Pain Pathway
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-illustrated textbook content from Neuroscience: Exploring the Brain, 5th Edition to provide a thorough answer. Here is the complete pain pathway:
The Pain Pathway (Nociception)
Pain is a protective sensation mediated by a dedicated neural system. It follows a sequence of four key stages: transduction → transmission → modulation → perception.
1. Peripheral Nociceptors and Transduction
Pain begins at free nerve endings (nociceptors) distributed throughout the skin, bone, muscle, most internal organs, blood vessels, and meninges. They are absent from brain parenchyma itself. Nociceptors respond to noxious mechanical, thermal, and chemical stimuli.
When tissue is damaged, a mixture of chemicals called the "inflammatory soup" is released around nociceptors. These include:
- Bradykinin - directly depolarizes nociceptors via specific receptors
- Prostaglandins - sensitize nociceptors (do not cause pain alone but amplify the response)
- ATP - activates purinergic receptors on nociceptors
- K+ - directly depolarizes neuronal membranes
- Serotonin, glutamate, histamine (from mast cells)
- Substance P and CGRP - neuropeptides released by nociceptors themselves, causing vasodilation and secondary hyperalgesia
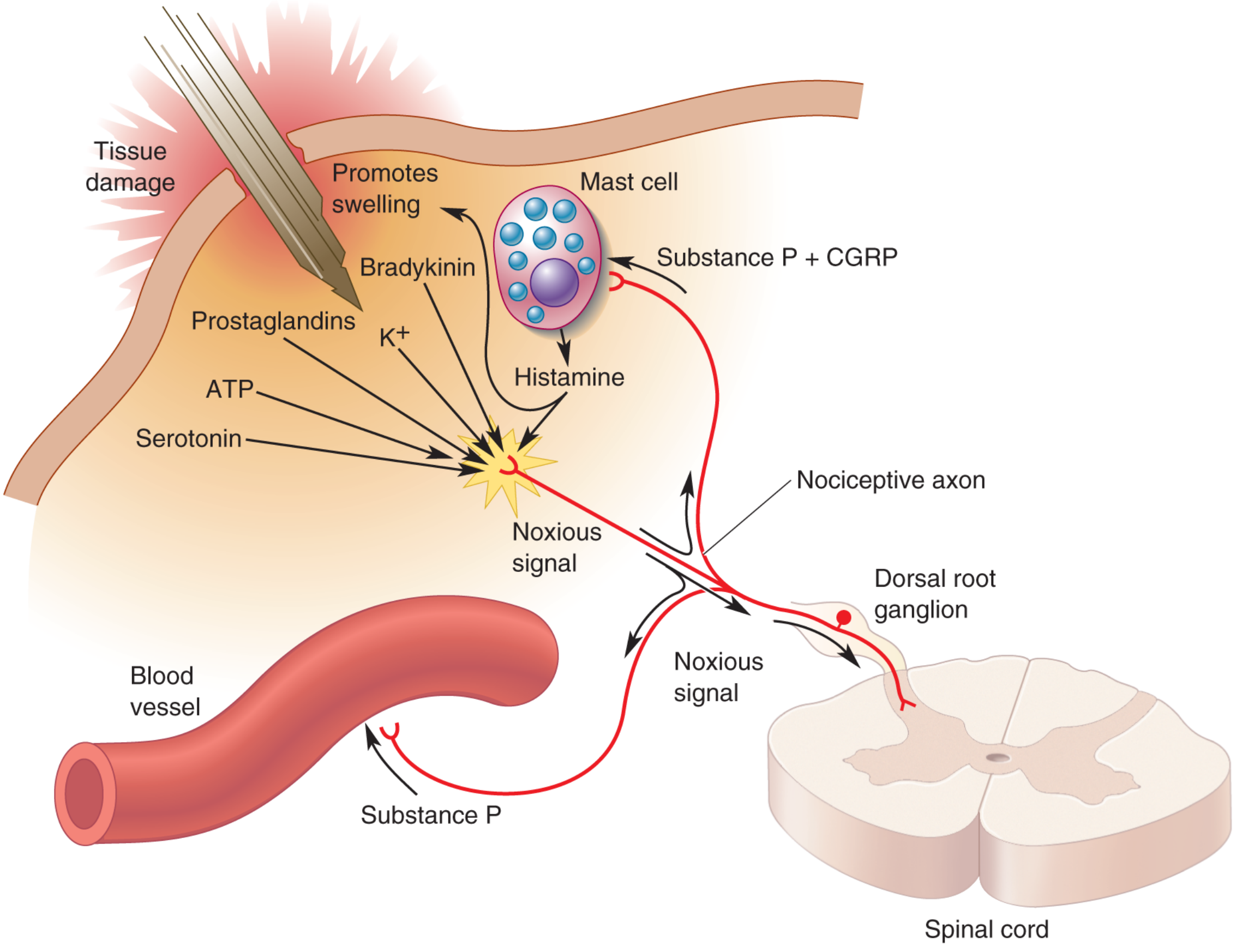
Figure 12.27: Peripheral chemical mediators of pain - Neuroscience: Exploring the Brain, 5e
2. Primary Afferent Fibers (1st-Order Neurons)
Two fiber types carry nociceptive signals from periphery to spinal cord:
| Feature | A-delta (Aδ) fibers | C fibers |
|---|---|---|
| Myelination | Lightly myelinated | Unmyelinated |
| Conduction velocity | ~5-30 m/sec | ~0.5-2 m/sec |
| Pain quality | First pain: sharp, fast, pricking | Second pain: slow, burning, aching, prolonged |
| Sensation | Acute localized pain | Dull, diffuse, persistent pain |
