Make notes on hydrocele operation
Reading File
Finding Sources
Searching the Web
hydrocele operation surgical technique types steps
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Finding Sources
Excellent - I have the diagrams and all the key content. Now I have enough information to write comprehensive, well-structured notes. Let me compile them.
Hydrocele Operation - Surgical Notes
Source: Bailey and Love's Short Practice of Surgery, 28th Edition
Definition
A hydrocele is an abnormal collection of serous fluid in a part of the processus vaginalis - usually the tunica vaginalis surrounding the testis, and occasionally along the spermatic cord.
Classification / Types
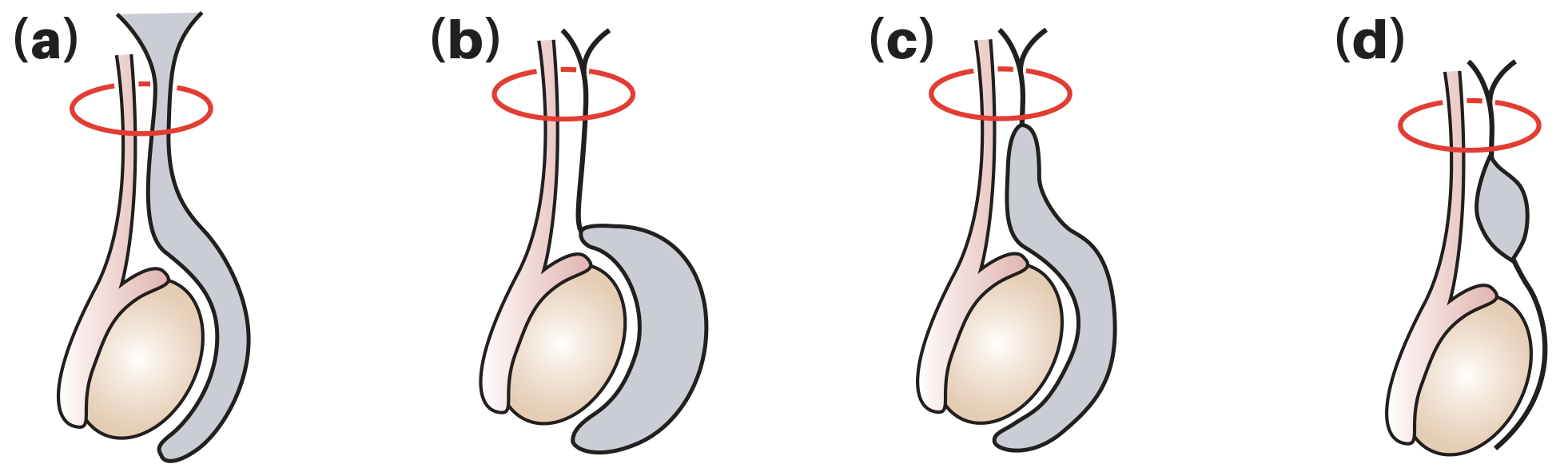
(a) Communicating/vaginal hydrocele (b) Infantile hydrocele (c) Congenital communicating hydrocele (d) Hydrocele of the cord
| Type | Mechanism |
|---|---|
| Communicating (congenital) | Patent processus vaginalis allows flow of peritoneal fluid into the tunica vaginalis; associated with indirect inguinal hernia |
| Non-communicating (vaginal/primary) | Processus vaginalis is closed; fluid accumulates due to excessive production or defective absorption by the tunica vaginalis (often idiopathic) |
| Infantile | Distal end closes but mid-portion of processus remains patent; proximal end open and communicating with tunica |
| Hydrocele of the cord | Both proximal and distal ends closed, mid-portion remains patent forming an isolated cyst |
- Primary hydrocele = non-communicating, most common globally, seen in middle-to-later life
- Secondary hydrocele = men >40 years; caused by local injury, infection, torsion, neoplasm, or radiotherapy
Important: If testicular tumour is suspected, do NOT puncture the hydrocele - risk of malignant needle-track implantation.
