strokes - expanding the pool of eligible candidates beyond earlier, more restrictive criteria.
Management of acute raise of bp ( 150/90 ) before surgery in case of normotensive patient
Finding Sources
Searching PubMed
"perioperative hypertension" AND management
Finding Sources
Finding Sources
Finding Sources
Searching the Web
management acute hypertension 150/90 normotensive patient before surgery anesthesia guidelines 2024
Finding Sources
Reading Web Page
https://www.ahajournals.org/doi/10.1161/CIR.0000000000001356
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://www.urmc.rochester.edu/MediaLibraries/URMCMedia/Anes…
Reading File
Reading File
I now have comprehensive, authoritative content from multiple sources. Here is the full synthesized answer:
Management of Acute Rise in BP (150/90) Before Surgery in a Normally Normotensive Patient
1. First: Understand the Clinical Context
A BP of 150/90 mmHg in a patient who is normally normotensive is a common preoperative scenario. Before doing anything, you must answer three questions:
- Is this a true elevation or white-coat/anxiety hypertension?
- Is there any end-organ damage (hypertensive emergency)?
- Does the degree of elevation actually pose a perioperative risk?
2. The Critical Threshold - Does 150/90 Even Require Action?
This is the most important point, and multiple guidelines agree on it:
A preoperative BP below 180 mmHg systolic / 110 mmHg diastolic has NOT been associated with increased perioperative cardiovascular risk and is NOT an indication to cancel or delay elective surgery.
- BP <180/110: No significant difference in perioperative outcomes vs. normotensives (2025 AHA/ACC Hypertension Guidelines; Morgan & Mikhail's Clinical Anesthesiology 7e)
- DBP <110 is not an independent risk factor for perioperative cardiovascular complications
- The 2024 AHA/ACC perioperative guideline explicitly states: "There is little evidence to defer surgery" for SBP/DBP <180/110 mmHg
So 150/90 in a normally normotensive patient does not require drug treatment, does not justify cancellation, and surgery can proceed after addressing the underlying cause.
- Barash, Cullen, and Stoelting's Clinical Anesthesia 9e; Morgan and Mikhail's Clinical Anesthesiology 7e
3. Step-by-Step Management
Step 1 - Identify the Cause (Rule Out Non-pathological Causes First)
| Cause | Features | Management |
|---|---|---|
| Anxiety / white-coat hypertension | No prior HTN, nervous patient, BP normalizes on reassessment | Reassurance, anxiolytic premedication |
| Pain | Patient in pain pre-op (e.g., fracture, abscess) | Adequate analgesia |
| Urinary retention | Full bladder, discomfort | Catheterize |
| Hypoxia / hypercarbia | SpO₂ low, restlessness | Oxygen, airway management |
| Drug/medication effect | NSAIDs, decongestants, stimulants | Review medication list |
| Undiagnosed chronic hypertension | No prior BP records - "new" finding | Treat as newly diagnosed, see below |
Anesthesia induction itself causes a 20-30 mmHg sympathetic surge in BP in normotensive patients - this is physiological and expected.
- Morgan and Mikhail's Clinical Anesthesiology 7e
Step 2 - Non-pharmacological Measures (First-line for 150/90)
These are sufficient in the vast majority of cases at this BP level:
- Reassurance - address fear and anxiety; calm environment
- Adequate pre-operative analgesia if pain is a contributor
- Anxiolytic premedication - oral midazolam 0.5 mg/kg or IV midazolam 1-2 mg; this alone often normalizes the BP
- Rest - allow 10-15 minutes of supine rest and recheck BP
- Correct reversible factors - full bladder, cold environment, discomfort
- Refer to baseline ambulatory BP - if the patient's home BP readings are normal, this is almost certainly situational
Step 3 - Assess for End-Organ Damage (Rule Out Emergency)
Even at 150/90, briefly screen for signs of a hypertensive emergency (rare at this level but important to exclude):
| Sign | Suggests |
|---|---|
| Chest pain / ST changes | Acute MI / ACS |
| Severe headache, visual changes, confusion | Hypertensive encephalopathy |
| Breathlessness, pulmonary edema | Acute heart failure |
| New focal neurological deficit | Stroke |
| Papilledema | Hypertensive emergency |
| Hematuria, rapidly rising creatinine | Hypertensive nephropathy |
If any end-organ damage is present - this becomes a hypertensive emergency, elective surgery must be cancelled, and IV antihypertensive therapy initiated in ICU. This does not apply at 150/90 in the absence of such features.