Both fiber types have their cell bodies in the dorsal root ganglia (DRG). Their axons enter the spinal cord via the dorsal root, branch immediately, travel a short distance up and down in the zone of Lissauer (outermost spinal layer), and then synapse in the substantia gelatinosa (Rexed laminae I and II of the dorsal horn).
3. Spinal Cord Synapses (2nd-Order Neurons)
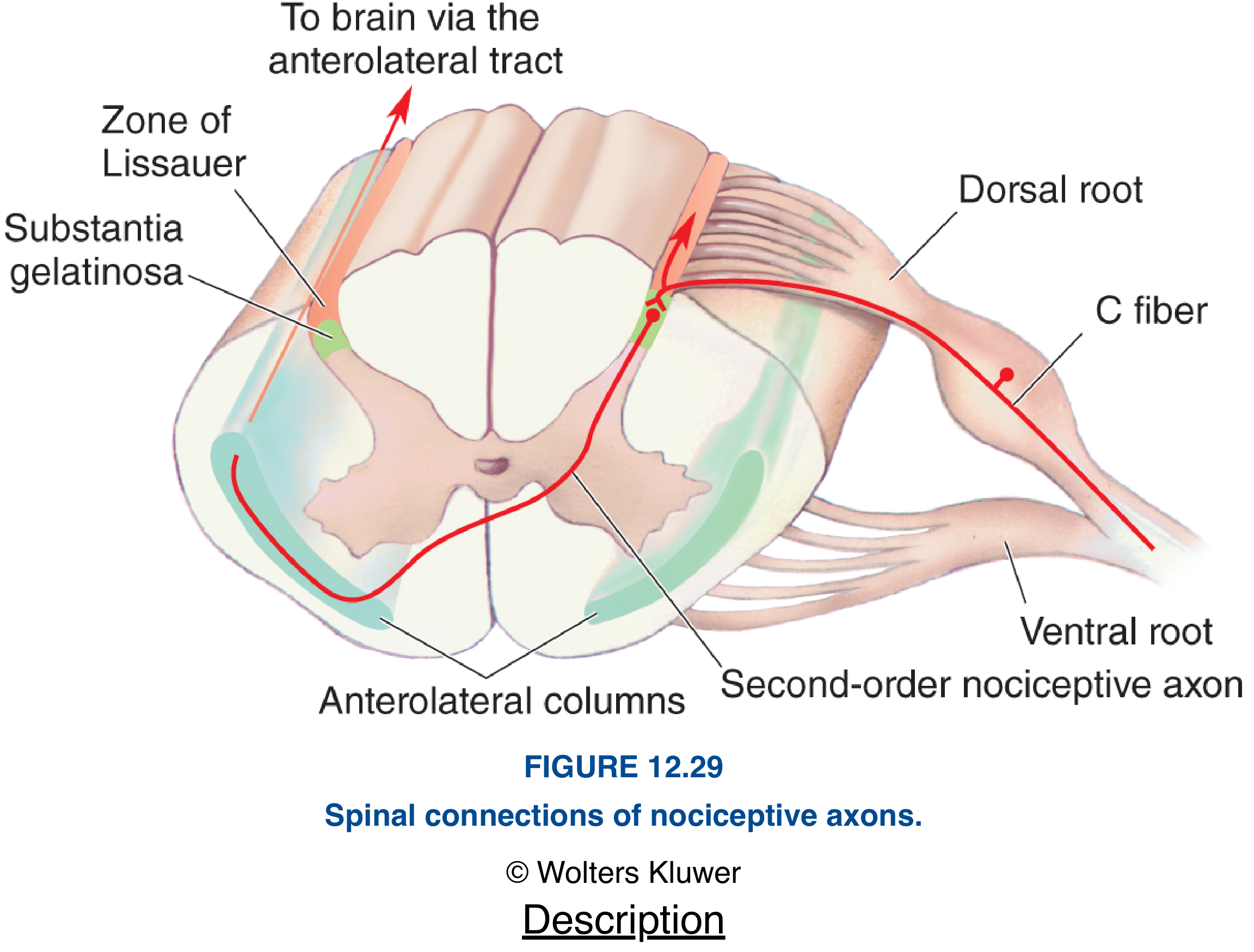
Figure 12.29: Spinal connections of nociceptive axons - Neuroscience: Exploring the Brain, 5e
The primary afferents synapse on second-order neurons in the dorsal horn. The main neurotransmitters released here are:
- Glutamate - primary fast excitatory transmitter
- Substance P (from dense core vesicles) - released by high-frequency trains; sensitizes postsynaptic neurons to glutamate; required for moderate-to-intense pain