Clinical Features
Examine in both upright and supine positions. Ask:
- Can you get above the swelling? - A hydrocele allows palpation of a normal cord above it (unlike an inguinoscrotal hernia)
- Are the testis and epididymis palpable? - A hydrocele encloses them so they may be impalpable
- Does it transilluminate? - Hydroceles are typically translucent (transilluminate brightly)
- Ultrasound is useful in almost all cases to assess testicular pathology
- Congenital hydrocele may be intermittent (fluid drains into peritoneal cavity when lying down)
- Hydrocele of the cord: smooth oval swelling above testis near cord; moves downward and becomes less mobile when testis is pulled down
Indications for Surgery
- Congenital hydrocele: ligation of patent processus vaginalis (herniotomy) if not resolved spontaneously by ~18 months
- Acquired hydrocele: surgical treatment if sizeable and bothersome
- Small hydroceles: conservative management (no treatment needed)
- Surgery can be performed under local anaesthesia
Surgical Approaches
1. Scrotal Approach
- Used for primary/non-communicating hydroceles in adults
- Direct incision over the scrotum
2. Inguinal Approach
- Used for communicating (congenital) hydroceles - ligation of processus vaginalis high at the internal ring
- Required for abdominoscrotal hydroceles to manage abdominal extent
- Preferred approach in children (communicating type)
Operative Techniques (Three Main Methods)
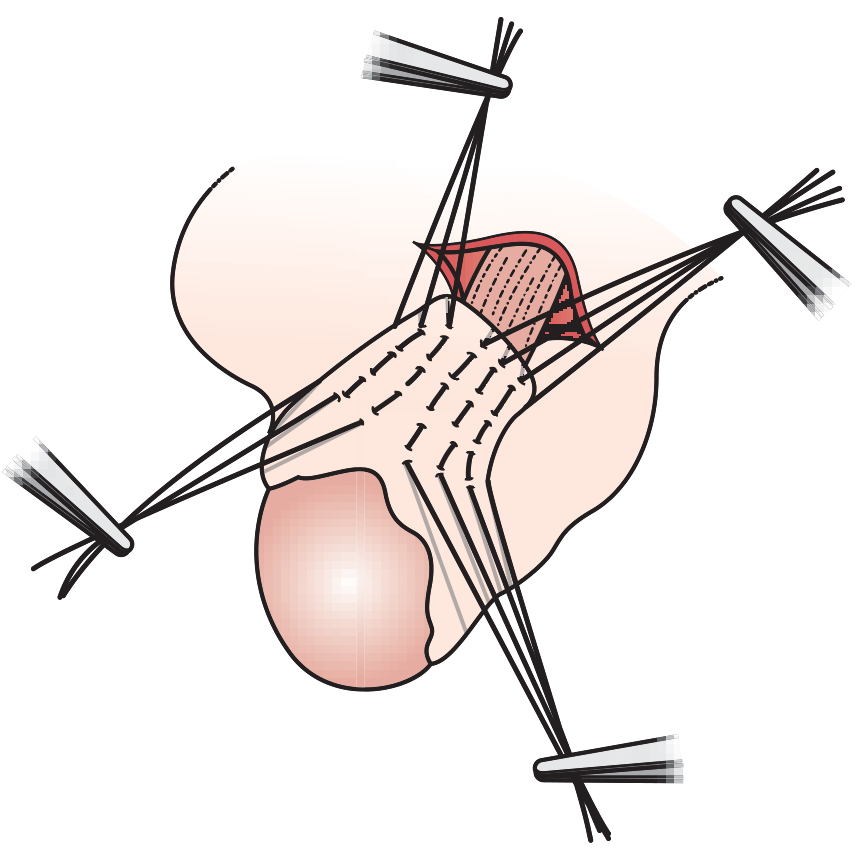
1. Lord's Operation (Plication)
- Indication: Thin-walled hydrocele sac
- Technique:
- Scrotal incision; deliver testis and hydrocele
- Aspirate fluid
- Place multiple interrupted absorbable sutures radially through the sac wall to plicate (bunch) the redundant tunica vaginalis at its attachment to the testis
- When tied, the tunica "bunches" at its testicular attachment
- Advantages: Minimal dissection; reduced risk of haematoma; less bleeding
- Disadvantage: Not suitable for thick-walled sacs
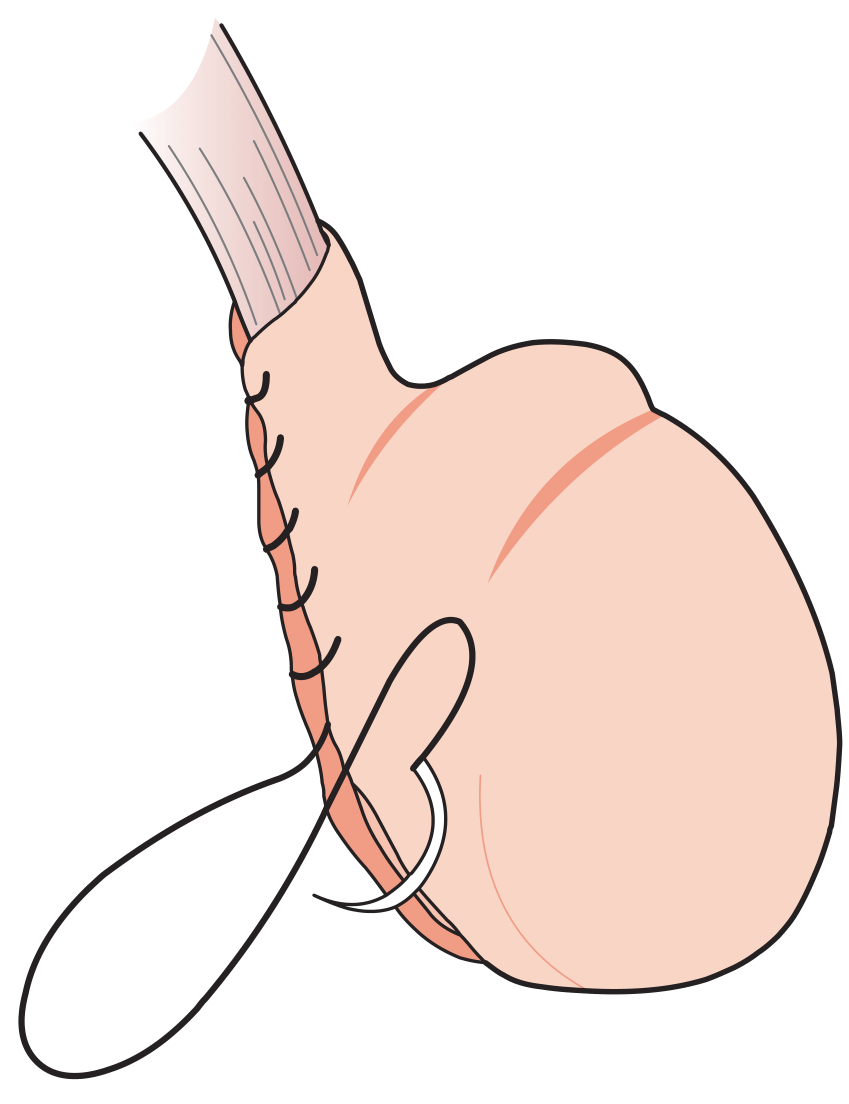
2. Jaboulay's Procedure (Eversion / Bottle Operation)
- Indication: Any hydrocele; especially useful for thin-to-moderate walled sacs
- Technique:
- Scrotal incision; deliver the testis with hydrocele sac
- Aspirate fluid; open the sac anteriorly
- Inspect the testis to exclude pathology
- Evert the sac behind the testis ("like turning a shirt inside-out")
- Anchor the everted sac edges with interrupted absorbable sutures behind the spermatic cord
- Return testis to scrotal pouch (prepared by fascial dissection)
- Advantage: Effective for most hydroceles
- Risk: Haemorrhage from cut sac edges can cause large scrotal haematoma; overrunning stitches at cut edge reduce this risk
3. Excision (von Bergmann / Excision Technique)
- Indication: Large, thick-walled, or multilocular hydroceles
- Technique:
- Deliver testis and hydrocele
- Aspirate fluid; open sac
- Excise the bulk of the hydrocele sac, leaving a narrow collar around the testis/epididymis
- Achieve haemostasis meticulously - oversew the edges of the sac (von Bergmann) or evert residual edges behind the cord (Winkelmann modification)