Step 4 - Decision: Proceed vs. Postpone
| BP | Recommendation |
|---|---|
| <180/110 (including 150/90) | Proceed with surgery - no evidence to delay, especially for urgent/semi-urgent cases. Address BP postoperatively |
| 180/110 - 180/120 | Exercise clinical judgment; weigh surgical urgency vs. risk; may proceed with IV antihypertensive on standby |
| >180/120 with no end-organ damage (urgency) | Consider short postponement for oral antihypertensive optimization; if surgery is urgent, proceed with IV BP control |
| >180/120 with end-organ damage (emergency) | Cancel elective surgery; IV therapy immediately |
For this patient (150/90), the answer is: proceed after treating the underlying cause (anxiety/pain/etc.).
Step 5 - If Pharmacological Treatment Is Deemed Necessary
This is rarely needed at 150/90 but if there is a compelling reason (e.g., BP remains elevated after all non-pharmacological measures and surgery is high-risk):
Oral / sublingual options (for mild-moderate elevation):
- Oral labetalol 100-200 mg (also has antianxiety properties via beta-blockade)
- Oral amlodipine 5 mg (takes hours to work - not ideal for immediate pre-op use)
- Avoid sublingual nifedipine - causes precipitous, uncontrolled BP drop; dangerous and discouraged by all current guidelines
IV options (for acute control if needed intraoperatively or if >180/110):
| Drug | Dose | Notes |
|---|---|---|
| Labetalol | 10 mg IV over 1-2 min; repeat/double every 10-20 min (max 300 mg) | Alpha + beta blocker; good for most situations |
| Nicardipine | 5 mg/hr IV, titrate to max 15 mg/hr | First-line for most perioperative hypertension per current guidelines |
| Clevidipine | Start 1-2 mg/hr IV; double every 90s; 1 mg/h increase = ~2-4 mmHg SBP reduction | Ultra-short acting (t½ ~1-2 min); ideal for precise titration; safe in hepatic/renal dysfunction - 2025 systematic review confirms efficacy |
| Esmolol | 500 mcg/kg IV bolus, then 50-200 mcg/kg/min infusion | Very short-acting beta-blocker; good during induction/laryngoscopy |
| Nitroglycerin | 5 mcg/min IV, titrate; max 200 mcg/min | Preferred if coronary disease or heart failure is present |
| Sodium nitroprusside | 0.3 mcg/kg/min IV (rarely required) | Avoid if raised ICP; cyanide toxicity risk with prolonged use |
Perioperative hypertension is defined as BP ≥160/90 or SBP elevation ≥20% of preoperative value persisting >15 minutes.
- 2025 AHA/ACC Hypertension Guidelines; 2024 AHA/ACC Perioperative Guideline
4. Intraoperative Considerations
- Patients with preoperative hypertension (even white-coat) are more prone to intraoperative BP lability - both hypertension AND hypotension
- The greatest BP surges occur during induction and laryngoscopy - a 20-30 mmHg systolic rise is expected even in normotensives
- An IV antihypertensive (labetalol or esmolol) should be on standby at induction
- Careful fluid management - avoid hypovolemia, which causes hypotension and then reflex tachycardia
5. Postoperative Plan
- If the elevated preoperative BP was an isolated finding and returns to normal after surgery, no further action is needed acutely
- If BP remains elevated postoperatively, arrange formal outpatient BP monitoring and workup for hypertension (ambulatory BP monitoring, ABPM)
- Address underlying risk factors: obesity, salt, alcohol, physical inactivity
Summary
| Question | Answer |
|---|---|
| Is 150/90 dangerous enough to cancel surgery? | No - threshold is >180/110 |
| Is pharmacological treatment needed? | Usually no - anxiety/pain relief is sufficient |
| What to do first? | Reassure, provide analgesia, premedicate with anxiolytic, recheck BP |
| If drugs are needed? | Oral labetalol or IV nicardipine/labetalol/esmolol |
| Avoid? | Sublingual nifedipine (precipitous drops) |
| Must-rule-out? | End-organ damage (hypertensive emergency) |
This is a shared conversation. Sign in to Orris to start your own chat.