The axons of the second-order neurons immediately decussate (cross the midline) through the anterior commissure and ascend in the anterolateral tract (ventral surface of spinal cord). This is the key distinction from touch pathways, which ascend ipsilaterally via the dorsal columns.
4. Ascending Pain Pathway - The Anterolateral (Spinothalamic) System
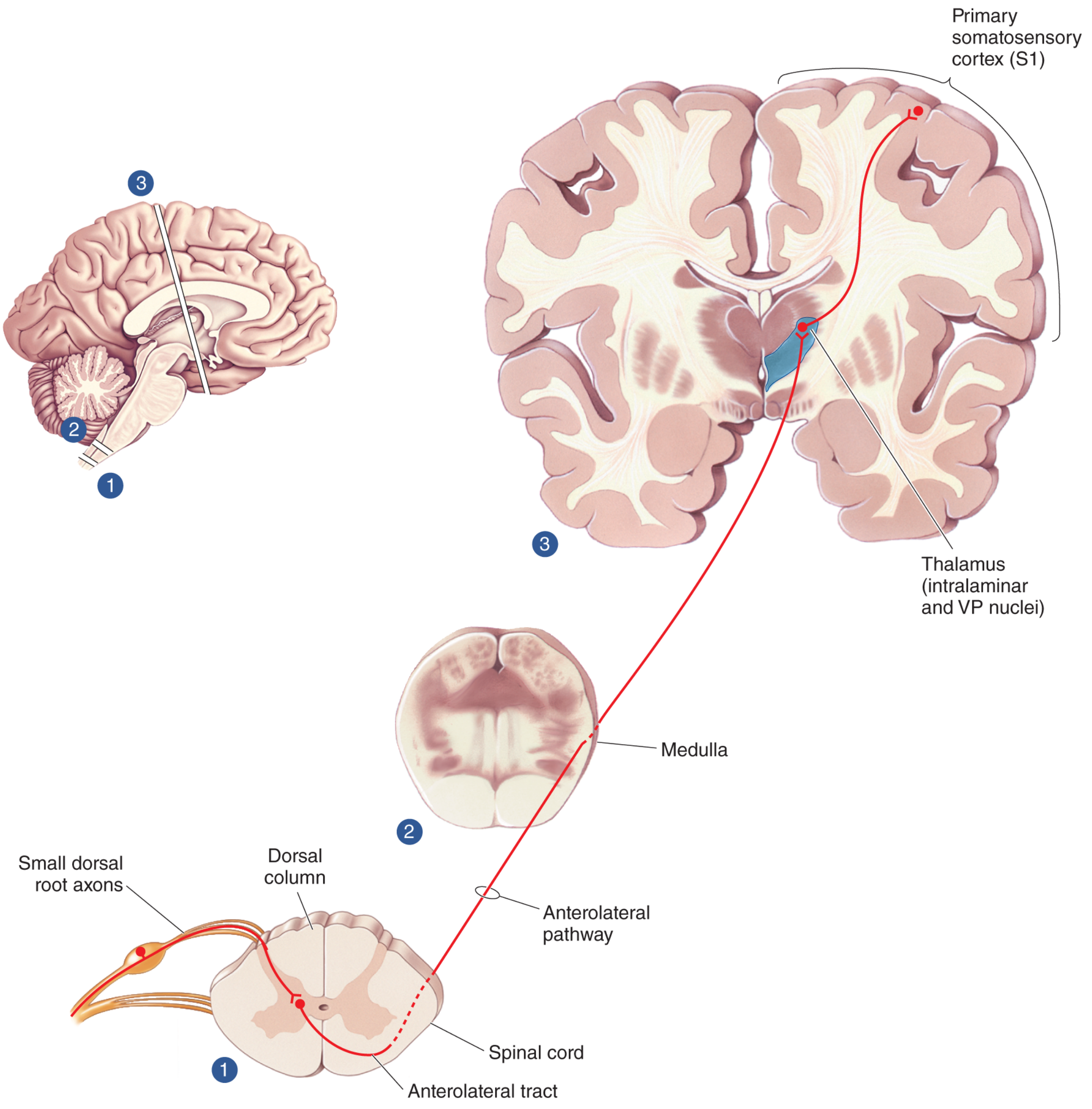
Figure 12.31: The anterolateral (spinothalamic) system - Neuroscience: Exploring the Brain, 5e
The crossed axons ascend through the anterolateral tract without synapsing, passing through the medulla, pons, and midbrain, and eventually projecting to the thalamus. The axons terminate in:
- The ventral posterior (VP) nucleus of the thalamus - same nucleus as touch afferents, but in a separate region
- The intralaminar nuclei of the thalamus - projects widely, involved in arousal and the affective/emotional dimension of pain
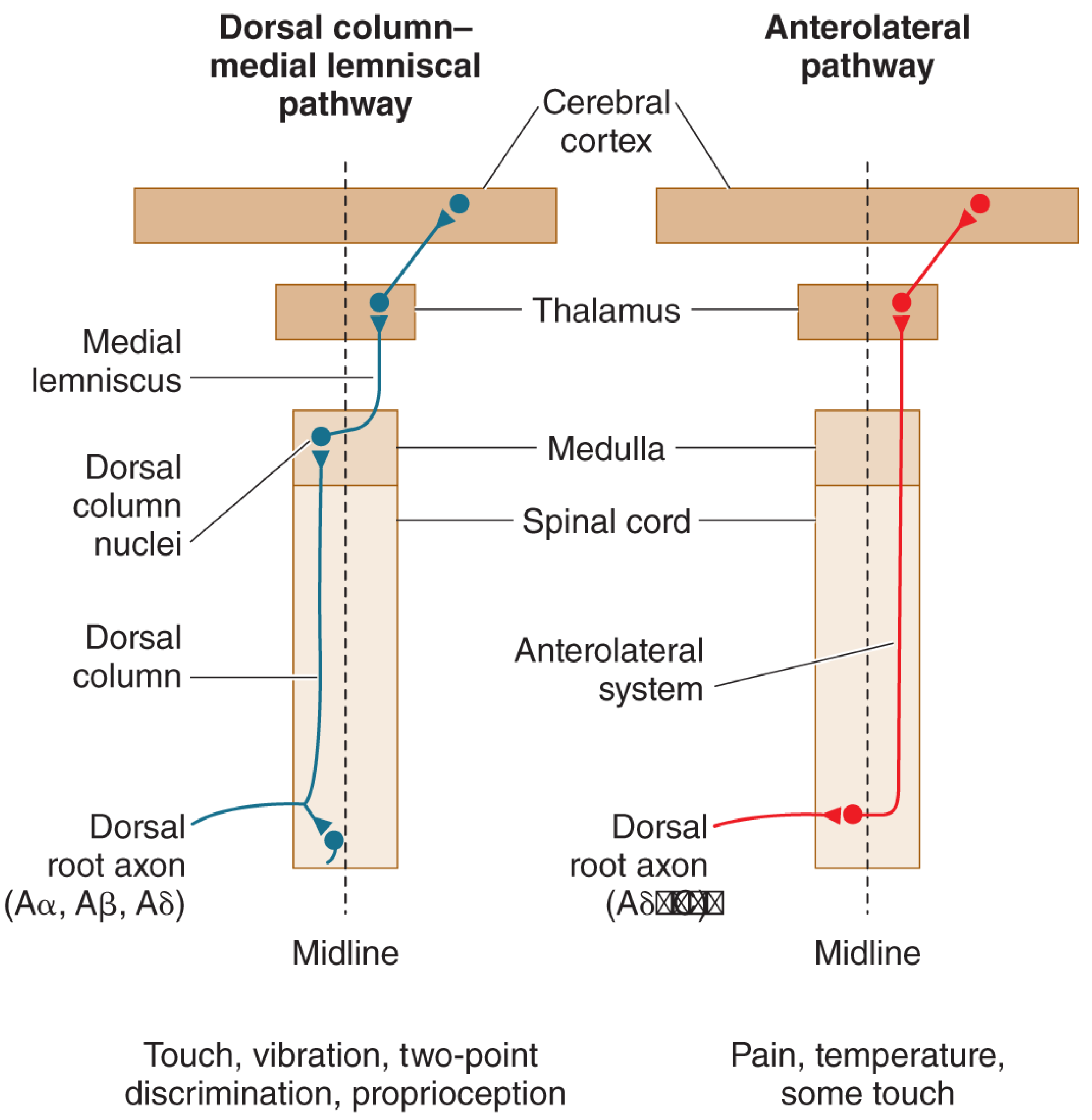
Figure 12.32: The two major ascending pathways - dorsal column (touch) vs. anterolateral (pain) - Neuroscience: Exploring the Brain, 5e