- Risk: Significant haematoma risk if haemostasis is not meticulous
4. Aspiration (± Sclerotherapy)
- Aspiration alone: fluid always reaccumulates within a week
- Indication: Men unfit for surgery
- Sclerosant injection (e.g., tetracycline): can be effective but painful
- Complication: Bleeding into sac causing haematocele formation
Comparison of Surgical Techniques
| Technique | Wall Type | Key Step | Advantage | Risk |
|---|---|---|---|---|
| Lord's (Plication) | Thin-walled | Radial plication sutures | Minimal dissection, less haematoma | Not for thick sacs |
| Jaboulay (Eversion) | Any | Sac everted behind testis | Simple, effective | Haematoma if edges not oversewn |
| von Bergmann (Excision) | Thick/large/multilocular | Sac excised | Treats difficult sacs | High haematoma risk |
| Aspiration ± sclerosant | Any | Drain fluid | Non-surgical | Recurrence, haematocele |
Complications of Hydrocele Surgery
- Haematoma/haematocele - most common; risk highest with excision technique
- Wound infection
- Recurrence
- Scrotal oedema
- Injury to vas deferens or epididymis - can cause obstruction/infertility
- Testicular atrophy (rare; from vascular injury)
- Post-varicocelectomy hydrocele - incidence 3-33% (average ~7%); due to lymphatic obstruction; managed identically to primary hydrocele
Summary Box
- Hydrocele = fluid collection within the tunica vaginalis
- Surrounds the testis and transilluminates brightly
- Ultrasound is valuable when testis is impalpable
- Treat conservatively unless large and symptomatic
- Surgery is the mainstay of treatment
- Testicular malignancy is an uncommon but important cause - exclude by ultrasound
Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1586-1587
Steps of surgery
Finding Sources
Reading Web Page
https://www.urology-textbook.com/hydrocelectomy.html
Finding Sources
Finding Sources
Reading File
Reading File
I now have detailed step-by-step content from Campbell Walsh Urology. Let me compile the complete operative steps notes.
Hydrocele Operation - Step-by-Step Surgical Notes
Sources: Bailey & Love's Short Practice of Surgery 28th Ed. | Campbell-Walsh-Wein Urology
Pre-operative Preparation
- Position: Supine
- Anaesthesia: General, spinal, or local anaesthesia (scrotal surgery can be done under LA)
- Prophylactic antibiotics: Perioperative dose
- Consent points: Haematoma, infection, recurrence, vas/epididymis injury, infertility, testicular atrophy
Surgical Approach Decision
| Indication | Approach |
|---|---|
| Primary/acquired hydrocele in adults | Scrotal |
| Communicating (congenital) hydrocele in children | Inguinal (ligation at internal ring) |
| Suspected testicular tumour | Inguinal (to avoid scrotal violation) |
| Abdominoscrotal hydrocele | Inguinal (manage abdominal extent) |
| Hydrocele of spermatic cord | Inguinal |
A. Lord's Plication Operation
Best for: thin-walled, small-to-medium hydroceles
Steps:
- Incision - Transverse or longitudinal scrotal incision over the hydrocele
- Dissection - Incise the skin, dartos, and external spermatic fascia layers down to the hydrocele sac; minimal dissection required
- Deliver - Deliver the hydrocele sac into the wound
- Aspirate - Aspirate the hydrocele fluid with a needle or by making a small nick in the sac
- Open sac - Incise the hydrocele sac along its anterior surface; extrude the testis through the aperture
- Inspect - Inspect the testis and epididymis to exclude pathology
- Plication sutures - Place multiple (8-10) interrupted, radially oriented absorbable (chromic catgut) sutures circumferentially through the sac wall; sutures are placed about 1 cm apart from the cut edge towards the testis
- Tie sutures - When tied, the redundant tunica vaginalis bunches up ("pleats") at its attachment to the testis; sac is gathered around the testis like a ruff
- No excision - No tissue is removed; no drain needed (lowest haematoma risk)
- Return testis - Return testis to the scrotum
- Closure - Close the scrotal layers with absorbable sutures; subcuticular skin closure
Key point: No tissue excision = minimal bleeding = least risk of haematoma
B. Jaboulay's Procedure (Eversion / "Bottle Operation")
Best for: thin-to-moderate walled hydroceles; most commonly performed operation
Steps:
- Incision - Transverse scrotal incision
- Dissection - Incise through the scrotal layers (dartos, cremasteric fascia, internal spermatic fascia) to expose the hydrocele sac
- Deliver - Deliver the testis with the intact hydrocele sac into the wound
- Aspirate - Needle aspiration of fluid to decompress the sac before opening
- Open sac - Make an incision into the anterior wall of the tunica vaginalis to open the sac
- Inspect - Thoroughly inspect the testis and epididymis (exclude tumour/epididymitis)
- Excise portion - Resect a portion of the parietal layer of the tunica vaginalis (the excess sac wall), leaving a 1-2 cm margin around the testis/cord
- Haemostasis - Diathermy or suture-ligate all bleeding points on the cut edges meticulously (failure = large scrotal haematoma); overrunning suture (e.g. 3-0 chromic) along cut edges
- Evert the sac - Evert the remaining parietal tunica vaginalis behind the testis and spermatic cord, like turning a bag inside-out ("bottle operation")
- Anchor - Approximate the opposing everted tunical edges to each other behind the cord with interrupted absorbable sutures; ensure the cord is NOT compressed
- Scrotal pouch - Return the testis to the scrotal pouch (prepared by blunt dissection of fascial planes)
- Drain - Consider a small suction drain (corrugated or vacuum) if haemostasis is not perfect; remove at 24-48 hours
- Closure - Close dartos with absorbable sutures; subcuticular skin closure; scrotal support dressing
C. Excision (von Bergmann Technique)
Best for: large, thick-walled, multiloculated hydroceles
Steps:
- Incision - Scrotal incision; wide exposure
- Mobilise - Dissect through all scrotal layers; fully mobilise the hydrocele sac from surrounding tissues
- Deliver - Deliver the entire hydrocele sac into the wound
- Aspirate and open - Aspirate fluid; incise the sac to inspect the testis