5. Trigeminal Pain Pathway (Face and Head)
Pain from the face and head follows an analogous route. Small-diameter fibers in the trigeminal nerve (CN V) synapse first in the spinal trigeminal nucleus of the brainstem (an extension of the substantia gelatinosa). Second-order axons cross the midline and ascend to the thalamus via the trigeminal lemniscus.
6. Thalamus to Cortex (Perception)
From the thalamus, pain information projects to a wide expanse of the cerebral cortex. Cortical areas involved include:
- Primary somatosensory cortex (S1) - localizes the pain and encodes its intensity
- Secondary somatosensory cortex (S2) - further processing
- Anterior cingulate cortex, insular cortex - emotional and autonomic responses to pain (the "suffering" component)
Pain has a broader cortical representation than touch.
7. Modulation - The Gate Control Theory
Pain signals can be modulated at the dorsal horn by the balance of input from large (Aβ) and small (Aδ/C) fiber activity. In Melzack and Wall's gate control theory:
- Aβ (touch) fiber activation → excites inhibitory interneurons in the dorsal horn → "closes the gate" → reduces nociceptive transmission
- C fiber (nociceptive) activation → inhibits those interneurons → "opens the gate" → increases pain signal transmission
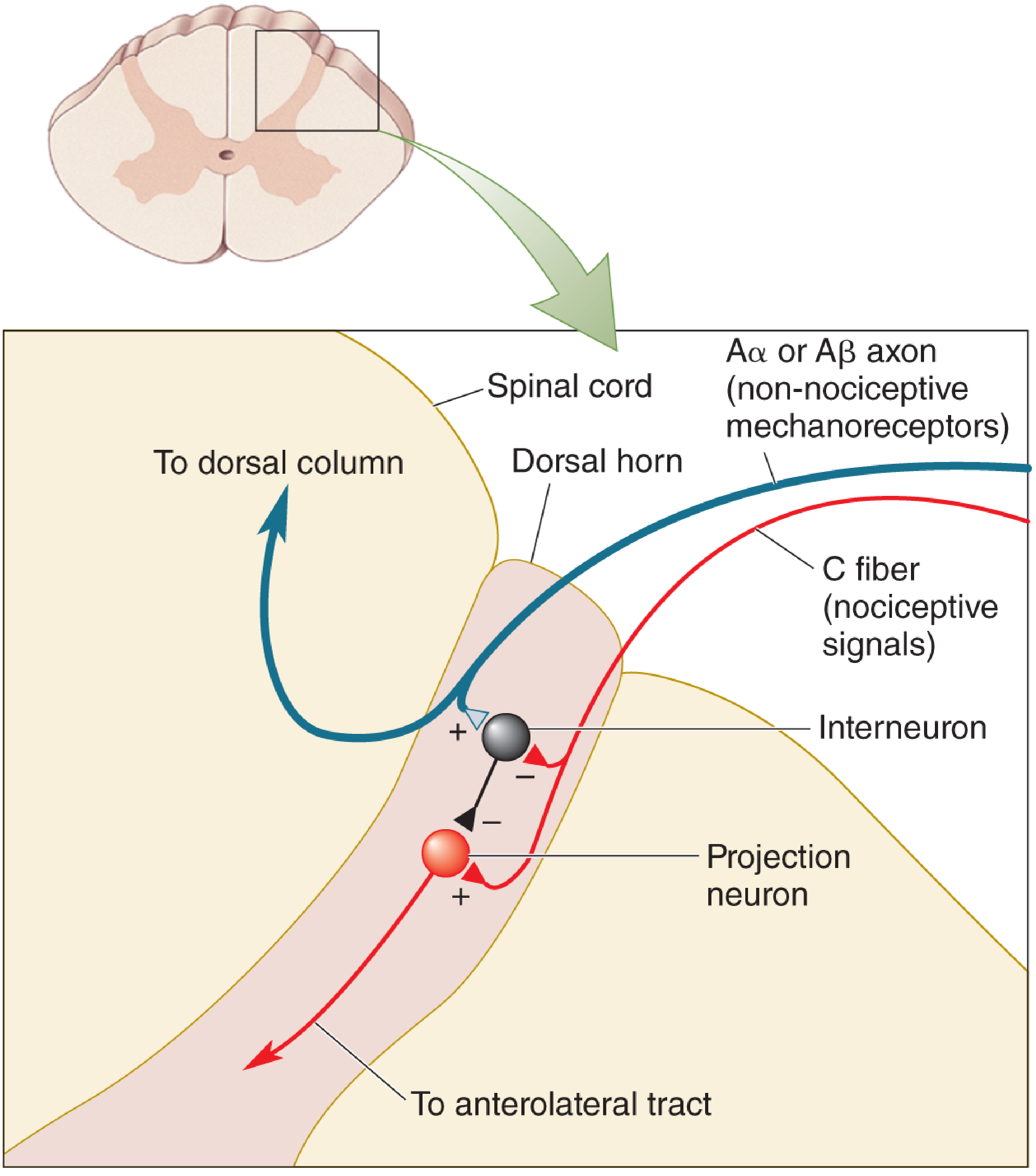
Figure 12.34: Melzack and Wall's gate control theory - Neuroscience: Exploring the Brain, 5e
This explains why rubbing an injured area reduces pain, and forms the basis for TENS (transcutaneous electrical nerve stimulation).
8. Descending Pain Control
Pain is also regulated from above via a descending inhibitory pathway:
- Periaqueductal gray (PAG) of the midbrain - key relay; receives input from the cortex, hypothalamus, and amygdala. PAG stimulation produces profound analgesia.