- Excise sac - Excise the bulk of the hydrocele sac (parietal tunica vaginalis), leaving only a 1-2 cm collar of sac tissue around the testis and epididymis; do NOT injure the testicular vessels, vas deferens, or epididymis
- Meticulous haemostasis - This step is critical; the cut edge of the thick sac bleeds significantly:
- Von Bergmann: Oversew the cut sac edges with a running absorbable suture for haemostasis
- Winkelmann modification: Evert the residual edges and suture them behind the spermatic cord (combines excision + eversion)
- Drain - Insert a closed suction drain (recommended due to extensive raw surface)
- Return testis and close - Return testis to scrotum; layered closure; firm pressure dressing
D. Window Technique (Less Common)
Steps:
- 4-cm anterior scrotal wall incision
- Blunt dissection to expose the parietal tunica vaginalis
- Stab incision to drain hydrocele fluid
- Create a 2.5 × 2.5 cm cruciate ("window") incision in the parietal tunica
- Evert the four flaps of the cruciate incision
- Stitch each flap with 2-0 chromic suture to maintain the window open
- Close scrotum
E. Bottleneck Technique
- Deliver testis and hydrocele sac
- Trim all but a 2-cm circumferential segment of tunica around the testis and cord
- Tack the tunical edges to each other, leaving the sac open (fluid absorbed by surrounding tissues)
F. Aspiration (± Sclerotherapy)
Only for men unfit for surgery
- Clean the scrotum; local anaesthetic infiltration
- Aspirate hydrocele fluid with a wide-bore needle under aseptic technique
- If sclerotherapy planned: inject sclerosant (e.g. tetracycline, phenol, or polidocanol) into the empty sac
- Apply pressure dressing
- Limitation: Fluid reaccumulates within ~1 week without sclerosant
- Sclerosant is effective but painful; may cause haematocele
G. Herniotomy (Congenital / Communicating Hydrocele in Children)
Inguinal approach steps:
- Inguinal incision over the inguinal canal
- Open the external oblique aponeurosis; expose the inguinal canal
- Identify the patent processus vaginalis (PPV) alongside the cord structures
- Separate the PPV carefully from the vas deferens and testicular vessels
- Ligate the PPV high at the internal inguinal ring (herniotomy)
- The distal sac is left open (not excised - scrotal dissection avoided)
- Repair the inguinal canal; close in layers
Postoperative Care
- Analgesia for 24-48 hours
- Pressure/scrotal support dressing for 24-48 hours
- Scrotal elevation and bed rest
- Drain removal at 24-48 hours (if placed)
- Avoid physical activity / heavy lifting for 2-4 weeks
- Regular wound inspection for signs of haematoma or infection
Complications
| Complication | Incidence | Notes |
|---|---|---|
| Haematoma / haematocele | Up to 10% | Highest with excision technique; meticulous haemostasis is key |
| Wound infection | 3-5% | |
| Recurrence | <5% | Lowest with excision techniques |
| Epididymal duct obstruction | Rare | Can cause infertility |
| Chronic scrotal pain | Rare | |
| Testicular atrophy | Rare | Due to vascular injury |
Campbell-Walsh-Wein Urology | Bailey & Love's Short Practice of Surgery, 28th Ed.
Steps means actually what i do
Finding Sources
Reading Web Page
https://accesssurgery.mhmedical.com/content.aspx?bookid=1755…
Reading File
Reading Web Page
https://www.urology-textbook.com/hydrocelectomy.html
I have all I need. Here is exactly what you physically do, step by step, as the operating surgeon - written as hands-on actions in sequence.
Hydrocele Operation - What You Actually Do
JABOULAY'S PROCEDURE
(Most commonly performed. The standard adult hydrocele operation)
SETUP
- Patient supine
- Shave and prep the scrotum and perineum
- GA / spinal / LA with sedation
- Drape to expose the scrotum
- Give IV antibiotics
STEP 1 - INCISION
- Hold the scrotum taut with your non-dominant hand, pushing the hydrocele anteriorly
- Make a transverse incision (4-5 cm) on the anterior wall of the scrotum, directly over the most prominent part of the hydrocele
- Cut cleanly through skin only first
STEP 2 - DEEPEN THROUGH LAYERS
Cut through each layer in sequence:
- Skin
- Dartos muscle (thin, reddish, bleeds - diathermy as you go)
- External spermatic fascia
- Cremasteric muscle and fascia
- Internal spermatic fascia
You will now see the bluish-white, tense tunica vaginalis (the hydrocele sac wall) bulging into the wound.
STEP 3 - DELIVER THE SAC
- Using blunt dissection (fingers or gauze), dissect the sac free from the surrounding scrotal tissue all around
- Grip the sac with tissue forceps and deliver the entire hydrocele sac out of the scrotum into the wound - it should come out looking like a smooth, pale, tense balloon
- The testis is inside the sac and cannot be felt yet
STEP 4 - ASPIRATE THE FLUID
- With a needle and syringe, aspirate the fluid from the sac to decompress it - or proceed directly to incision
- The sac collapses and becomes flabby
STEP 5 - OPEN THE SAC
- Pick up the anterior wall of the tunica vaginalis with tissue forceps
- Make a small nick with a scalpel
- Extend the incision with scissors along the anterior face of the sac - cut it open widely
- Remaining fluid drains out
STEP 6 - INSPECT THE TESTIS
- Deliver the testis and epididymis out through the opening
- Look carefully - feel and inspect the testis, epididymis, and cord for any:
- Tumour
- Epididymo-orchitis
- Torsion
- Gumma
- If any suspicious lesion - stop, do NOT proceed; plan radical orchidectomy via inguinal route
STEP 7 - EXCISE THE SAC
- Cut away the bulk of the hydrocele sac (parietal tunica vaginalis) with scissors
- Leave a 1-2 cm cuff/collar of sac around the testis and epididymis - do NOT trim right up to the epididymis (risk of injury)
- Do NOT cut the vas deferens, testicular vessels, or epididymis
- You are left with a small collar of tunica around the testis and a large excised piece of sac
STEP 8 - HAEMOSTASIS (CRITICAL STEP)
- The cut edge of the sac bleeds - control every bleeding point
- Use diathermy on individual vessels
- Run a continuous absorbable suture (3-0 chromic catgut or Vicryl) along the entire cut edge to oversew it - this is the von Bergmann step
- This step prevents haematoma - take your time here
STEP 9 - EVERT THE SAC (Jaboulay Step)
- Take the remaining collar of tunica and fold/evert it behind the testis and spermatic cord - like turning a shirt inside-out, so the raw surface faces outward
- Bring the two cut edges of the collar together behind the cord
- Stitch them together with interrupted 2-0 or 3-0 absorbable sutures - make sure the cord is not compressed at all
STEP 10 - RETURN THE TESTIS
- Gently push the testis back down into the scrotal pouch