- Raphe nuclei of the medulla (serotonin) and locus coeruleus (norepinephrine) - receive PAG output
- These nuclei project back down to the dorsal horn and suppress nociceptive neuron activity
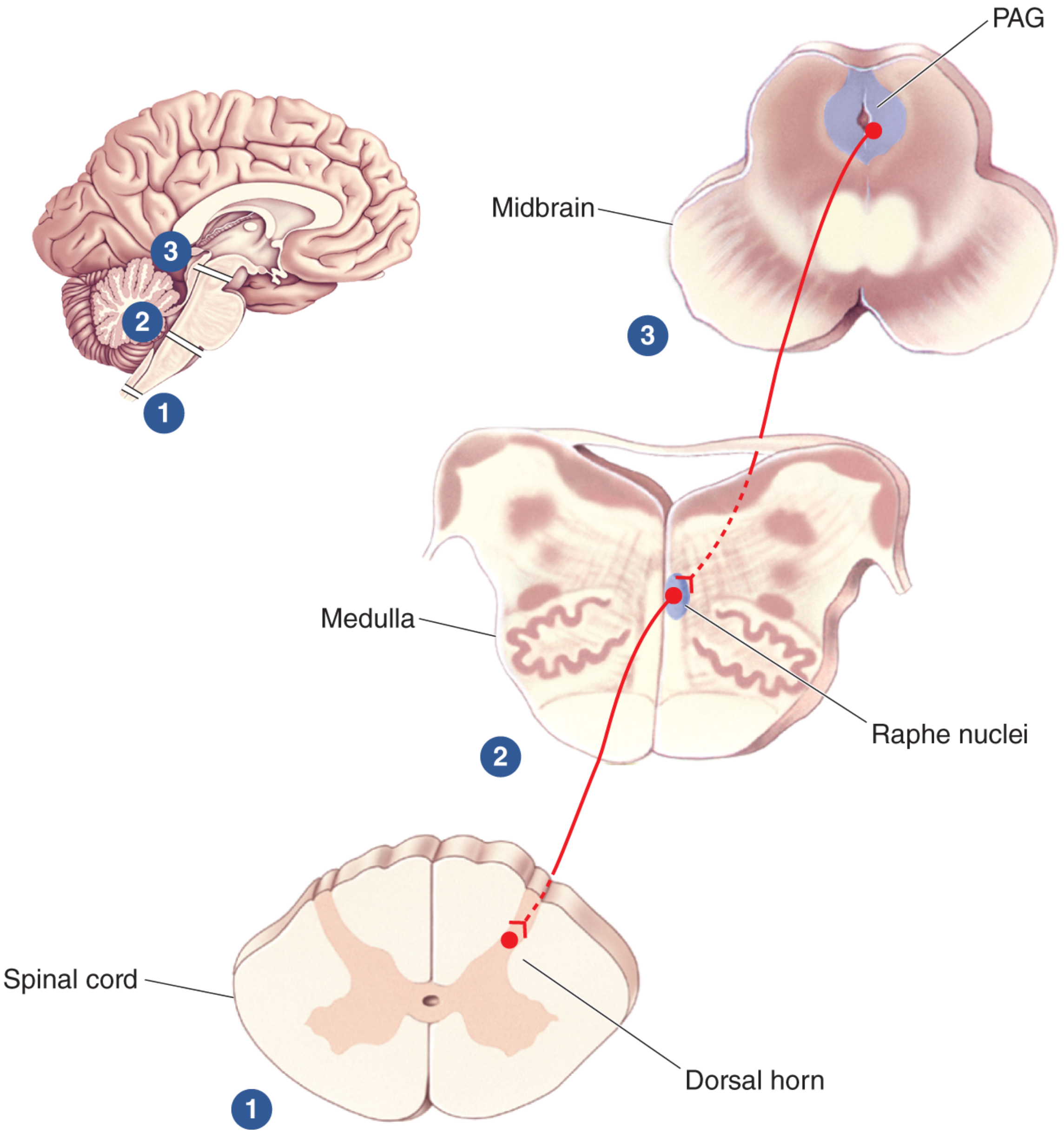
Figure 12.35: Descending pain control via PAG - Neuroscience: Exploring the Brain, 5e
Endogenous opioids (endorphins, enkephalins, dynorphins) are the key neuromodulators in this descending system. They are concentrated in areas that process nociceptive information and provide the biochemical basis for opioid analgesia.
Summary: The 3-Neuron Pain Pathway
| Neuron | Location | Tract |
|---|---|---|
| 1st order | Peripheral tissue → DRG → dorsal horn | Free nerve endings → A-delta/C fibers |
| 2nd order | Dorsal horn → crosses midline → thalamus | Anterolateral (spinothalamic) tract |
| 3rd order | Thalamus → cerebral cortex | Thalamocortical projections |
Key clinical correlate: Because pain fibers cross at the spinal cord level (vs. touch fibers that cross in the medulla), spinal cord hemisection produces ipsilateral loss of touch but contralateral loss of pain and temperature - the hallmark of Brown-Séquard syndrome.
Source: Neuroscience: Exploring the Brain, 5th Edition - Chapters on somatic sensation and pain pathways
This is a shared conversation. Sign in to Orris to start your own chat.