- The testis should sit comfortably with its everted tunica behind it
STEP 11 - DRAIN (Optional)
- If there was any oozing or extensive dissection, place a small corrugated or suction drain through a separate stab incision inferiorly in the scrotum
- Bring it out and fix with a suture
- Remove at 24-48 hours
STEP 12 - CLOSE IN LAYERS
- Dartos - close with continuous 2-0 Vicryl (closes the deep dead space)
- Skin - close with 3-0 Vicryl rapide subcuticular or interrupted sutures
- Apply a firm scrotal support dressing (fluffed gauze + snug underwear/jockstrap)
LORD'S PLICATION
(For thin-walled, smaller hydroceles - quicker, less bleeding)
| Step | What you do |
|---|---|
| 1. Incision | Same scrotal incision as above |
| 2. Layers | Cut through same layers to reach the sac |
| 3. Aspirate | Aspirate fluid through a needle in the sac |
| 4. Small opening | Make a small incision in the anterior sac wall - just big enough to deliver the testis through |
| 5. Deliver testis | Squeeze the testis out through the small hole; it sits in the wound with the sac gathered around it |
| 6. Inspect | Look at testis and epididymis |
| 7. Plication sutures | Place 8-12 interrupted chromic catgut sutures radially, each picking up a 1 cm bite of the sac wall, from the cut edge inward toward the testis - placed all around the circumference like spokes of a wheel |
| 8. Tie sutures | Tie each suture - the sac gathers and bunches up ("pleats") at the testis like a ruff collar |
| 9. No excision, no drain | Nothing is removed; no drain needed |
| 10. Return and close | Return testis; close dartos and skin as above |
The sac is NOT excised - just gathered up so it cannot re-expand - that's why haematoma risk is lowest with this method.
HERNIOTOMY (Congenital Hydrocele in Children)
(Inguinal approach - you are ligating the processus vaginalis, not operating on the sac itself)
| Step | What you do |
|---|---|
| 1. Incision | Groin crease incision (inguinal) - 2-3 cm, just above and medial to the internal ring |
| 2. Open external oblique | Cut through external oblique aponeurosis along the direction of fibres; expose the inguinal canal |
| 3. Find the cord | Identify the spermatic cord at the internal ring |
| 4. Find the processus | Identify the patent processus vaginalis - a thin-walled sac running anterior to the cord structures |
| 5. Separate | Carefully separate the processus vaginalis off the vas deferens and testicular vessels using blunt dissection (they are stuck together) - this is the delicate part |
| 6. Ligate high | Transfixion-ligate (double ligation) the processus vaginalis as high as possible at the internal inguinal ring using absorbable suture |
| 7. Divide | Divide the processus below the ligation |
| 8. Leave distal sac | Leave the distal sac open in the scrotum - do NOT go into the scrotum to excise it |
| 9. Close canal | Repair the inguinal canal; close external oblique, Scarpa's fascia, and skin |
WHAT NOT TO DO (Pitfalls)
- Do NOT puncture a hydrocele if testicular tumour is suspected - malignant track seeding
- Do NOT ligate or compress the spermatic cord when everting the sac
- Do NOT trim the sac flush with the epididymis - leave a 1-2 cm cuff
- Do NOT ignore bleeding at the sac edge - meticulous haemostasis prevents haematoma
- Do NOT leave a closed distal sac after herniotomy - it will form a new hydrocele
Campbell-Walsh-Wein Urology | Bailey & Love's Short Practice of Surgery, 28th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.